
Abstract
Purpose:
The goal of this study is to identify the most efficient sweeping angle (SA) during photoselective vaporization of the prostate (PVP).
Materials and Methods:
Experiments were conducted with GreenLight XPS™ laser at 120 and 180 W. Ten blocks of porcine kidney were used for each SA (0, 15, 30, 45, 60, 90, and 120 degrees). Vaporization efficiency was assessed by the amount of tissue removed per time. The coagulation zone (CZ) thickness was also measured.
Results:
Maximal vaporization rate (VR) was achieved at SA 15 and 30 degrees. Irrespective of power, VR increased and CZ decreased linearly with decreasing SA from 120 to 30 degrees. The CZ was the thinnest at SA 30 degrees.
Conclusions:
Optimal vaporization occurred at a SA of 15 degrees and 30 degrees with the lowest CZ at 30 degrees. Contrary to a previous recommendation for a wider SA (60 degrees or greater), a narrower SA (30 degrees) achieved the maximal tissue vaporization efficiency.
Introduction
For these reasons, we investigated whether alterations in SA affect vaporization efficiency by applying a scientific approach to elucidate principles for PVP technique.
Materials and Methods
We used an in vitro model of isolated, porcine kidneys for testing tissue vaporization. Ten 2.5×2.5×1.5 cm blocks were used for each SA at 120 and 180 W (n=140). During vaporization, each tissue block was placed cortex side up in a tissue holder. 13
A 180 W 532 nm lithium triborate (LBO) laser and fiber delivery system (GreenLight XPS™ and MoXy™ liquid cooled fiber; American Medical Systems, Inc, Minnetonka, MN) were used. Tissue vaporization was performed at this system's customary powers of 120 and 180 W by a surgeon who was experienced with clinical PVP. For all experiments, laser fiber sweeping was performed with a fixed sweeping speed of 0.5 sweep/sec. Seven different SAs (0, 15, 30, 45, 60, 90, and 120 degrees) were selected. SA is defined as the total angle of rotation through the midpoint, which is at 90 degrees to the tissue. Specimens were fixed in a metal tissue holder with a screw-tight top plate containing a 1.5×1.5 cm aperture. 14
Computer-assisted motors enabled the relative movement of the laser-fiber tip along the tissue surface (x-axis) at a fixed speed of 2 mm/sec while maintaining a fixed 2-mm working distance between fiber and targeted tissue (z-axis). 13,14 The sweeping speed was maintained at 0.5 sweep/sec by manual synchronization of the laser-fiber movement with a metronome, while the side-to-side SAs (y-axis) were achieved by visual monitoring of a protractor attached to the laser fiber.
Vaporization efficiency was assessed by measurement of the vaporization rate (VR) from tissue cavity volume created. 14 The first and last 2.5 mm tissue sections were excluded to obtain more consistent volume estimations. The treated tissues were dissected into 10 specimens 1 mm thick. Each tissue cross-section was imaged by a 9.1 M DSC-H50 digital camera (Sony®) and each cross-sectional area was measured with Image-Pro Plus image processing software (Media Cybernetics, Bethesda, MD). All measured areas of each specimen were integrated to quantify the eventual vaporization volume. Coagulation zone (CZ) thickness at five different locations (3, 5, 6, 7, and 9 o'clock on the crater) and vaporization depth were measured by imaging (see Fig. 1). 14 We decided SA 60 degrees to be the standard for % difference. 15 Statistical analysis was performed with the two-sample Student t test with a P value<0.05 considered statistically significant.
