
Abstract
Purpose:
To assess the intrarenal arteries injuries after cranial pole nephrectomy in a pig model to compare these findings with those in humans.
Materials and Methods:
Polyester resin was injected through the ureter and the renal artery to make three-dimensional casts of 61 pig kidneys. The cranial pole of the kidneys was sectioned at four different sites before the solidification of the resin, and the casts were examined for arterial damage.
Results:
Section performed through the hilus (15 kidneys): The cranial division of the renal artery was sectioned in two (13.33%) cases, the ventral branch of the cranial division of the renal artery was sectioned in 13 (86.7%) cases, and the dorsal branch of the cranial division of the renal artery was sectioned in 11 (73.34%) cases. Section at 0.5 cm cranial to the hilus (16 kidneys): The cranial division of the renal artery was sectioned in 1 (6.25%) case, the ventral branch of the cranial division of the renal artery was sectioned in 14 (87.5%) cases, and the dorsal branch of the cranial division of the renal artery was sectioned in 13 (81.25%) cases. Section at 1.0 cm cranial to the hilus (15 kidneys): The ventral branch of the cranial division of the renal artery was sectioned in five (33.33%) cases, and the dorsal branch of the cranial division of the renal artery was injured in five (33.33%) cases. Section at 1.5 cm cranial to the hilus (15 kidneys): No lesions were found in the main arteries, only in the interlobular branches.
Conclusions:
As previously demonstrated in humans, sections at 1.0 cm or more cranially to the hilus in pigs also showed a significant decrease in damage to the major intrarenal arteries. Therefore, as regards arterial damage, the pig kidney is a useful model for partial nephrectomy in the cranial (upper) pole.
Introduction
The main problems in partial nephrectomy are bleeding, lesions to remaining arteries, and urinary leakage. Many techniques have been studied in the pig model and humans to control bleeding in LPN. Parenchymal ischemia has been performed using compressive cables 4 –6 or vascular pedicle clamps. 7 –9 Moreover, bleeding during resection has been controlled with unipolar or bipolar cauteries, 4,5,10 ultrasound, 10,11 hydro-jet, 7,12 and laser. 4,9,13 Topical hemostasis on the cut renal surface has also been performed with various types of sealants. 5,8,14
The cranial pole, both in man and pig, is a technical challenge site for OPN and LPN because of its limited visualization and complex arterial relationships, compromising the surgical outcomes, primarily for the novice laparoscopist. 2 This situation necessitates additional training, and the pig kidney is considered the most suitable animal model. The arterial supply to the cranial pole in pigs has been described, 15 showing some differences from humans, 16 such as the relationship between the dorsal artery (retropelvic artery) and the infundibulum of the cranial (superior) major calix. Recently, it was demonstrated that nephrectomies performed at less than 1.0 cm from the hilar zone in the human kidney result in a high incidence of lesions to major arteries. 17
We assessed the injuries of the pig intrarenal arteries, simulating the cranial pole nephrectomy in different transverse section planes. The aim was to compare the results with previous findings in humans 17 to determine if the pig kidney is a suitable model for partial nephrectomy of the cranial pole.
Materials and Methods
Nonfixed kidneys were obtained from adult mixed-breed Duroc and Large-White farm pigs that weighed 60 to 80 kg (mean 72 kg) and were slaughtered at 140 days of age. The institutional animal review committee approved the research protocol.
