
Abstract
The indications, instrumentation, surgical technique, and complications of laparoendoscopic single-site radical nephrectomy (LESS-RN) are being described in detail in an attempt to familiarize urologists with this novel laparoscopic technique. Our initial experience of 30 consecutive cases of LESS-RN is reported. The results indicate that, in experienced hands, LESS-RN is feasible and safe, with results comparable to those of conventional laparoscopic radical nephrectomy. Nevertheless, larger series of patients are needed to prove if the increased technical difficulty of LESS-RN justifies its use in routine urologic practice.
Introduction
Indications and Contraindications
Indications and contraindications of LESS-RN are similar to those of conventional laparoscopic nephrectomy. LESS-RN is indicated for the excision of renal tumors up to stage T3b in the absence of positive lymphs node or distant metastasis. 3,4 In the presence of a solitary kidney or T1a and T1b disease, however, a more conservative nephron-sparing surgery should be considered. 5
Maximum tumor size for laparoscopic nephrectomy has not been standardized. The accumulation of laparoscopic experience tends to expand individual surgeon indications for tumor nephrectomy. Tumors with a diameter of up to 14 cm have been reported to be successfully managed via the laparoscopic approach. 4,6 Contraindications for LESS-RN include patients who are candidates for laparoscopy because of cardiovascular and respiratory comorbidities or uncorrected coagulopathy. 7 Ipsilateral abdominal surgery could be considered a relative contraindication, because adhesions could be challenging even to the most experienced surgeon.
Preoperative Workup
Every case of suspected renal malignancy needs thorough investigations to exclude potential metastatic disease before laparoscopic management can be initiated. High-resolution contrast CT is of outmost importance, because it determines tumor size, tumor invasion, and suspicious lymph nodes and may indicate vessel involvement. 3 If renal vein or inferior vena cava involvement is suspected, then an MRI should be performed. Contrast CT is for the assessement of contralateral renal function and size. In patients with reduced renal function or a small contralateral kidney, it is important to establish differential renal function. Further imaging investigations are necessary for the detection of metastasis. A chest and brain CT scans as well as bone scintigraphy should be considered in the preoperative evaluation.
Materials
Instrumentation
Instrumentation for LESS includes a combination of specially designed and conventional laparoscopic instruments, listed below:
1. Single incision port access
Nondisposable
X-cone (Karl Storz, Tuttlingen, Germany)
Endocone (Karl Storz, Tuttlingen, Germany)
Disposable
TriPort (Olympus, Hamburg, Germany)
QuadPort (Olympus, Hamburg, Germany)
Gelport (Applied Medical, Rancho Santa Margarita, CA)
Gelpoint (Applied Medical, Rancho Santa Margarita, CA)
Other ports, such as Uni-X single laparoscopic port system (Pnavel Systems, Morganville, NJ), are considered not appropriate for LESS-RN, because the insertion of large diameter instruments, such as the vascular stapler, is not possible. We currently perform our cases using the QuadPort.
2. Laparoscopic camera
A 30-degree lens high-definition laparoscopic 5-mm camera with flexible handle or a 0-degree lens high-definition laparoscopic 10-mm camera (EndoEye, Olympus Medical, Tokyo, Japan) was used during most of the cases in our series. A 30-degree lens high-definition laparoscopic camera, 5-mm in diameter, extra long (eg, Karl Storz, Tullingen, Germany) was also used for the performance of LESS-RN.
3. Instruments
Nondisposable
Prebent instruments (Olympus, Hamburg, Germany; Karl Storz, Tutllingen, Germany)
Disposable
Articulating instruments, (RealHand, Novare Surgical Systems Inc, Cupertino, CA; Autonomy Laparo-Angle, Cambridge Endo, Framingham, MA; EndoMiniDissect and EndoClinch, Covidien, Gosport, United Kingdom)
We currently favor the use of prebent instruments in combination with conventional laparoscopic instruments. Nevertheless, prebent or articulating instruments were used, depending on the availability for the performance of the current series of LESS-RN.
