
Abstract
Introduction:
Fluoroscopy with retrograde pyelogram is commonly used to obtain access for percutaneous nephrolithotomy (PNL). Our practice uses room air for retrograde identification of calyceal anatomy. Herein we explore whether an air pyelogram was associated with a decrease in radiation exposure compared with standard retrograde pyelogram.
Methods:
We retrospectively reviewed all PNL procedures performed at our institution over the past 2 years. Of the 260 PNL procedures performed during the study period, 96 had information on radiation dosage required for analysis. The effective dose (ED) was calculated using accepted conversion tables. Multivariable linear regression was used to determine the association between ED and the use of air pyelogram controlling for factors thought to affect radiation exposure.
Results:
Of the 96 PNL procedures included in the study, 60 (63%) were performed with an air retrograde pyelogram (AP) and 36 (37%) used contrast retrograde pyelogram (CP). Both groups were matched in terms of age, body mass index, stone burden, and number of access tracts. Multivariable linear regression showed significantly lower radiation exposure in the AP group than in the CP group (p = 0.001). There was no difference in fluoroscopy time between the two groups. Using an AP lowered the mean adjusted ED nearly twofold, from 7.67 (CI = 5.99–9.81) to 4.45 (CI = 3.68–5.38) mSv.
Conclusions:
An air retrograde pyelogram is associated with decreased radiation exposure during PNL when compared with a contrast retrograde pyelogram.
Introduction
Fluoroscopy during PNL contributes to cumulative radiation exposure for patients with nephrolithiasis. We evaluated whether the use of air for performance of a retrograde pyelogram affected radiation exposure during PNL when compared with the use of a contrasted retrograde pyelogram.
Methods
After obtaining Institutional Review Board approval, we retrospectively reviewed all PNL procedures performed by a single surgeon (G.M.P.) and interventional radiologist (M.J.M.) at our institution from November 2007 to April 2009. Of the 260 PNL procedures that were performed, a total of 96 patients with data on their radiation dosage during PNL were included for analysis.
Radiation dosage was recorded in a dose report from the intraoperative C-arm, (General Electric OEC 9800 Elite; General Electric, Waukesha, WI). The radiation dose measured included all radiation exposure during percutaneous access, wire placement, tract dilation, stone removal, and drainage tube placement. Radiation exposure during the cystoscopic placement of the external ureteral catheter was not included. The dose report included fluoroscopy time and a dose area product expressed in rads · cm2. The effective dose (ED) was calculated using accepted conversion tables, converting rads · cm2 to mSv. 1
Demographic and intraoperative characteristics of the patients were recorded. Stone burden was measured from preoperative noncontrast computed tomography (NCCT) or intravenous pyelogram and was defined as the greatest cross-sectional area of the stone viewed anteroposteriorly (expressed in cm2). Preoperative NCCT or intravenous pyelogram were also used to determine stone location and configuration, including whether or not the stone crossed an infundibulum. A stone was considered branched if it involved either the renal pelvis and a calyx or multiple calyces. The presence or absence of hydronephrosis was also determined from preoperative imaging. The number of percutaneous access tracts required during the procedure was recorded. In cases where the patient presented to the operating room with a percutaneous nephrostomy tube already in place, a value of zero was recorded in the data field. The operative reports and intraoperative images were reviewed to determine if air or contrast was used to perform the retrograde pyelogram.
Surgical technique
After induction of general anesthesia, the patient undergoes cystoscopy and placement of an open-ended ureteral catheter. The patient is placed prone on the operating room table. Access is obtained under fluoroscopic guidance with a portable C-arm (General Electric OEC 9800 Elite; General Electric). The stone is observed using fluoroscopy and 5–10 cc of room air is injected via the open-ended ureteral catheter (Fig. 1). This technique allows for delineation of the collecting system anatomy and identification of the preferred calyx for puncture. After skin incision, an 18-guage needle is placed percutaneously into the collecting system under fluoroscopic guidance. A 0.038 in Sensor Guidewire (Boston Scientific, Natick, MA) is placed through the needle and down the ureter under fluoroscopic guidance. After placement of a second (safety) guidewire, a 30F balloon dilator (Nephromax-Boston Scientific, Marlborough, MA) is placed over the working wire and inflated with dilute Isovue contrast to a pressure of 22 cm H2O. Fluoroscopy is used to confirm appropriate positioning of the balloon and to confirm complete inflation. A 30F percutaneous access sheath is placed over the inflated balloon and its position confirmed with fluoroscopy. The C-arm is moved away and intracorporeal lithotripsy is performed via standard techniques through a rigid nephroscope. At the completion of stone fragmentation and removal, the collecting system is inspected with a flexible nephroscope to assess for residual fragments. Fluoroscopy is used to confirm complete stone removal. Additional fluoroscopic images are obtained depending on the type of drainage used. In cases where a nephrostomy tube or an internal ureteral stent are placed, additional fluoroscopic images are obtained to ensure appropriate positioning.
