
Abstract
Background and Purpose:
Laser energy has gained widespread use, not only in stone treatment, but also in multiple endourologic procedures such as endopyelotomy and incision of ureteral strictures. Furthermore, laser use gains access to open, laparoscopic, and robot-assisted surgery. Therefore, potential complications, such as fiber breakage and detection of these radiolucent fiber remainders, may become of interest. The aim of this study was to evaluate a prototype of a radiopaque laser fiber that was designed for lithotripsy with a holmium:yttrium-aluminum-garnet laser.
Materials and Methods:
A gold-clad 200-μm optical laser fiber was evaluated for its influence on deflection, fiber degradation, as well as radiopaque property in vitro and in vivo. The results were compared with a commercially available 200 μm optical core lithotripsy fiber.
Results:
The gold-clad prototype fiber showed radiopaque property in vitro as well as in vivo, although high body mass index reduces visibility. Introducing the fiber into a flexible ureteroscope had no influence on deflection properties or the diameter of the fully deflected tip. Fiber burn was considerably low and comparable to that of the standard fiber.
Conclusion:
The 200 μm optical core gold-cladd fiber prototype offers comparable performance to a commercially available fiber of the same optical core diameter. Radiopaque property was proven in vitro as well as intracorporeally, thereby adding an additional safety feature to laser treatment in endourology as well as in laparoscopic and robotic surgery.
Introduction
To use these surgical approaches, laser energy is transmitted from the laser generator to the desired object via silica fibers. A complication unique to these fibers is the risk of fiber breakage throughout the procedure, leading to fiber leftovers within the urinary tract. Ideally, these snippets have to be removed to avoid secondary encrustation, as reported by Cinman and associates 2 or possible perforation of intra-abdominal organs. Finding radiolucent silica fiber remnants, however, can be challenging within the urinary tract, but even harder in an intra-abdominal laparoscopic or open procedure.
To overcome this potential hazard, a radiopaque laser fiber may be advantageous. The aim of this study was to evaluate the performance in an in-vitro and in-vivo setting, using a prototype of a gold-clad radiopaque laser fiber.
Materials and Methods
A 200-μm optical silica core flexible fiber for Ho:YAG laser lithotripsy, with an optical silica cladding of 220 μm, was gold clad to achieve radiopaque behavior and fluoroscopic visibility of this fiber. By adding the gold cladding, the outer diameter of the fiber, including the gold cladding, increased to 255 μm. Adding the buffer (280 μm), the outer fiber diameter of the finished radiopaque device is 535 μm, adding 35 μm compared with the standard fiber. The fiber performance of this prototype (GF-1, LISA laser products, Katlenburg, Germany) was evaluated in vitro and in vivo and assessed against a commercially available, reusable 200 micron optical core fiber (outer diameter: 1.3F, min. bending radius 15 mm; LithoFib,™ LISA laser products, Katlenburg, Germany).
In-vitro evaluation included visibility under fluoroscopy in air and within a body phantom, in which the delay block was 15 and 30 cm of water. After approval of the Institutional Review Board, in-vivo assessment enclosed visibility of the fiber within the renal collecting system with and without contrast dye. The patients gave informed consent before fiber testing in vivo.
Fiber flexibility, as well as fiber burn was evaluated in vitro under standardized conditions. Deflection capacity was tested after fiber introduction into a new flexible ureterorenoscope (Cobra, Richard Wolf, Knittlingen, Germany), measuring deflection angle of the empty and the loaded scope using a protractor. To evaluate fiber degradation, the fiber was cut, cleaved, and laser lithotripsy was carried out in a water bath using phantom stones (plaster of Paris) and a standardized laser output of 8 W (0.8 J, 10 Hz, Sphinx, LISA laser products, Katlenburg, Germany). Total energy delivery was limited to 500 J per measurement. Fiber tip degradation was determined using a micrometer. All measurements were performed five times.