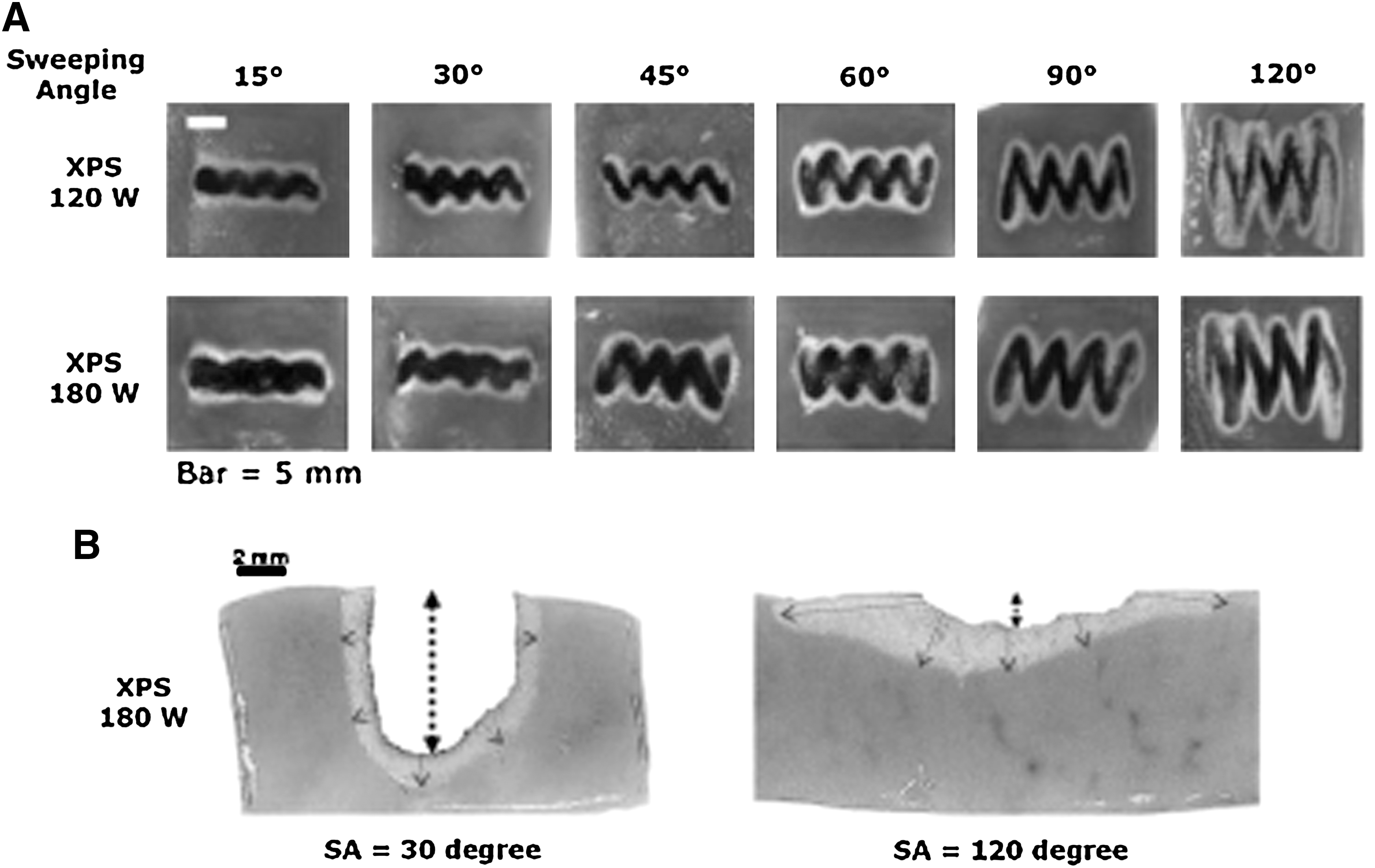
Comparison of vaporized porcine kidney tissue images.
