
Abstract
Background and Purpose:
Membranous urethral length is one of several factors that can influence return of continence after radical prostatectomy. Using our robot-assisted laparoscopic prostatectomy (RALP) database, we assessed which preoperative (with endorectal coil MRI [eMRI]) and intraoperative anatomic measurements correlate with return to urinary continence (no pads) and continence quality of life (CQOL) as determined by the International Consultation on Incontinence Questionnaire (ICIQ) score.
Patients and Methods:
A total of 75 patients who underwent RALP and eMRI by a single surgeon were analyzed. To emulate the distal continence zone intraoperatively, stretched urethral length (distance from the perineal membrane to the prostate apex on stretch) and cut urethral length (urethral stump length) were individually measured and recorded after apical dissection. Preoperative International Prostate Symptom Scores (IPSS) were recorded. Univariate and multivariate Cox regression analysis were performed to determine the association between MRI-measured and intraoperative urethral lengths and return to continence as well as CQOL.
Results:
None of the urethral measurements as determined by eMRI correlated with continence or ICIQ scores. On multivariate analysis, only membranous urethral length on eMRI approached significance with respect to ICIQ (P=0.07). On multivariate analysis controlling for preoperative age, body mass index, IPSS score, and gland size, both stretched and cut urethral length correlated with decreased time to continence (P=0.03 and P=0.04 respectively).
Conclusion:
Longer stretched and cut urethral lengths appear to correlate with faster return to a pad-free state. Attention to maximal preservation of the distal continence mechanism is important for optimal continence outcomes after RALP.
Introduction
Perhaps the most important factor in the preservation of continence after RP is the preservation of the functional sphincter mechanism or the “intramural distal sphincter mechanism,” a term coined by Turner-Warwick. 4 Here, the sphincteric mechanism comprises the striated sphincter externally and the urethral wall smooth muscle and elastic tissue and the urethral mucosa internally. The striated sphincter is functional only from the prostate apex to the bulb, whereas the internal component of the distal sphincter mechanism extents to the verumontanum. Maximal preservation of this zone that extends from the verumontanum to the penile bulb or perineal membrane is critical in RP.
Endorectal coil MRI (eMRI) has been shown to be the best method for estimation of clinical stage, prostatic anatomy and measurements, and urethral lengths before RP. No studies, however, have assessed intraoperative prostatic and urethral measurements, how they correlate with preoperative MRI measurements, and whether they can be predictive of continence outcomes. Furthermore, no study has demonstrated how these factors influence continence quality of life (CQOL). We examine the preoperative (using eMRI) and intraoperative anatomic characteristics and urethral measurements and their correlation with the eventual timing and return to full urinary continence and CQOL.
Patients and Methods
The most recent 75 patients who underwent robot-assisted laparoscopic prostatectomy (RALP) by a single surgeon (RG) and who had undergone preoperative eMRI imaging were analyzed. All were prospectively entered into our Institution Review Board approved prostatectomy database. In the last 2 years, all patients who were scheduled for RALP at our institution have undergone preoperative eMRI for anatomic and optimal clinical cancer staging. All MRIs were performed on a 1.5 Telsa GE Signa Excite scanner (Platform V. 11x) with the use of an endorectal coil.
The following sequences were obtained: T1 weighted without fat suppression in the axial plane with full field of view and coned-down field of view, T2 weighted without fat suppression in the axial, coronal, and sagittal planes with coned-down field of view, T2 weighted with fat suppression in the axial plane with coned-down field of view and diffusion-weighted images in axial plane with coned-down field of view. Apparent diffusion coefficient map was obtained in each case. Multiplane reconstructions in coronal-oblique plane through the prostatic urethra were performed on Aquarius Net Workstation V4.4.3.2.3. Prostate dimensions (height, length, and width) and urethral lengths were measured by one of two attending radiologists.