Intrarenal anatomy (collecting system and arteries) was studied in 61 (29 right and 32 left) three-dimensional endocasts of the collecting system together with the intrarenal arteries. The endocasts were obtained as previously described. 15 Briefly, a yellow polyester resin (2 to 6 mL) was injected into the ureter to fill in the kidney collecting system, and a red resin (5 to 8 mL) was injected into the main trunk of the renal artery to fill in the arterial tree. Three percent methyl ethyl peroxide was added to the resin as a catalyst. Before the complete setting of the resin, while it was still gelatinous, which allowed cutting and avoiding leakage, transverse sections of the cranial pole of the kidney were obtained at different distances from the hilus, simulating the LPN (Fig. 1). The sections were grouped as follows:
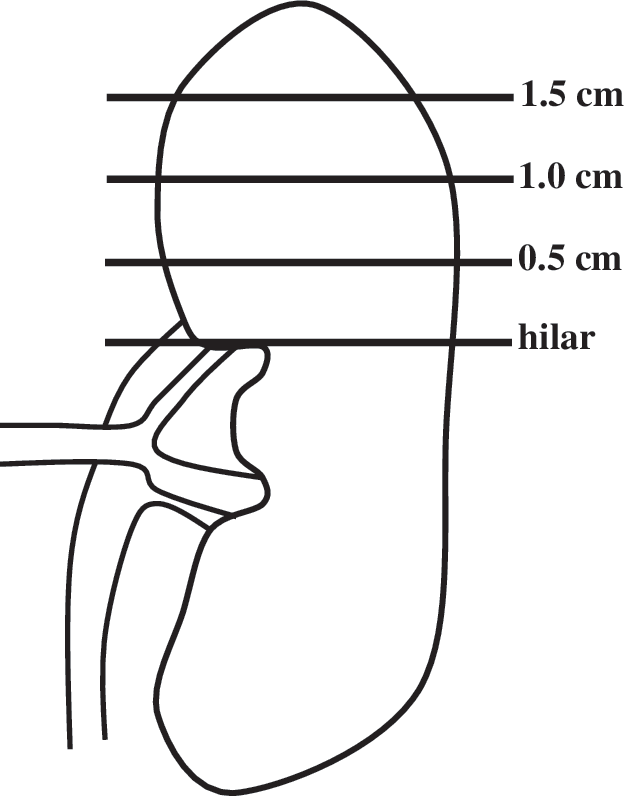
Schematic drawing of the pig kidney, showing the transverse planes where the kidney sections were performed at the hilus (most cranial margin of the hilus), 0.5 cm cranial to hilus, 1.0 cm cranial to hilus, and 1.5 cm cranial to hilus.
Group 1 – hilar section (most cranial margin of the hilus): 15 kidneys (7 right and 8 left)
Group 2 – section 0.5 cm cranial to hilus: 16 kidneys (8 right and 8 left)
Group 3 – section 1.0 cm cranial to hilus: 15 kidneys (7 right and 8 left)
Group 4 – section 1.5 cm cranial to hilus: 15 kidneys (7 right and 8 left)
After setting of the resin (24 hours), perirenal fat was removed, and the kidneys were immersed in a bath of concentrated commercial hydrochloric acid for 48 to 72 hours until total removal of the organic matter was achieved. After corrosion, only the three-dimensional endocasts of the injected systems remained. To preserve the in vivo relationships, one or two arterial branches were fixed to the collecting system.
The casts were analyzed to identify any lesion to the cranial division of the renal artery and its branches: The apical artery, the ventral branch, the dorsal branch, the dorsal hilar branch, and the ventral hilar branch. 15 The distance between the section line and the origin of the hilar branch on the dorsal and ventral surfaces was also recorded.