Results
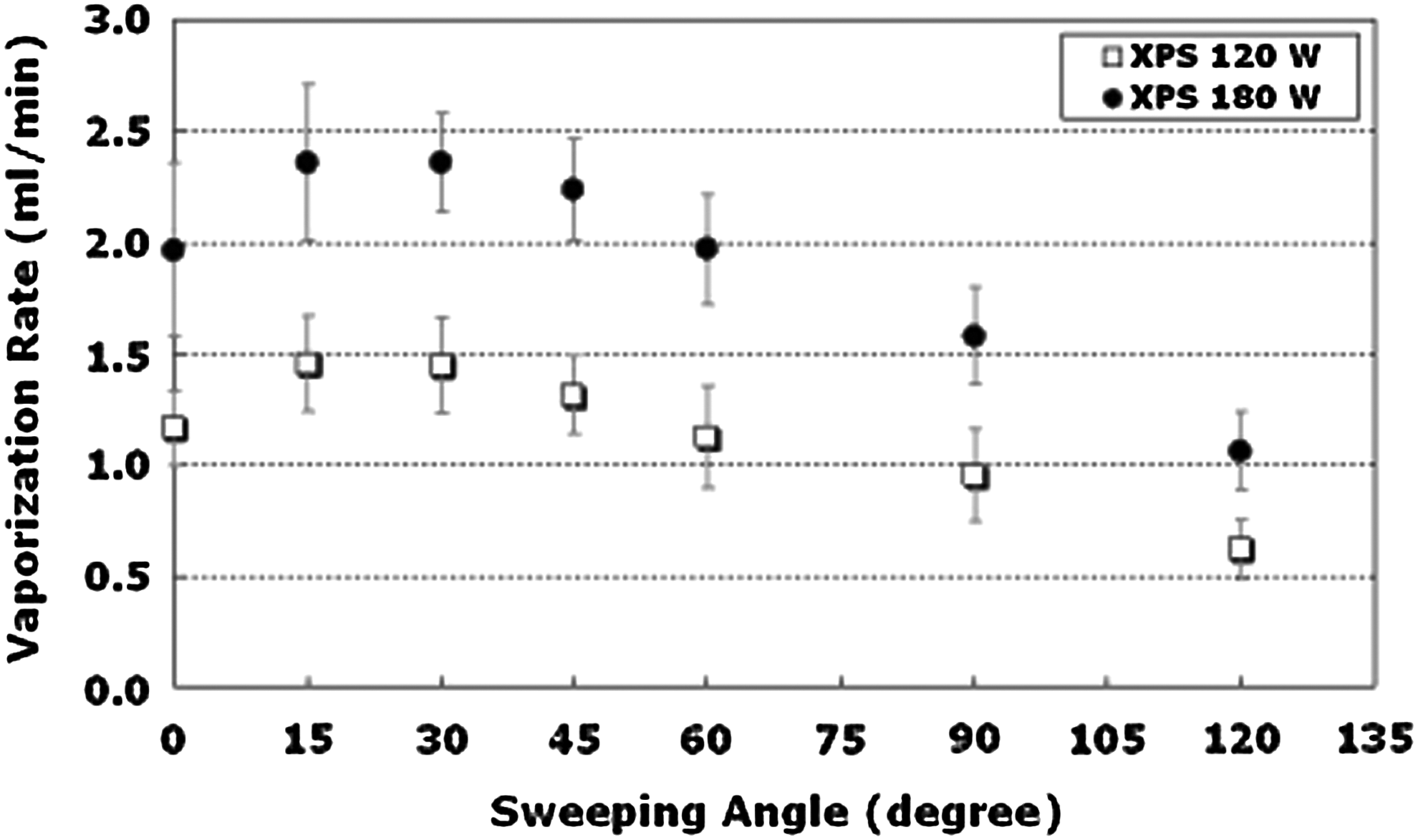
The highest mean of VRs in 120 W was 1.5±0.2 mL/min at SA 15 degrees, and 2.4±0.3, 2.4±0.2 mL/min at SA 15 degrees and 30 degrees in 180 W (Table 1). The percent difference of VR between 120 and 180 W was statistically significant at each SA (P<0.005). VRs at 180 W were 62% to 75% higher than those at 120 W, and VR showed similar changes in both powers.
SA=sweeping angle; VR=vaporization rate (mL/min); CZ=coagulation zone; VD=vaporization depth.
Figure 2 displays the overall trend of VR as a function of SAs. Irrespective of power, VR increased and then saturated as SA increased from 0 degrees to 30 degrees. The percent difference of VR with 60 degrees was statistically significantly increased with SA of 15 degrees and 30 degrees (29.5% and 28.6%; P=0.007 and P<0.005, respectively) at 120 W, and SA 15 degrees, 30 degrees, and 45 degrees (19.9%, 20.0%, and 13.6%; P<0.005, P<0.005, and P=0.03, respectively) at 180 W (Table 2). The maximum VR for the SAs was shown at 15 degrees and 30 degrees in both powers.
Vaporization rate as function of sweeping angle at two different power levels.
SA=sweeping angle; VR=vaporization rate (mL/min); CZ=coagulation zone.