4. Conventional laparoscopic (straight) instruments.
Nondisposable
Laparoscopic scissors
Laparoscopic bipolar forceps
Laparoscopic ultrasonic scissors (Olympus, Hamburg, Germany)
Needle scopic instruments—forceps, needle holder (Karl Storz, Tutllingen, Germany)
Disposable
Hem-o-lok clips (Teleflex Medical, Research Triangle Park, North Carolina)
Vascular Endo GIA linear stapler (Covidien, Dublin, Ireland)
Surgical Steps
Patient setup and trocar placement
The procedure is performed with the patient under a general anesthetic. A urethral catheter and a nasogastric tube are inserted immediately before the procedure. The patient is catheterized and placed in the lateral decubitus position with the table in slight flexion on the patient's waist (Fig. 1). Pressure points are minimized, and the upper arm is brought cranially and secured on a cradle with posterior supports. Skin preparation is the same as the conventional open approach in case it becomes necessary to convert to open surgery.
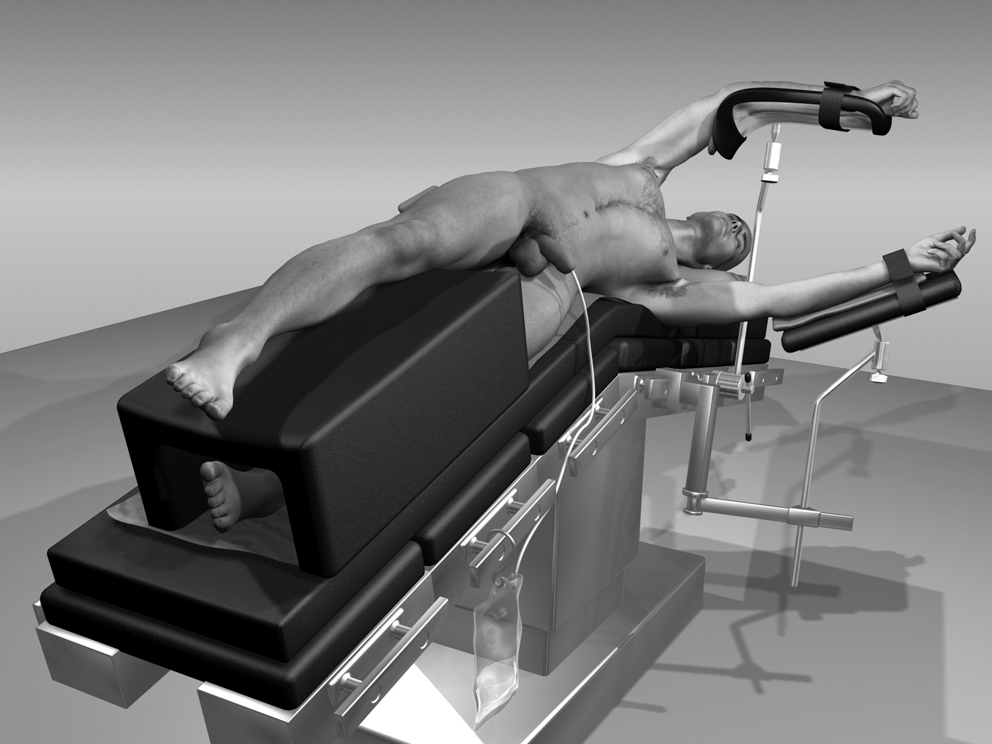
Patient positioning.
The patient is moved back to a dorsal supine position, and a 3-cm incision is made at the umbilicus (minilaparotomy); the multiport is positioned according to manufacturer's instructions. In obese patients, we prefer the insertion of the multiport in a paraumbilical site on the side of the planned nephrectomy (Fig. 2).