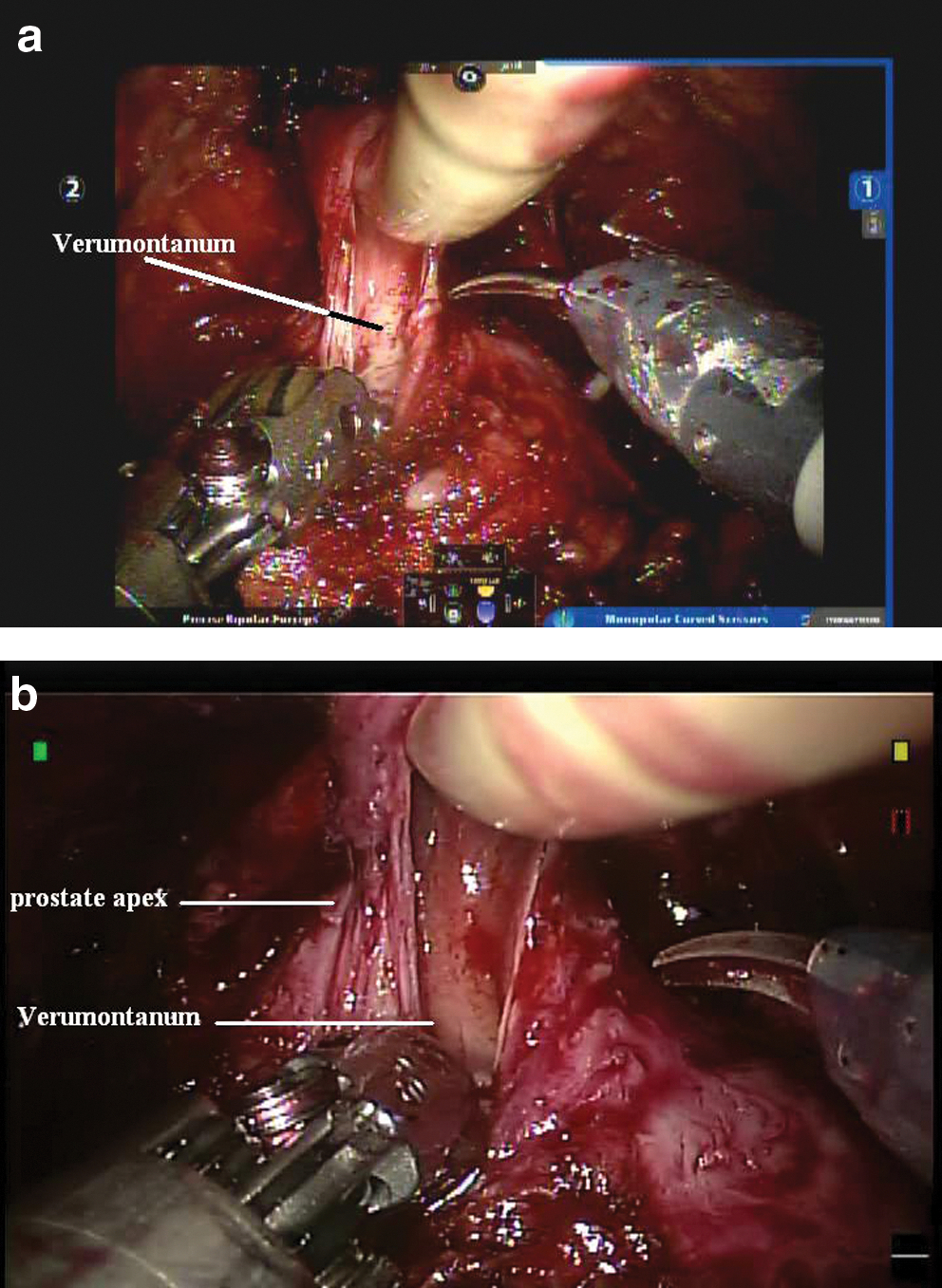
The distal continence zone was assessed by measuring the distance between the verumontanum to the penile bulb (just below the urogenital diaphragm). Membranous urethral length was also separately determined as the distance from the apex of the prostate to the bulb (Fig. 1). To closely approximate the distal continence zone intraoperatively, stretched urethral length (distance from the urogenital diaphragm to the prostatic apex with cephalad retraction) and cut urethral length (length of preserved urethral stump) were individually measured with a surgical tape ruler and recorded after apical dissection (Fig. 2). The cephalad retraction was achieved with the fourth arm of the robot on the base of the prostate. The amount of cephalad retraction used was the same retraction that is routinely used and is customary during apical dissection in robot-assisted RP. This retraction is necessary for full visualization and dissection of the prostatic apex to help minimize the risk of positive surgical margins. We measured the distance specified just before urethral transection.