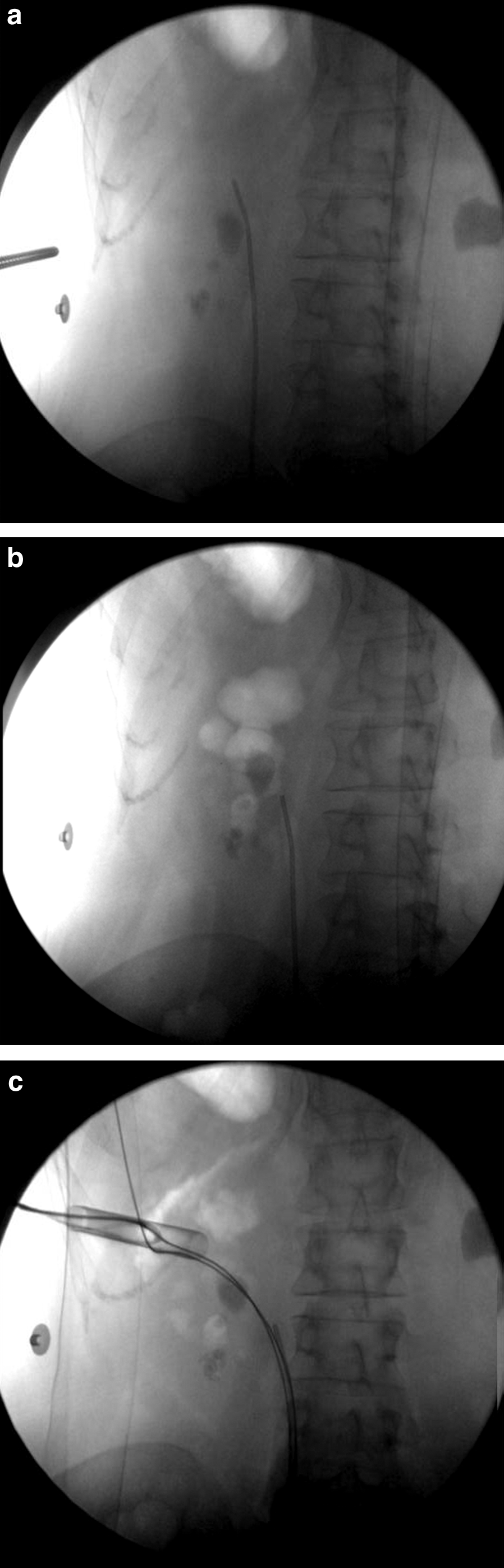
Percutaneous access utilizing air retrograde pyelogram to aide in opacifying the collecting system. Scout image is taken
Data analysis
Multivariable linear regression was used to determine the association between ED and the use of air pyelogram controlling for factors thought to affect ED. A multivariable linear regression was also used to determine the association between fluoroscopy time and the use of air pyelogram. Statistical analysis using multivariate tests was conducted using STATA (Version 10.0, College Station, TX).
Results
A total of 96 PNL procedures were included in this analysis. Of these, 60 were performed with an air retrograde pyelogram (AP) and 36 were performed with a contrast retrograde pyelogram (CP). The baseline characteristics of the two groups are presented in Table 1. There were no statistical differences between the baseline characteristics; however, there was a trend toward decreased ED in the AP group compared with the CP group. There was no difference in fluoroscopy time between the two groups.
BMI = body mass index.