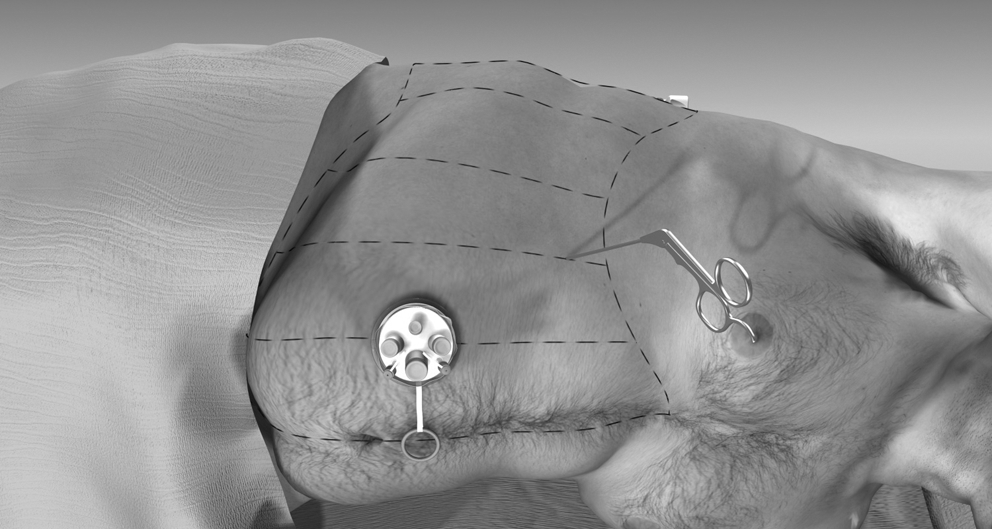
Port placement in obese patient.
Exposure of the kidney (mobilization of the colon)
In the case of a left nephrectomy, the operation begins with an incision along the white line of Toldt from the caudal part of the descending colon up to the level of the spleen (the iliac vessels should be exposed) The splenocolic ligament is released to maximize exposure of the kidney. Prebent forceps and scissors are recommended for colonic mobilization using a combination of sharp and blunt dissection. The colon is then retracted medially and away from the operating field. The use of monopolar coagulation should be avoided during the mobilization of the colon, because thermal injuries are the most common cause of bowel injury. 8 Cold or ultrasonic scissors as well as bipolar coagulation could be used instead. Injuries to the spleen are avoided by minimizing splenic retraction and by the use of a nasogastric tube for decompression of the stomach.
In the case of a right nephrectomy, the reflection of the ascending colon should be mobilized from the cecum to the hepatic flexure (Fig. 3). All subhepatic parietal peritoneum must be dissected, including the triangular ligament. The mobilization of the liver and colon allows for adequate exposure of the kidney. Nevertheless, in some cases, additional retraction of the liver might be necessary to expose the right kidney. An additional needlescopic grasping forceps is inserted directly (without trocar), as shown in Figure 2.
Mobilization of the ascending colon.
Ureter mobilization
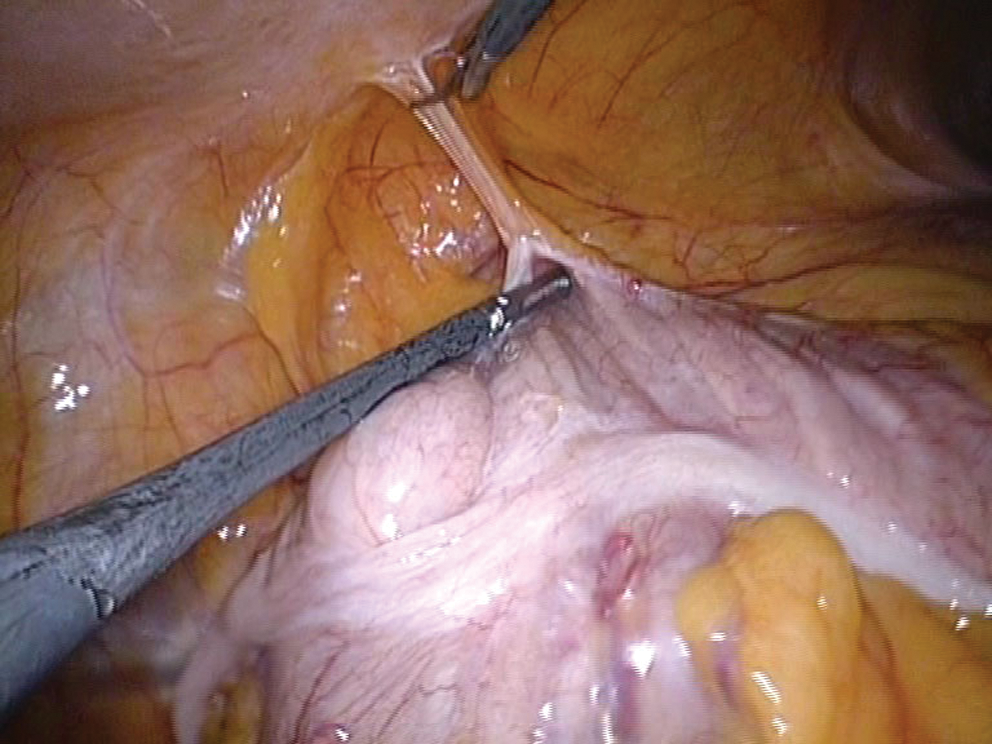
The ureter is then identified within the retroperitoneal fat. Early mobilization of the ureter provides a point for the retraction of the kidney—essential for LESS-RN. A prebent instrument provides anterior ureteral retraction, exposing the surrounding fatty tissue, which is dissected using another prebent or a straight conventional laparoscopic instrument (Fig. 4). We favor the use of bipolar forceps for the dissection of the ureter. Dissection continues up to the level of the ureteropelvic junction. The mobilized ureter is used for the retraction of the kidney, which facilitates the exposure of the renal hilum.