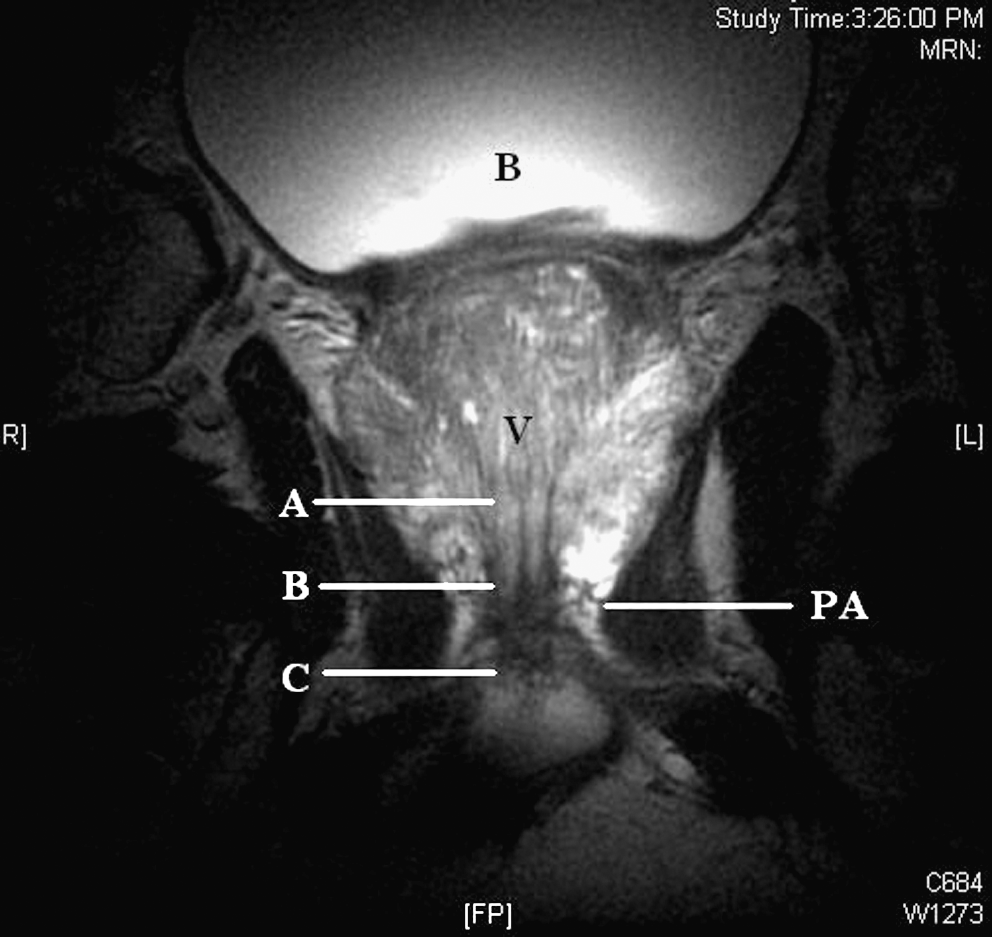
Coronal T2 weighted image of an endorectal MRI image. Distance from A to C (distance from distal verumontanum to penile bulb) represents functional distal urethral length. Distance from B to C represents membranous urethral (sphincteric urethral) length. B=bladder; V=verumontanum; PA=prostatic apex.