The differences between groups were tested by one-way analysis of variance and the Tukey test. The Student t test was used to compare damage in the dorsal and ventral hilar branches. P value of 0.05 was considered statistically significant. GraphPad Prism 5.00 software for Windows was used for all analyses.
Results
After endocasts obtainment with the produced intrarenal lesions determined by the sections as described, we found the following results (Table 1):
(1) Section at the hilus (Fig. 2)
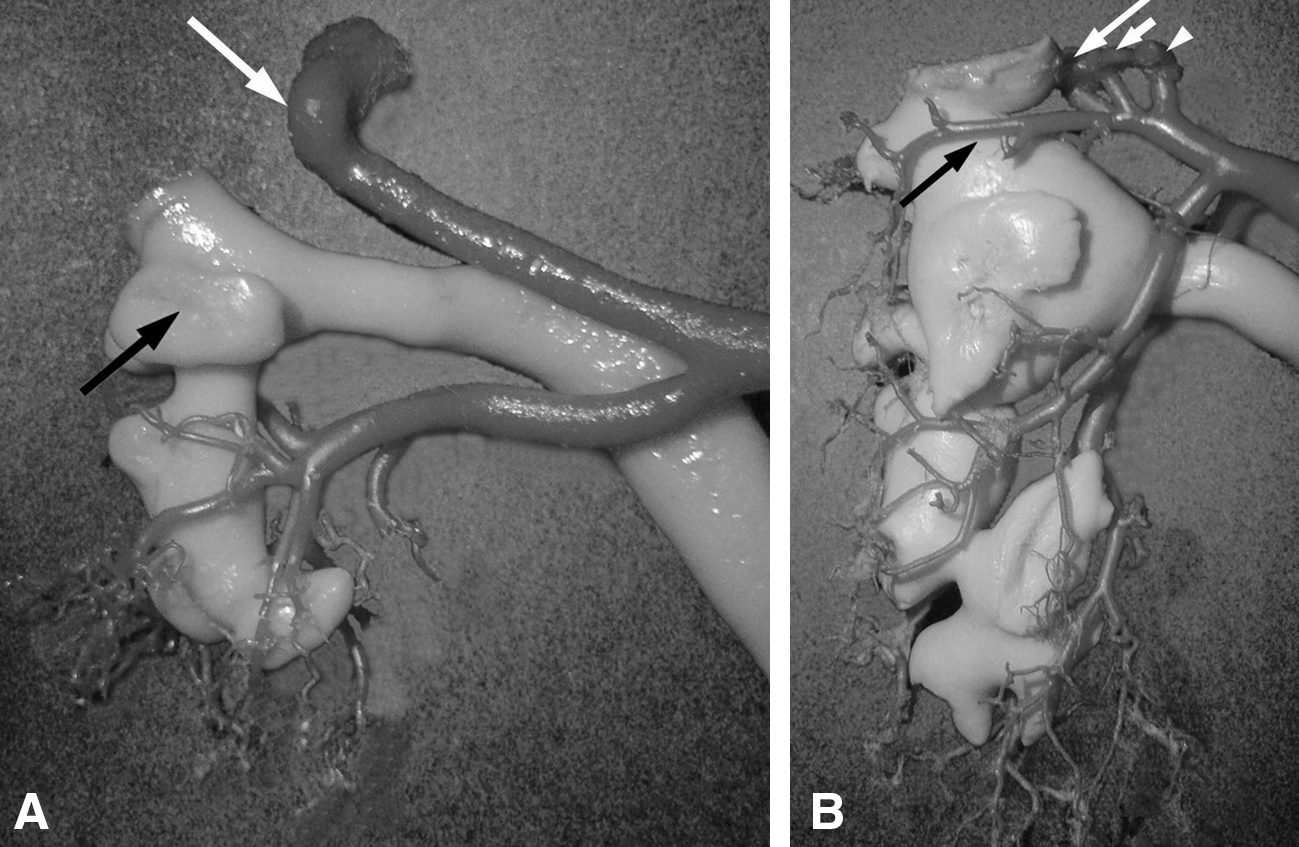
Of the 15 kidneys, the cranial division of the renal artery was totally transected in two cases (13.33%), before its bifurcation. The ventral branch of the cranial division of the renal artery was transected in 13 cases (86.67%), and the dorsal branch of the cranial division of the renal artery was transected in 11 cases (73.34%). The apical artery was injured in all cases when it was present (61.54%). The vascular distribution in the hilar zone was lost in the dorsal and ventral regions in two (13.33%) and three (20%) cases, respectively. The average distances between the section at the hilus and the origin of the hilar branch on the dorsal and ventral surfaces were 0.73 cm and 0.79 cm, respectively (Table 2).
Data are indicated in cm.
SD=standard deviation.
(2) Section at 0.5 cm cranial to the hilus (Fig. 3A)
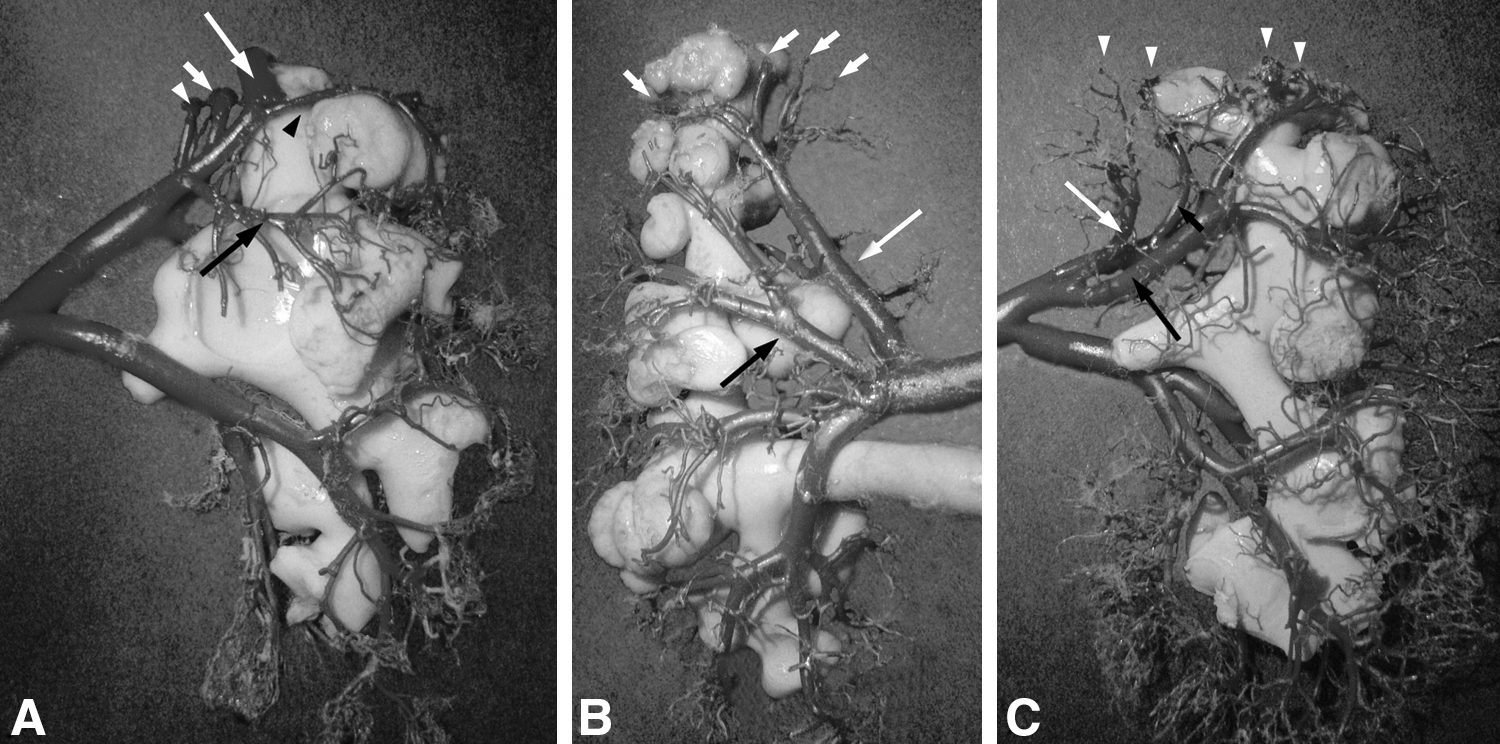
In this group of 16 kidneys, the cranial division of the renal artery was transected in one (6.25%) case, before its bifurcation. The ventral branch of the cranial division of the renal artery was transected in 14 (87.50%) cases, and the dorsal branch of the cranial division of the renal artery was transected in 13 cases (81.25%). The apical artery was transected in all cases when it was present (68.75%). The vascular distribution in the hilar zone was transected in only one (6.25%) case, at the dorsal region. The average distances between the section at 0.5 cm cranial to the hilus and the origin of the hilar branch on the dorsal and ventral surfaces were 1.08 cm and 1.24 cm, respectively (Table 2).
(3) Section at 1.0 cm cranial to the hilus (Fig. 3B)