Mobilization of ureter.
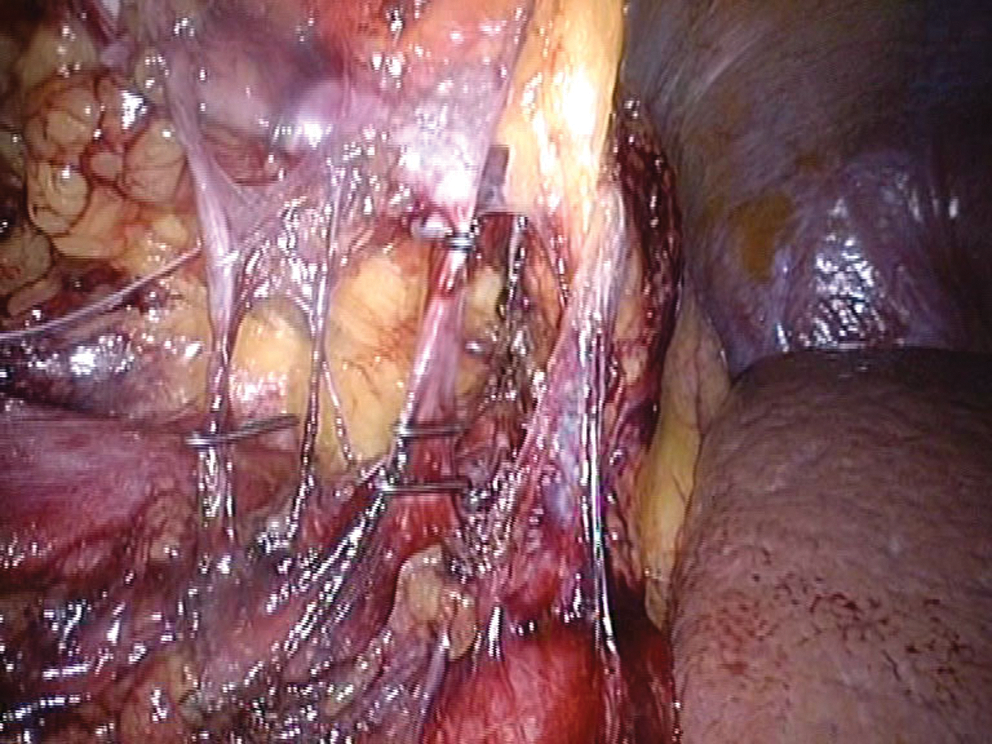
The retraction of the ureter is facilitated by suture retraction. A suture with a long straight needle is used for the purpose; the needle is passed through the abdominal wall from outside to inside the abdominal cavity, around the ureter and through the abdominal wall again (Fig. 5). The suture is tied or clipped to the skin. The continuous traction provided by the suture facilitates the exposure and dissection of the medial margin of the kidney, including the renal hilum. If the initial identification of the ureter is difficult, then its dissection can begin from as low as the external iliac vessels, where it can easily be identified.

Stay suture placement to elevate ureter to facilitate renal mobilization.