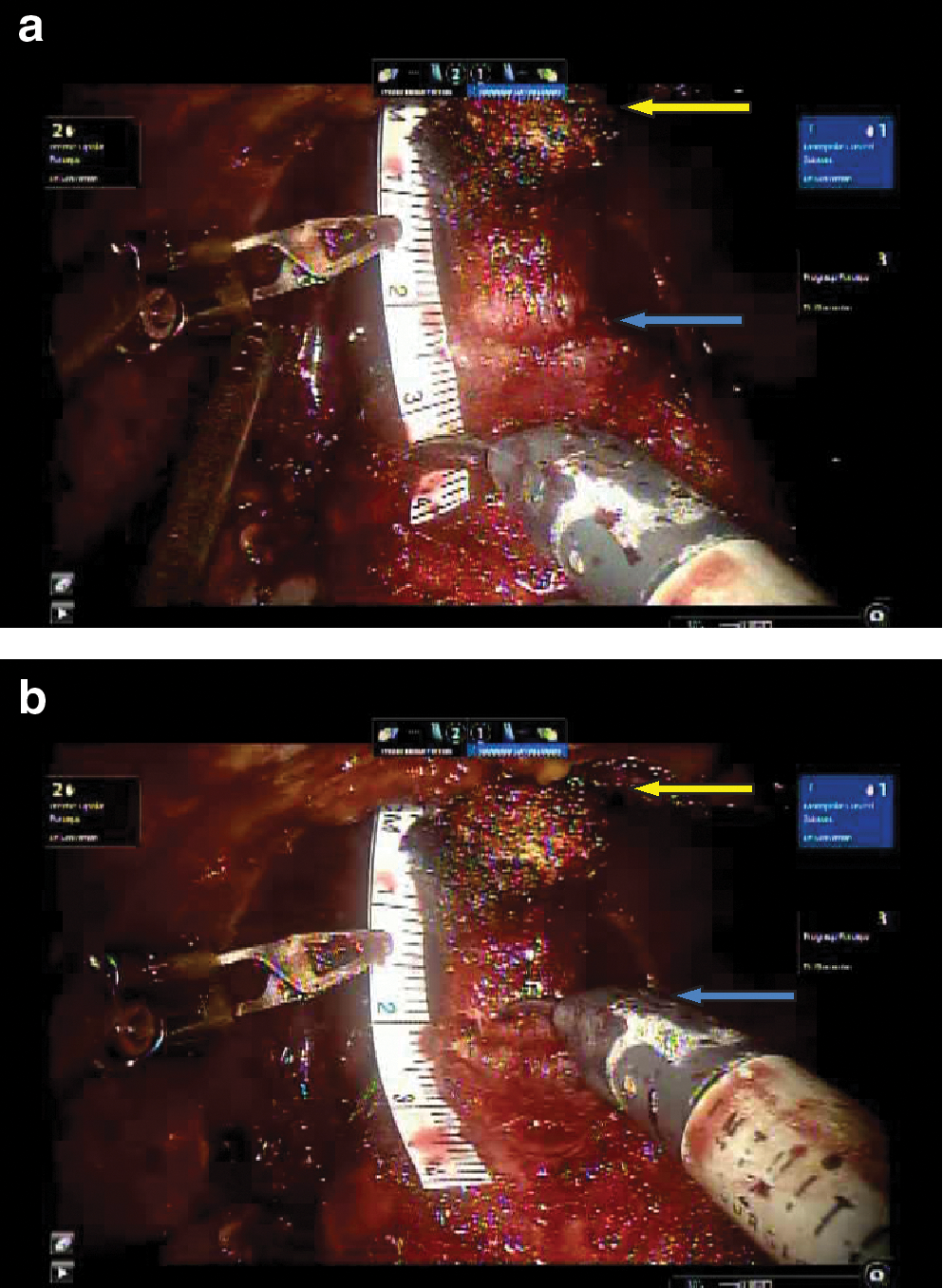
Intraoperative photograph demonstrates both stretched
Preoperative International Prostate Symptom Scores (IPSS) was recorded, as well as postoperative pad use. CQOL was determined by the International Consultation on Incontinence Questionnaire (ICIQ) scores (see Appendix). These were assessed postoperatively for each patient at 6 weeks and 3 monthly intervals subsequently. The final ICIQ score was determined at the time when the final continence outcome was reached, or at the final follow-up appointment for patients in whom 18-month data were not available yet.
Statistical analysis
Correlations between all intraoperative and MRI measurements of urethral length, IPSS prostate measurements, demographic factors (eg, age, body mass index [BMI]) and ICIQ as well as continence months were assessed using Pearson correlations. Univariate Cox regression models were used to examine the relationships between continence months and intraoperative and MRI measurements of urethral length, as well as other important factors including IPSS, age, BMI, race, and prostate measurements. Kaplan-Meier survival curves were used to plot the cumulative incidence of continence by urethral length. Hazard ratios (HR) and 95% confidence intervals (CI) were estimated for the association between continence and various measures of urethral length using a continuous variable as well as a categorical variable (<2 cm or ≥2 cm) where the cutoff point selected of 2 cm was the median length.
Multivariate analysis was also performed to determine the associations between ICIQ and intraoperative and MRI measurements of urethral length using linear and categorical models. For the association between urethral cut length and continence month, we also assessed effect modification by age (<60 vs ≥60), by BMI (nonobese vs obese), and by race (white vs others). SPSS software was used for all statistical analysis.