Statistical analysis was carried out using SPSS statistical software (Chicago, IL). The data were analyzed using unpaired t test. A probability of P<0.05 was considered statistically significant.
Results
In-vitro examination proved radiopaque property of the tested fiber in air, as well as under 15 and 30 cm water columns (Fig. 1). During in-vivo examination in two patients (A. body mass index [BMI] 21.48; B. BMI 30.34), again the new fiber proved to be radiopaque (Figs. 2A, B). Visibility was reduced, however, in the patient with the high BMI. The standard LithoFib fiber was not detectable in either case. After using contrast dye, no fibers were detectable under fluoroscopy.
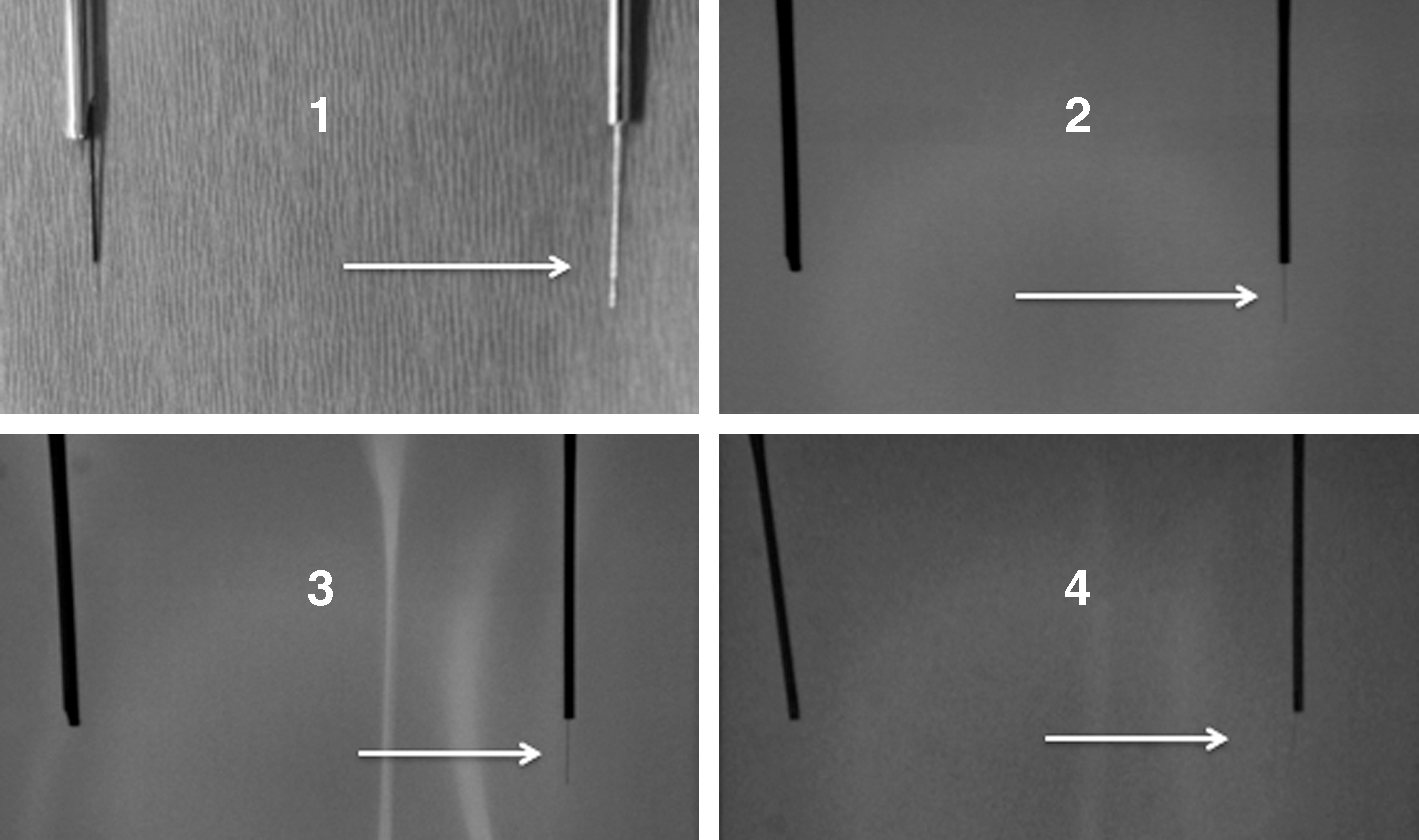
In-vitro evaluation of radioopaque properties.