Gonadal vein dissection
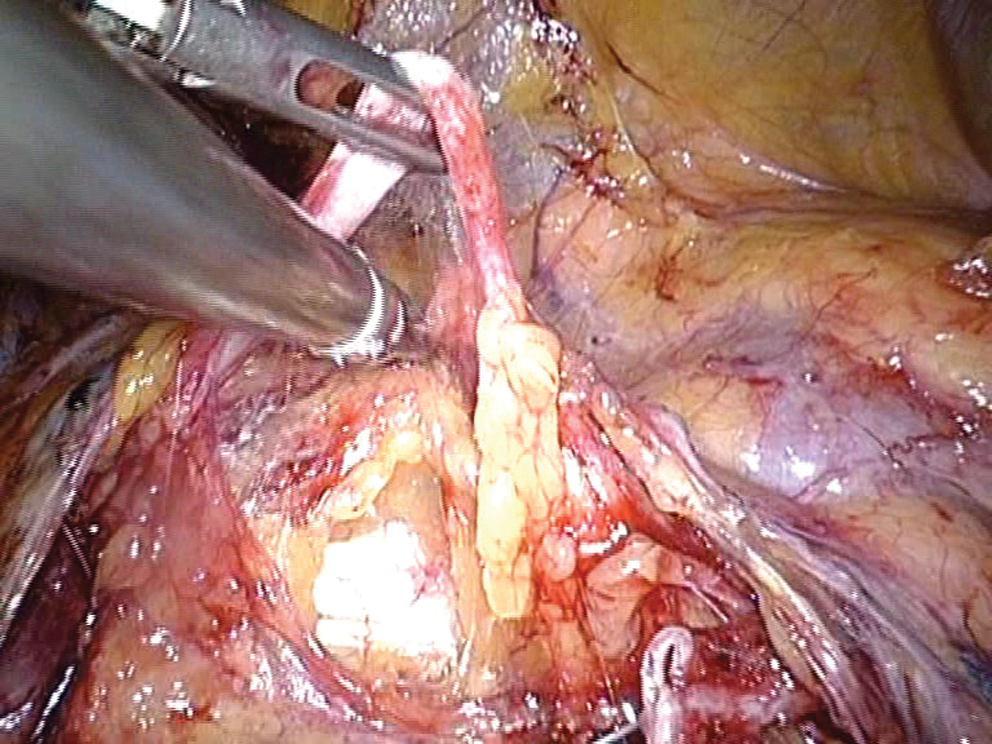
When performing a right-sided LESS-RN, the dissection of the ureter is performed toward the ureteropelvic junction along the inferior vena cava using bipolar forceps and a prebent grasper. The gonadal vein should be identified and is ligated with metal clips near its insertion to the inferior vena cava (Fig. 6). On the left-side nephrectomy, the clips for the gonadal vein should not be placed too cranially toward the renal hilum, because the clips may interfere with the subsequent application of Hem-o-lok clips or vascular EndoGIA stapler across the renal vein.
Clipping of gonadal vein.
Needlescopic liver retraction
In right LESS-RN, retraction of the liver away from the operative field is essential for the performance of the next steps of the procedure. For this purpose, a 2.5-mm needlescopic instrument is inserted without trocar to retract the liver (Fig. 7). The latter incision does not leave a noticeable scar after instrument retrieval and does not need suturing. For liver retraction during right-side nephrectomy, the instrument could alternatively be inserted in the anterior axillary line below the 12th rib. Insertion of a needlescopic instrument to facilitate retraction is occasionally necessary in left LESS-RN.