Results
The clinical and demographic information can be seen in Table 1. On average, patients were continent by 5.2 months (range 0–15 mos). The positive margins rate was 18.6% with 4/15 patients having positive apical margins. Three patients were incontinent at the time of the study, because of a limited follow-up of only 5 months. None of the urethral lengths as determined by eMRI correlated with ICIQ scores. Apex to base length, pathologic gland weight, and IPSS scores all correlated with increasing ICIQ scores (poorer CQOL, P<0.05) on univariate analysis. On multivariate analysis, only eMRI measurements of membranous urethral length and verumontanum-bulb length (length of intramural distal sphincteric mechanism) approached significance in relation to postoperative ICIQ scores (0.07 and 0.10, respectively) (Table 2). None of the eMRI urethral measurements correlated with pad use.
PSA=prostate-specific antigen; IPSS=International Prostate Symptom Score; MRI=magnetic resonance imaging; ICIQ=International Consultation on Incontinence Questionnaire.
Data controlling for age, race, body mass index, International Prostate Symptom Score, and prostate weight.
CI=confidence interval; BMI=body mass index; IPSS=International Prostate Symptom Score; ICIQ=International Consultation on Incontinence Questionnaire; MRI=magnetic resonance imaging.
The intraoperative urethral lengths did not correlate with CQOL (ICIQ scores) on univariate or multivariate analysis. In terms of continence, on multivariate analysis, both stretched (P=0.03) and cut urethral length (P=0.04) correlated with decreased time zero pad use (Table 2). On Cox regression analysis using urethral length as a categorical variable, a cut urethral stump length of at least 2 cm was a significant predictor of time to pad-free state, P=0.02 (Fig. 3).
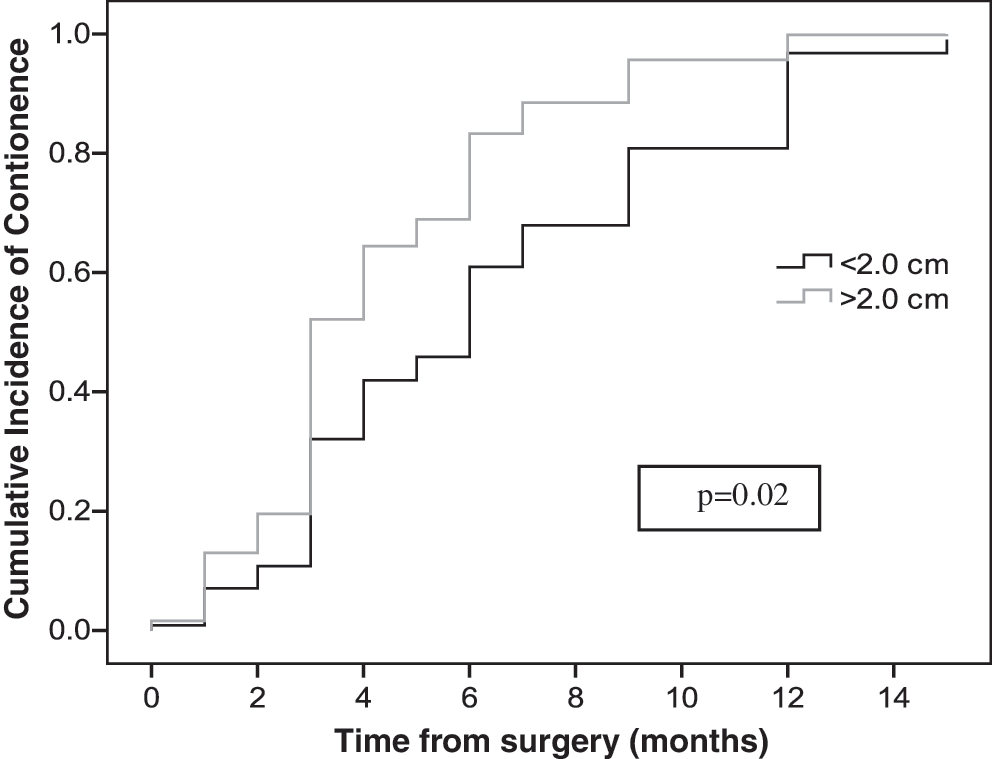
Return to continence in patients with a urethral length less than and greater than 2 cm.
Based on the mean age of our sample population (60 years), we further stratified patients by age as a categorical variable. Multivariate analysis demonstrated that a longer urethral stump in patients >60 years was a significant predictor of return to continence with a hazard ratio of over 7, P=0.001 (Table 3).