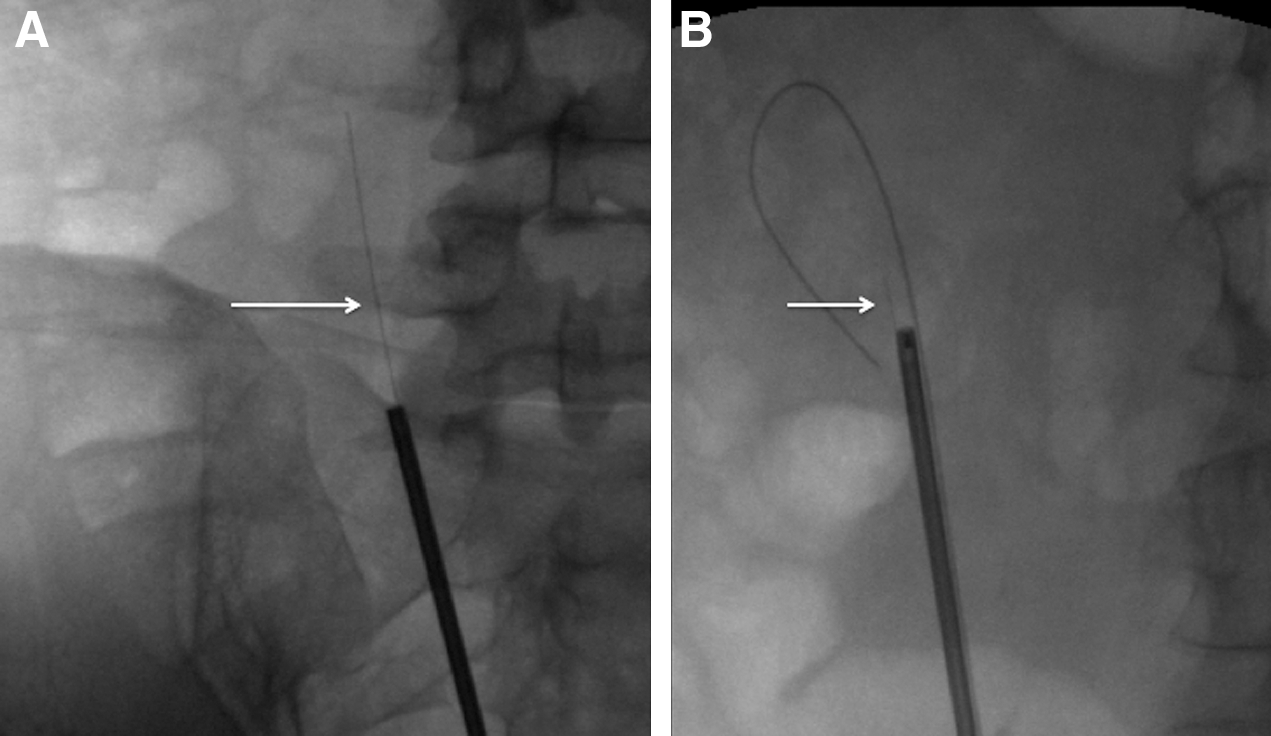
In-vivo evaluation of radioopaque property.
The evaluation of the deflection showed no differences between maximum deflection angles in the empty as well as in the loaded scope. Maximum deflection angle of 270 degrees could be reached with both fibers. The inner diameter of the fully deflected tip of the ureteroscope was 22 mm in the empty ureteroscope and did not increase with any of the tested fibers within the working channel.