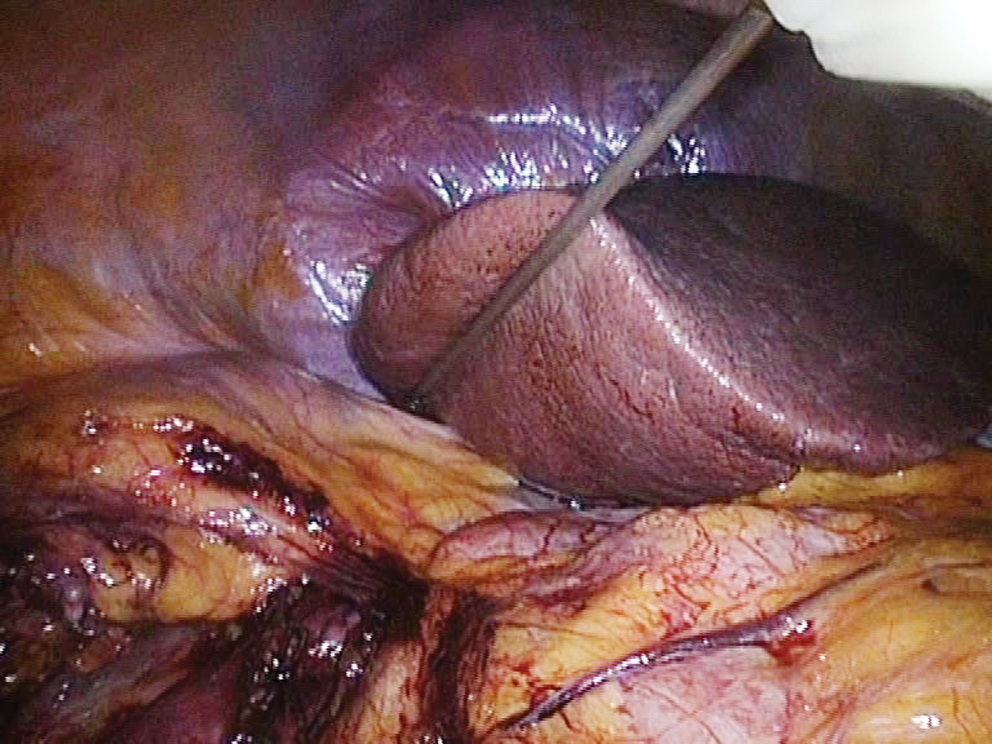
Insertion of needlescopic instrument for liver retraction.
Hilar dissection
The renal vein is the first hilar vessel to be identified and is dissected from the surrounding connective tissue by a combination of sharp and blunt dissection. A prebent instrument is held in the left hand of the surgeon and provides traction while bipolar forceps or ultrasonic scissors or prebent dissector is used in the right hand.
Control of the renal pedicle
Renal artery branches can be identified cranially and posteriorly to the renal vein. Prebent forceps are used to retract the renal artery, which is subsequently freed from the surrounding connective tissue. A minimum of two Hem-o-lok clips should be placed medially toward the aorta and one toward the kidney (Fig. 8). Titanium clips may also be used. The renal artery is divided with scissors. Additional arterial branches are ligated and divided in the same manner. When the renal artery and its branches are divided, the renal vein is optimally exposed.The posterior side of the renal vein should be completely mobilized; a needlescopic instrument may facilitate dissection. Large Hem-o-lok clips are placed, and the vein is transected. It is important to visualize the hooked tip of the clip behind the vessel before closure of the clip-applicator (Fig. 9).