Data controlling for age, race, body mass index, International Prostate Symptom Score, and prostate weight.
CI=confidence interval.
Discussion
Based on Turner-Warwick's observations and Gil Vernet 5 before him, Myers described the anatomy pertinent to RP. 6 He divided the male continence zone into a proximal or superior sphincter vs a distal or inferior sphincter separated by the verumontanum. He identified various segments comprising the urinary control mechanism including: (1) An intact bladder neck with its preprostatic sphincter (internal sphincter), (2) the inframontanal urethra, and (3) the levator ani (puboanalis-puboperinealis complex) forming the urogenital hiatus that flanks the sphincteric (membranous) urethra. The “intramural distal sphincteric mechanism” extends from the verumontanum to the perineal membrane or the penile bulb. Here, the sphincteric mechanism comprises the striated sphincter externally and the urethral wall smooth muscle and elastic tissue and the urethral mucosa internally. The striated sphincter is functional only from the prostate apex to the bulb, whereas the internal component of the distal sphincter mechanism extents to the verumontanum. This internal component has been described as being the important component for urinary control, not the striated sphincter. With the advent of RALP and the magnification afforded in a relatively bloodless field, the different anatomic components of the distal sphincteric mechanism can be visualized intraoperatively in detail (Fig. 4).
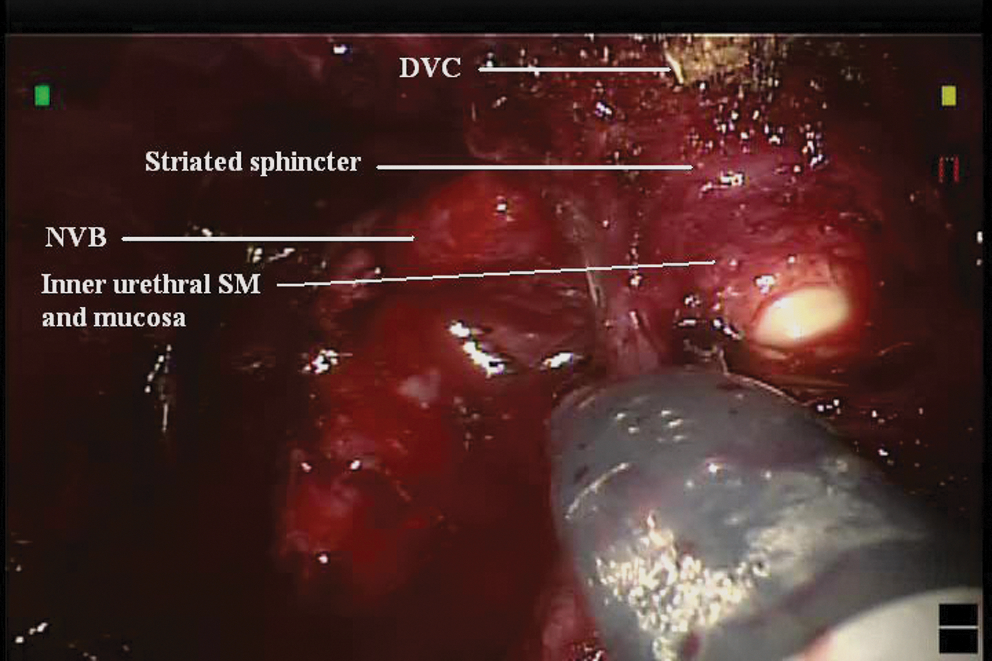
Different components of the sphincteric mechanism clearly visible. DVC=dorsal venous complex; NVB=neurovascular bundles.
There are various variables that are of potential significance with regard to the preservation of the distal continence mechanism. The shape of the prostatic apex and the location of the verumontanum in relation to the apex can vary. After division of the anterior urethra near the apex, the verumontanum can often be visualized with cephalad retraction of the prostate with the fourth robotic arm. It is ideal to divide the urethra just below the verumontanum posteriorly to preserve as much of the distal sphincteric mechanism as possible. Sometimes, the verumontanum is right at the apex, in which case transection below this level can lead to complete preservation of the continence zone (Fig. 5a). This is not always possible, however, because in most patients, a posterior lip of the prostate apex extends beyond the level of the verumontanum (Fig. 5b). In fact, the division of the posterior urethra at this level should be made in a tangential fashion to avoid positive margins in this area. 7
Urethra after anterior division with cephalad traction.