Fiber degradation measurements did not show significant differences (P=0.671). Fiber burn was 103.2 μm (±4.7 μm) in the gold-clad fiber and 102.2 μm (±4.3 μm). In both fibers, the complete fiber layers, including the gold cladding, burned back equally.
Discussion
With the widespread use of laser energy in endourology but also growing interest in laparoscopic as well as in robot-assisted surgery, 4 –6 potential hazards of this technique become of interest. To deliver the laser energy to the target, low-OH silica optical core fibers, with fluorine doped silica cladding, are used as the energy transmitter. 7,8 One of these potential complications is fiber tip breakage during the procedure, with the consequent need to remove this foreign body to avoid encrustation or possible perforation of intra-abdominal structures. 2 Small caliber fibers in particular, as used in endoscopic treatments, are more susceptible for intraprocedure damage. 9 Because these commonly used laser fibers are radiolucent, finding this foreign bodies can be a time consuming and frustrating procedure, even in the small compartment of the renal collecting system. One can imagine that losing fiber material within the abdominal cavity can be even more challenging.
To overcome this problem, the use of a radiopaque laser fiber may be a potential solution. Before achieving radiopaque behavior of the fiber, different questions have to be answered. First, the material has to be biocompatible, 10 the molecular structure has to guarantee radiopaque behavior already with little amounts of the used material, because fiber diameter is a crucial issue in endourology. 11 One possible solution for this problem is to add a secondary gold cladding to a silica core fiber.
Radiopaque biocompatible behavior is one issue. The main focus, however, still is functionality. Therefore, thorough evaluation of new fiber types is mandatory. To assess functionality of a small caliber fiber used for calculi fragmentation, different issues are of interest, including fiber degradation during use 12 and the influence on flexibility and performance of a flexible ureteroscope. 13 The presented results showed comparability of the GF-1 prototype with an equal-sized, commercially available fiber. As expected, both fibers did not influence the maximum deflection angle as well as the inner diameter of the fully deflected scope in a latest generation ureteroscope. 14
Fiber burn was considerably low in both fiber types and comparable to results published in the literature. 12 One reason may be the applied energy settings (0.8 J, 10 Hz). Increasing pulse energy higher than 1 J is known to escalate fiber degradation, especially in small caliber fibers. 15
Radiopaque behavior of the GF-1 fiber was demonstrated in vitro as well as in vivo. With rising BMI of the patient, fiber detection becomes more delicate, but still detectable. Despite visibility of the gold-clad fiber in a body model as well as in vivo, it remains unclear if small snippets can be easily visualized once lost in the urinary tract or in the abdominal cavity after surgery and if fiber remnants may be a problem at all. In general, it can be assumed that a fiber snippet in the urinary tract can pose as a possible nidus—eg, for stone formation. Furthermore, one may anticipate that increasing use of laser technology in laparoscopic or robot-assisted surgery may lead to the problem of “lost” long-living fiber snippets, with consequences still to be determined. After proving the concept of radiopaque laser fiber technology for Ho:YAG laser lithotripsy, further testing will be needed to evaluate the behavior of larger caliber fibers to transmit higher amounts of energy. This testing will need to include animal studies to evaluate detectability of small fiber remnants.
Conclusion
The GF-1 200-μm optical core gold-clad fiber prototype offers comparable performance with a commercially available fiber of the same optical core diameter. Radiopaque property and concept were proven in vitro as well as intracorporeally. Further studies need to investigate in-vivo fragmentation behavior in this fiber type, as well as functionality in larger caliber fibers.
Radiopaque fiber cladding may add an additional safety feature to laser treatment in endourology as well as in laparoscopic and robot-assisted surgery.
Footnotes
Disclosure Statement
Drs. Gross and Bach are consultants for Cook Urology. For Dr. Hermann, no competing financial interests exist.