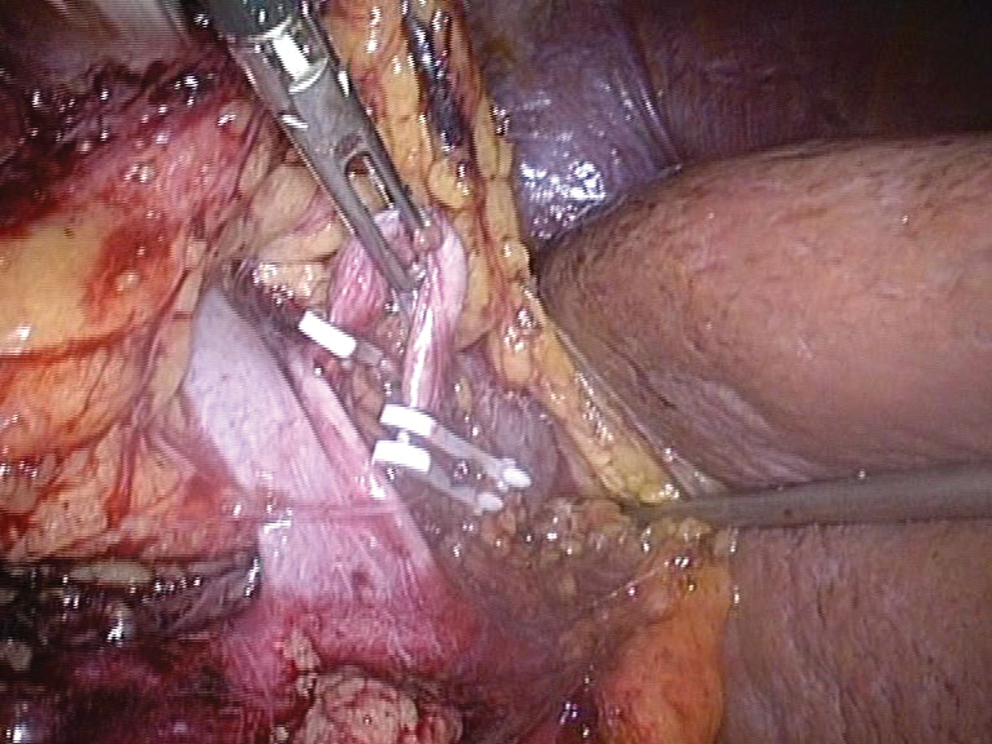
Clipping of renal artery (Hem-o-lok clips).
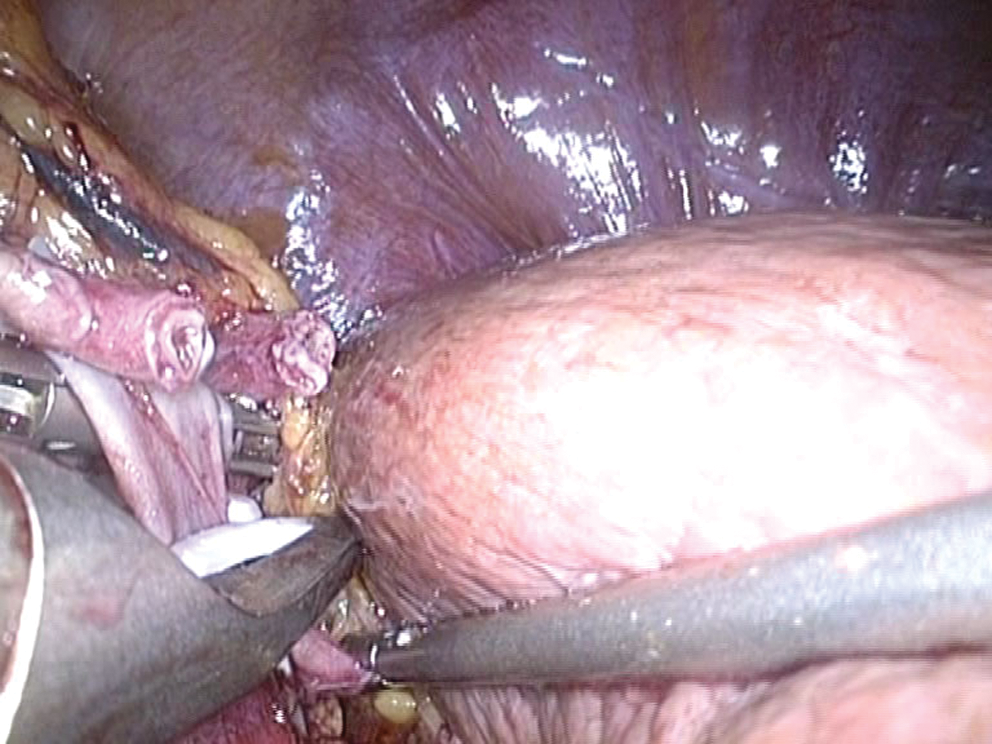
Clipping of renal vein (Hem-o-lok clips).