The mean of the CZ initially decreased as SA increased from 0 degrees to 30 degrees, but CZ gradually increased later beyond SA 30 degrees (Table 1). At SA 15 degrees and 30 degrees, the means of CZ were 0.8±0.2 mm and 0.7±0.1 mm, and the percent difference with 60 degrees was−17.0% and −18.9% (Table 2). Laser energy coagulated the least around the vaporization specimen tissue at SA 30 degrees. At SA 15 degrees and 30 degrees, the vaporization results were similar at 120 and 180 W. SA 30 degrees created a relatively wider groove than SA 15 degrees whereas SA 15 degrees generated a narrow, elongated groove in cross-section (Fig. 3).
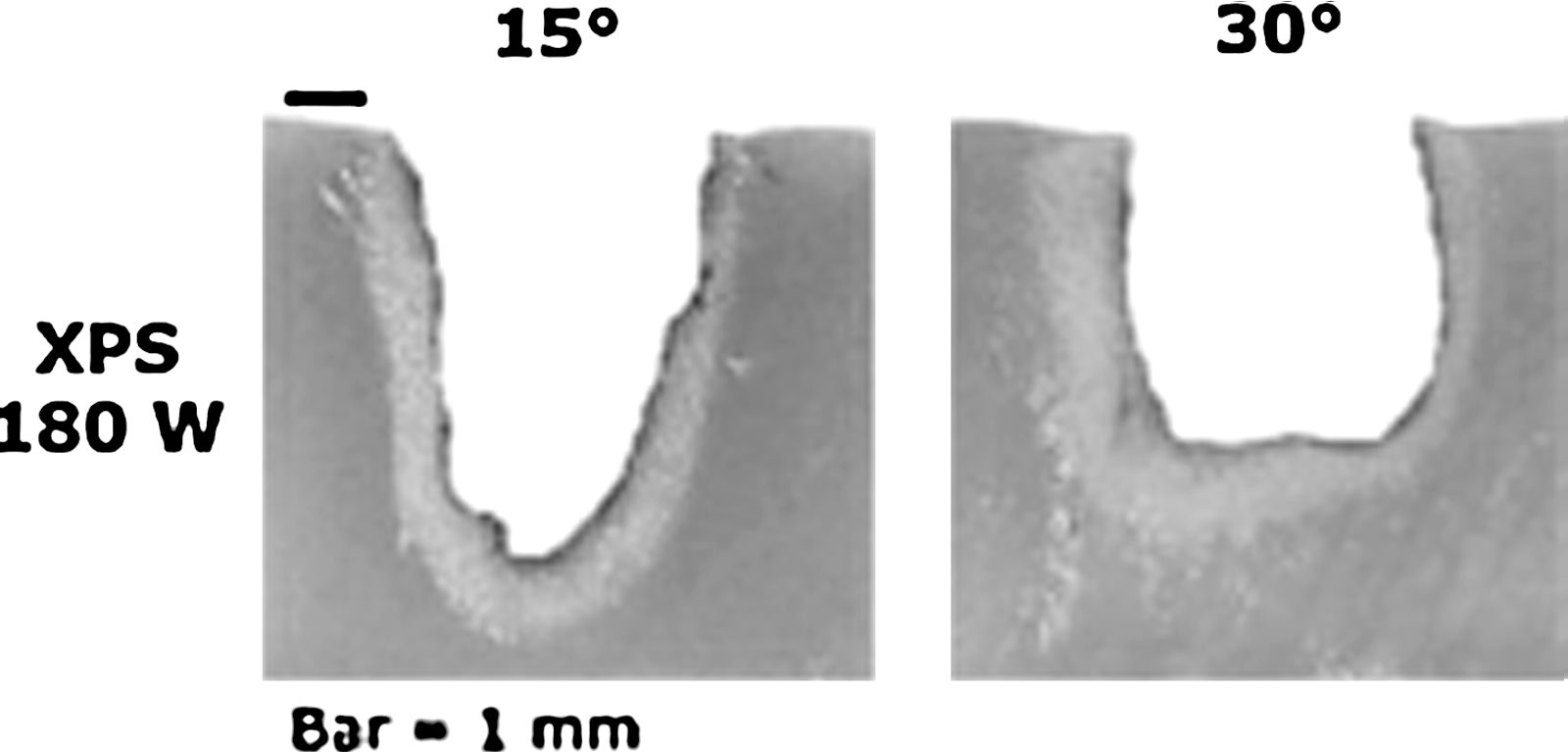
Images of cross-section vaporized with 180 W at two different sweeping angles (SA). The groove at SA 15 degrees is more elongated than at SA 30 degrees. The tissue was evenly vaporized at SA 30 degrees from top to bottom because the cross-sectional image seems U shaped, which reduced the remnant tissue between the grooves.