The superior continence outcomes of longer membranous urethral lengths on preoperative MRI have been reported by some investigators. Coakley and colleagues 8 showed that membranous urethral length was associated with faster return to stable postoperative continence. Likewise, Paparel and associates 7 compared the change in MRI-measured membranous urethral length (MUL) and return to continence. 7 Longer preoperative and postoperative membranous urethra as well as decreased MUL loss ratio was associated with a faster return to continence. The concept of restoration of the functional urethral length intraoperatively has also been examined. The Rocco suture is based on the reconstruction of the posterior sphincteric support mechanism. 9 Likewise, Nguyen and colleagues 10 have postulated that their technique of anterior and posterior reconstruction effectively increases the functional urethral length. Both groups have based their reconstruction on the relationship between the length of the membranous urethra preoperatively and its positive impact on continence.
In a retrospective case series, Van Randenborgh and coworkers 11 looked at the effect of urethral length and continence. Of 610 patients who had standard excision of the urethra vs a group of 403 patients who underwent careful dissection of the distal intraprostatic urethra, the urethral length preservation (ULP) group had a significantly earlier return to continence (no pad use, 76% vs 89%). Thirty-three percent of the ULP group was fully continent within 1 month of surgery vs 15% of the standard RP group (P<0.001). Interestingly, fewer positive margins were reported in the ULP group. The impact of MRI-measured membranous urethral length on continence has also been evaluated after radical cystectomy and orthotopic bladder substitution. 12 A study of 40 male patients who underwent radical cystectomy and orthotopic ileal substitution for bladder cancer revealed that there was no significant correlation between preoperative membranous urethral length and time to stable day or night continence.
Contrary to other studies, we could only demonstrate a correlation that approached significance regarding preoperative measurements and continence. None of the above mentioned studies, however, used intraoperative measurements of urethral lengths and correlated that with continence outcomes. We were able to demonstrate that stretched and cut urethral lengths were significantly associated with a faster time to full continence. A cut urethral stump length of at least 2 cm appears to be a significant predictor of time to pad-free state. Therefore, every effort should be made to maximize the length of the urethral stump intraoperatively.
Because there are different definitions of what is perceived as continence in the RP literature, we used the ICIQ scoring system to gain a better understanding of the patient's own perception of their continence status. Patients can be pad free, but yet have leakage and not perfect quality of life once queried. In our cohort, 89% were pad free at last follow-up. We were able to demonstrate a trend toward better CQOL (lower ICIQ scores) with increasing overall length of the distal intramural sphincter mechanism intraoperatively, as well as membranous urethral length on eMRI.
Interestingly, when looking at cut length (urethral stump length) as a function of age, the effect of cut length seemed to be more pertinent for the older patient (age >60 y). With advancing age (over 60 y), the length of the urethral stump was predictive of faster continence recovery. Although our study does not elucidate an explanation for this finding, a possible explanation can be presumed atrophy of the pelvic floor muscles and weakening of the pelvic floor with advancing age. In terms of margins status, we did not find any association with margin positivity or location and preserved urethral length. In our study population, only 13 patients had T3 disease and only 3 had focal positive surgical margins at the apex. We do not believe that the apical dissection compromised the cancer operation. The overall margin positivity rate in this series is reflective of the inner-city urban nature of our medical center and the high-risk population it serves.
The limitations of this study include the relatively small sample size, which can limit power especially on multivariate analysis. We also used the ICIQ scoring system, which is a relatively simplified version of CQoL. We have found that in our predominantly inner-city population with limited higher education, however, more complex scoring systems are confusing and often not completed correctly. We have found the ICIQ system a reliable gauge of continence status and perception of CQOL in our population.
Conclusion
Longer stretched and cut urethral lengths appear to correlate with faster return to a pad-free state. Attention to maximal preservation of the distal continence mechanism is important for optimal continence outcomes after RALP. This is especially true for older patients in whom longer cut urethral lengths appear to correlate with faster return to a pad-free state.
Appendix
The International Consultation of Incontinence Modular Questionnaire is a validated questionnaire to assess urinary continence and its impact on quality of life. It comprises three scored items and an unscored self-diagnostic item. It allows the assessment of the prevalence, frequency, and perceived cause of urinary incontinence, as well as its impact on everyday life. 13
Footnotes
Disclosure Statement
No competing financial interests exist.