The renal vein could also be divided by using a vascular EndoGIA stapler (with articulating tip). In a left nephrectomy, positioning the stapler across the renal vein proximal or distal to the adrenal vein results in excision or sparing of the ipsilateral adrenal gland. The kidney with the perirenal fat and ipsilateral adrenal in the intact Gerota fascia is removed during radical nephrectomy. An adrenal-sparing approach could be considered for patients with smaller renal tumors. All stapler devices should be carefully inspected before use, because malfunction, although uncommon, can have disasterous consequences. 8
Kidney mobilization
After control of the renal vessels, the lower pole is dissected from its attachments using the bipolar forceps or ultrasonic scissors. The ureter is left intact to prevent rotation of the kidney. Mobilization of the upper pole is performed before lateral dissection. This prevents the kidney from falling into the operating field and obscuring the major vessels. Any identified lumbar vessels are clipped and transected. Once the upper pole of the kidney is free, lateral dissection is commenced. Finally, the ureter is clipped, divided, and the kidney is ready for retrieval.
Specimen retrieval
A standard 15-mm endocatch bag can be inserted through the QuadPort, because there is a 15-mm port available on the device. The specimen is placed and secured inside the bag and is retrieved at the end of the operation after hemostasis has been reviewed. The incision in the fascia and skin may be extended to facilitate specimen retrieval. At the end of the procedure, a 16F Robinson drain may be placed through the umbilical incision, if needed. The incision is closed with interrupted suture to the fascia to avoid a subsequent umbilical hernia.
Postoperative care
The nasogastric tube is removed after the operation and the urinary catheter on postoperative day 1. The drain is removed when the drainage declines to less than 50 mL per day (usually on postoperative day 1 or 2). A liquid diet is initiated on the first evening after the operation. Low molecular weight heparin is commenced on postoperative day 1 and continued until the patient is mobile.
Management of intraoperative complications
In the laparoscopic literature, the majority of intraoperative complications are related to adjacent organ (4% incidence) and vascular injury (2%). 8 Bowel, spleen, pancreas, and diaphragm injuries have been reported to have incidence of 0.8%, 1.4%, 2.1%, and 0.6%, respectively. Vascular complications are associated with malfunction of stapler devices in 1.7% to 10% of the cases. 8 Organ and vascular injuries often necessitate open conversion and reoperation. LESS-RN, regardless of the approach (simple, radical, donor or partial), has been reported to have low intraoperative complication rates (Table 1). Nevertheless, the currently available data are limited to a low number of cases.
EBL = estimated blood loss; LOS = length of stay; n/a = not available; ICU = intensive care unit; lap = laparoscopy.
Bowel injuries should be assessed carefully and, if necessary, by an open surgical approach. Colostomy or bowel resection and reanastomosis should be performed according to the type of injury found. Splenic injury can be managed by the application of hemostatic agents and pressure. Uncontrolled bleeding or significant bleeding should be managed by splenectomy. Pancreatic injuries are often complicated and may necessitate multidisciplinary management. Injuries to the diaphragm should be sutured, and a thoracic drainage should be placed, if deemed necessary.
Management of postoperative complications
Deep venous thrombosis, chronic renal failure, port-site metastasis, and chylous ascites are postoperative complications that have been reported for laparoscopic radical nephrectomy. 8 Deep venous thrombosis is managed conservatively and should be prevented by compressive stockings intraoperatively and administration of low molecular weight heparin and early mobilization postoperatively. Chronic renal failure is a significant issue for patients who are undergoing radical nephrectomy. The performance of nephron-sparing surgery should be selected over radical treatment when the appropriate indications are present. Port-site metastases are very rare (six cases reported totally) and can be prevented by avoiding morcellation and using an endoscopic retrieval bag. Chylous ascites is prevented by clipping the large lymphatic vessels that cross the renal vein.
Summary of Experience in LESS-RN
The published experience of LESS-RN is summarized in Table 1. There are only limited reports published on LESS-RN, and reported complications remain minimal. We have currently performed 30 cases of LESS-RN at our institutions. Perioperative data for our series of patients are presented in Table 2. One postoperative bleeding complication occurred. The patient was transfused with 2 units of blood. This case was managed without reintervention. Prolonged ileus developed in one patient; it was managed conservatively. A case of postoperative deep venous thrombosis was observed and was managed with anticoagulants.
BMI = body mass index.
Conclusion
Early experience and results of LESS-RN are encouraging. While the procedure is technically challenging, we are able to observe standard oncologic principles with minimal morbidity.
Footnotes
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
*
A coordinating article with video is available in Videourology 25/1 at