Discussion
Among the laser devices, the wavelength 532 nm (KTP, LBO) laser is commonly used because of its sustainable outcomes after surgery. 16 –20 While the mechanical aspects of PVP have evolved, the fundamental surgical technique during the PVP, such as laser-fiber sweeping motion, received little attention. There are no universally accepted parameters, and scientifically proven recommendations are very rare.
Gomez Sancha and colleagues 7 recommended using the SA 60 degrees for vaporization in the 80 W PVP laser system because keeping a short distance between the laser fiber and tissue was thought to be an important factor for efficient tissue vaporization by several experts' opinions. Contrary to previous recommendations, we found that a narrow SA (30 degrees) achieved a greater vaporization; the VR linearly increased at both powers as the SA decreased from 120 degrees to 30 degrees. This would result in a lower power density than vaporization threshold, thus producing a more coagulative effect. 7
As the SA further decreased from 15 degrees to 0 degrees, we did not see any increase in the VR, but rather reduction of it. A feasible explanation for this outcome can be a longer vaporization pathway at SA 15 degrees (ie, zigzag pattern on tissue) from fiber sweeping than at SA 0 degrees. Because vaporization depths at SAs of 0 degrees and 15 degrees were found to be similar in this study, it is conceivable that the difference in power density at these angles would be minimal. On the other hand, once the fiber is swept, the beam area can cover a larger area to vaporize. Hence, minimal change in power density but longer pathway of tissue vaporization at a SA 15 degrees can achieve a relatively higher vaporization rate than at SA 0 degrees.
Laser-tissue effects can be categorized as either vaporization with resulting immediate tissue vaporization or coagulation followed by delayed tissue sloughing. 21 Once tissue is coagulated, it is quite difficult for the remaining laser energy to attain appropriate vaporization because of reduced light absorption. For BPH therapy, coagulation makes the procedure imprecise and can be especially hazardous, especially in important anatomic areas such as the external sphincter. The coagulated tissue is also associated with the irritative voiding symptoms after surgery. 21
We found that the degree of thermal coagulation ensuing vaporization, as expressed in CZ, increased linearly as SA increased from 30 degrees to 120 degrees. As the SA increased above 30 degrees, the beam area at the tissue surface was wider and distance from the laser fiber to the tissue was increased, which reduces vaporization efficiency and increases coagulation. 7,13 SAs of 15 degrees and below also showed an increased CZ than at SA 30 degrees (Table 1). While SAs of 15 degrees and below provided much longer irradiation times to create the deeper grooving of tissue as we mentioned above, these SAs may result in increased thermal damage in the form of deeper coagulation. 13,22 This phenomenon is seen through cross-sectional images where vaporized area was U shaped at SA 30 degrees but V shaped at SA 15 degrees even though both had the similar total volume vaporized (Fig. 3). The tissue was vaporized evenly from top to bottom when the cross-sectional images are U shaped, which reduced the remnant tissues between the grooves. This may have important clinical implications where grooved defects can result in an uneven tissue surface, higher risk for perforation, and more difficult hemostatic control. For these reasons, although the VR was similar at SA 15 degrees and 30 degrees, a SA 30 degrees was the most efficient for tissue vaporization regardless of the laser power and produced less tissue coagulation than other SAs.
To date, this remains the first data for the laser-fiber sweeping technique with the 180 W 532 nm LBO laser based on a scientific investigation rather than based on surgeon experience or opinions.
We believe that this experiment may be useful for clinical training of urologists in the PVP laser system.
Conclusions
In this experiment, the most efficient SA for tissue vaporization occurred at 30 degrees regardless of the laser power. As SA increased from 0 degrees to 30 degrees, VR increased and CZ narrowed. Beyond SA 30 degrees, VR abruptly decreased and the CZ began to thicken, indicating that a wider sweeping angle (greater 30 degrees) will cause less efficient vaporization and more tissue coagulation. This study highlights the fundamental principles of PVP for practicing urologists.
Footnotes
Disclosure Statement
Funding for this study was provided by American Medical Systems, Inc.