On multivariable linear regression analysis controlling for age, gender, body mass index (BMI), stone burden, presence of hydronephrossis, number of percutaneous access sites, branched stone, and whether the stone crosses an infundibulum and type of drainage used, air was associated with significantly lower ED. The mean-adjusted ED during PNL for AP group was 4.45 mSv (95% CI 3.68–5.38) compared with 7.67 mSv (95% CI 5.99–9.82) for CP group (p = 0.001) (Fig. 2). Increasing BMI (p < 0.001), increasing stone burden (p = 0.009), and increasing percutaneous access sites (p = 0.013) were associated with significantly higher ED. In addition, branched stone (p = 0.002) and presence of hydronephrosis (p = 0.018) was associated with significantly lower ED. On multivariable linear regression controlling for the same factors, there was no association between fluoroscopy time and whether an air pyelogram or contrast pyelogram was performed (p = 0.150).
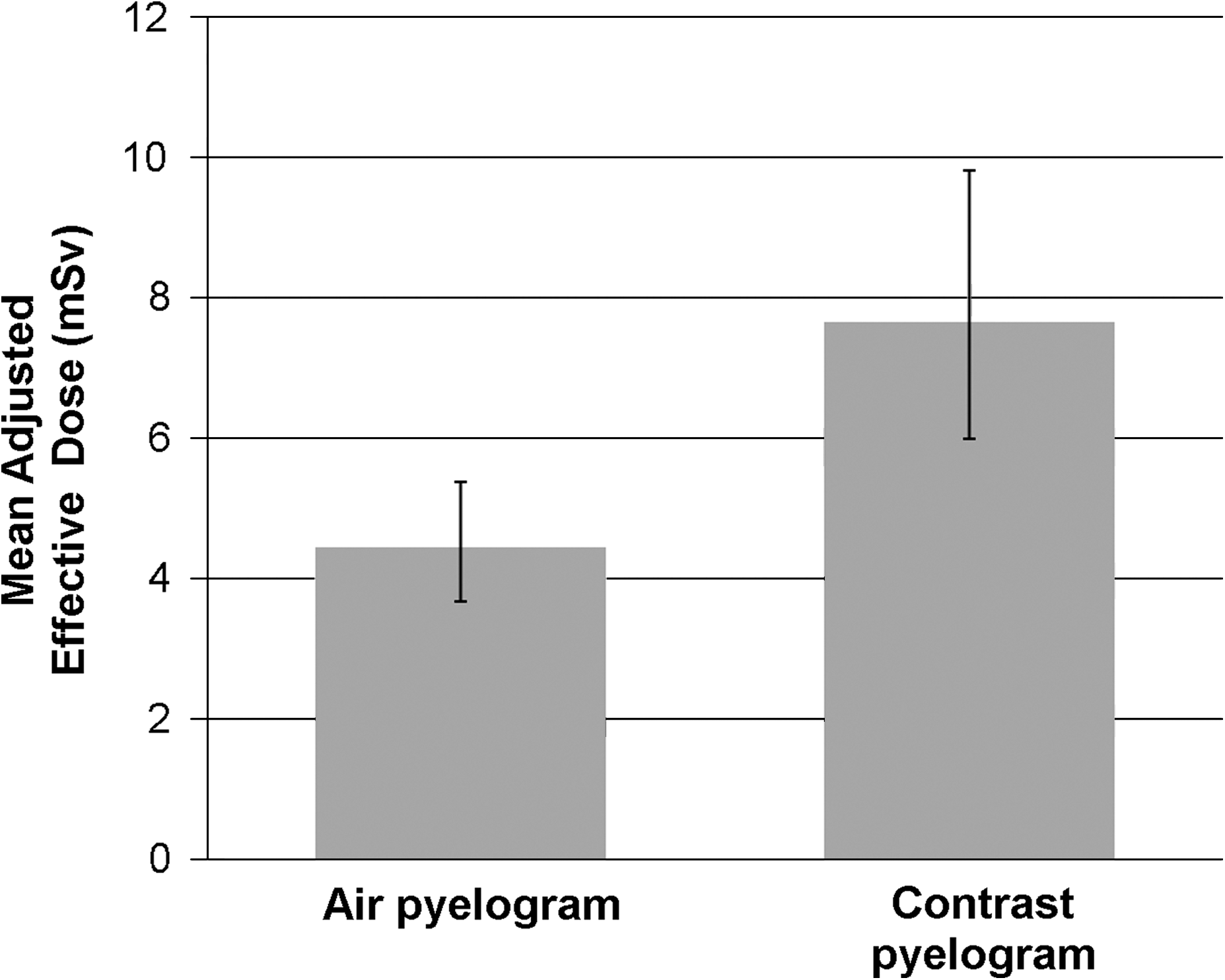
Comparison of mean-adjusted effective dose (mSv) between air pyelogram and contrast pyelogram.
Discussion
There have been a number of recent studies that have investigated the increased risks of patient radiation exposure. This concern has been well documented with regard to the increasing use of computed tomography (CT) imaging. 2,3 It is estimated that 29,000 future cancers in the United States can be attributed to CT scans performed in this country in 2007, and of those 14,000 are due to CT imaging of the abdomen and pelvis alone. 3 Patients with nephrolithiasis are at particular risk from radiation exposure due to the common utilization of NCCT imaging in the diagnostic work-up of these patients. Additionally, these patients are often exposed to radiation during interventions to treat their stones. Ureteroscopy, shock wave lithotripsy, and PNL all utilize fluoroscopy, thus contributing to patients' total radiation exposure.
A recent report from two academic centers addressed the issue of radiation exposure over a 1-year period in patients who had a primary acute stone event. 4 The investigators found that patients underwent an average of 4 radiographic examinations, including 1.7 CT scans during the 1-year period. The median ED the patients were exposed to was 29.7 mSv, and 20% of the patients were exposed to >50 mSv. This dose exceeds the International Commission on Radiological Protection recommendation on limits for occupational exposure to radiation. 5 The limit set for occupational exposure is 20 mSv averaged over a 5-year period with no >50 mSv in any single year. In comparison, a typical CT of the abdomen and pelvis without contrast exposes patients to a median of 15 mSv. 2 The recommendation on limits for public exposure is even stricter, suggesting no more than an average of 1 mSv per year over a 5-year period. Currently, there is no recommended limit for patient medical exposure as it should be determined by weighing the relative risks and benefits for each individual study or procedure. The investigation of radiation exposure of stone patients did not include radiation exposure related to any interventions the patients may have undergone during that 1-year period. 4
Fluoroscopy is commonly used to aide access during PNL. 6 Other imaging modalities have been used for access, including ultrasonography and CT-guided access. 7,8 Use of fluoroscopy during PNL is not limited to access alone. This modality is also used during the placement of guidewires down the ureter and dilation of the nephrostomy tract. Once intracorporeal lithotripsy is complete, fluoroscopy is often used to evaluate for residual fragments. Depending on the type of drain left at the completion of PNL, additional fluoroscopic images are often obtained. For instance, fluoroscopy is used to confirm the appropriate positioning of a nephrostomy tube or an internal ureteral stent.
The use of ultrasonography for access during PNL is an appealing way to reduce radiation exposure. However, ultrasonography is typically used in conjunction with fluoroscopy for PNL. 7 Although use of ultrasonography during access obviously reduces the total radiation exposure for the patient, it is unclear by how much. There has been one series reported using ultrasonography exclusively for PNL, without the aid of fluoroscopy. 9 The authors describe performing all stages, including dilation, with ultrasonography. They conclude that ultrasonography alone is a good method for uncomplicated PNL, and that in complex cases fluoroscopy should be employed until more experience is gained using ultrasonography. The main limitations of ultrasonography are user dependency, requiring training and experience, as well as observation difficulties of both stone and ureter, especially when placing wires during access. Until more experience can be gained using ultrasonography alone, or until newer imaging technologies are developed that do not utilize radiation, fluoroscopy will be necessary for the performance of PNL.
Risk factors for increased fluoroscopy exposure during PNL have been reported. Our own data suggest that increasing BMI, increasing stone burden, and increasing number of access tracts lead to an increase in ED, whereas branched stones and the presence of hydronephrosis are associated with decreased ED. 10 Others have found stone size and number of access tracts as the only factors related to increased fluoroscopy time. 11 Stone burden, the presence of hydronephrosis, and whether a stone is branched cannot be altered to effect radiation dose to patients during PNL. Patients can lose weight to reduce their BMI before PNL; however, it is not practical to delay PNL in patients who are symptomatic or obstructed while they attempt to lose weight. The number of access tracts is determined by stone characteristics and decreasing the number of accesses may prolong procedures and compromise stone-free rates.
The current study found that the use of air instead of iodinated contrast for retrograde pyelogram during access for PNL reduces the ED by nearly 50%, from 7.67 to 4.45 mSv. The present study did not demonstrate decreased fluoroscopy time with air; however, fluoroscopy time is felt to be a poor measure of radiation exposure during fluoroscopic procedures. 12 To our knowledge, this is the first study to demonstrate a modifiable surgical variable that affects radiation dose to patients during PNL. A previous study described a simplified technique utilizing fluoroscopy for access during PNL in 2007. 13 This technique allowed for triangulation of the targeted calyx and needle without the need for rotating the C-arm. A follow-up to this study demonstrated that as an inexperienced endourology fellow gained experience with this technique, the fluoroscopy time for the procedure decreased significantly. 14 This reduction of fluoroscopy time had more to do with experience than their actual technique, which was not compared with other techniques.
Although the use of air was associated with a significant decrease in the ED patients who were exposed to, it was not associated with decreased fluoroscopy time. This suggests that the air did not necessarily make access any easier or quicker. In our experience, we believe that air has certain advantages over contrast when obtaining access. Air preferentially fills and outlines the posterior calyces when patients are lying prone, thereby allowing more rapid identification of the appropriate access site. Injection of air into the collecting system does not obscure the view of the stone, which aides in the identification of the ideal access point to treat the targeted stone. The stone can be clearly observed during the entire access. Air is unlike contrast that typically obscures the stone. The diminished volume of air required for identification of the posterior calyces may have a secondary benefit in reducing the extent of extravasation encountered especially when multiple access sites are required or during difficult access. Extravasated iodinated contrast makes it particularly difficult to identify the collecting system. Although these are perceived advantages of air, they did not contribute to reduced radiation dose as there was no difference in fluoroscopy time. One concern when using air for retrograde pyelogram is the perceived risk of air embolism. 15,16 Based upon the literature, air embolism is an extremely rare event. It is our routine to inject 5–10 cc of air. We have not encountered any untoward events when using the air pyelogram technique in over 150 cases.
The explanation for decreased radiation exposure with the use of air is related to the physics of image acquisition and the impact of the different densities between air and contrast. The C-arm detects different densities via the image intensifier and automatically adjusts the tube current (mAs) or tube potential (kVp) to maintain image quality. 17 This is a feature on most C-arms called automatic brightness control. With denser materials such as iodinated contrast, the C-arm will increase tube potential or tube current to maintain the image quality. This allows for better image quality with the denser material; however, it also leads to increased radiation dose to the patient.
There are a number of limitations to the current study. This is a retrospective investigation and information on radiation dose was not saved for every PNL case at our institution. Whether this information was stored was dependent on the radiology technician working the C-arm for any given case. We do not believe that this limitation should introduce any bias into the data. Another limitation is that the ED does not provide information on doses to specific organs or sites in the body. As different tissues have different radiosensitivities, we are not able to make recommendations based on potential tissue injury.
It is unclear what the risks of malignancy are for these lower doses of radiation exposure; however, most experts agree there is a linear relationship between ED and risk of cancer. 5,18,19 Data extrapolated from atomic bomb survivors in Japan demonstrate a significantly increased risk of cancer even at very low radiation exposures. 19 In general, it is felt that there is a significantly increased risk of cancer with an acute exposure of 10 to 50 mSv and with protracted exposures of 50 to 100 mSv. 18 The mean ED reported in our series has to be taken in the context of overall radiation exposure for stone patients. Since these patients are already at increased risk, every small decrease in radiation dose is significant.
With increasing concern over patient radiation exposure, it is important to counsel patients about the risks of fluoroscopy and to minimize their exposure. The use of PNL in the United States more than doubled between 1988 and 2002, from 1.2 per 100,000 people to 2.5 per 100,000 people. 20 The majority of these patients will be exposed to radiation from diagnostic imaging as well as fluoroscopy. It is imperative to work toward reducing that exposure.
To minimize radiation during PNL, the fluoroscopy beam should be collimated to the area of interest, the image intensifier should be placed as close to the patient as possible, and a pulsed fluoroscopy mode should be used. 21 In addition to these technique modifications, the current study suggests that the use of air instead of iodinated contrast may further reduce patient radiation exposure during percutaneous stone removal.
Conclusions
The use of room air for performance of a retrograde pyelogram during access for PNL significantly reduces radiation exposure. This finding is likely due to the increased density of contrast leading to automatic adjustment of the C-arm tube current and tube voltage. Given these findings, we continue to use air pyelograms to aide in fluoroscopic access during PNL.
Footnotes
Disclosure Statement
No competing financial interests exist.