The 15 kidneys of this group had no damage on the cranial division of the renal artery. The ventral branch of the cranial division of the renal artery was transected in five (33.33%) cases, and the dorsal branch of the cranial division of the renal artery was also transected in five (33.33%) cases. The apical artery was transected in all cases when it was present (53.33%). The average distances between the transverse cut 1.0 cm cranial to the hilus and the origin of the hilar branch on the dorsal and ventral surfaces were 1.67 cm and 1.59 cm, respectively (Table 2).
(4) Section at 1.5 cm cranial to the hilus (Fig. 3C)
In these 15 kidneys, no injury was found to the main arteries. Damage was observed only in the interlobular branches. The average distances between the transverse section 1.5 cm cranial to the hilus and the origin of the hilar branch on the dorsal and ventral surfaces were 2.13 cm and 2.21 cm, respectively (Table 2).
Discussion
Various techniques used in pig kidney surgery have yielded good results, but urinary leakage, 5,10 bleeding during surgery, 4,11 postoperative bleeding, 5,10 and renal necrosis 4 are significant problems in these experimental techniques. Thus, some pigs died from these complications. 4,5,10 Other experimental procedures such as hydro-jet cutting 7,12 and harmonic scalpel without hilar clamping 11 also needed a supplementary coagulation to accomplish hemostasis. Ong and colleagues 18 performed 12 LPN in six pigs using bipolar needle electocautery without hilar clamping. Those pigs needed temporary hilar occlusion in two cases. The main concerns of a LPN in humans are hemostasis and urinary leakage, although in pigs we have demonstrated that urinary leakage is unusual after LPN, even without closure of the collecting system and without the use of a Double-J stent. 19 Recently, many techniques have been investigated in the pig model to solve these problems. 6,14 Despite the fact that it is difficult to compare different procedures, research still continues in an attempt to establish the best way to make the perfect LPN with minimum bleeding.
Blood in the surgical field makes it difficult to identify tumors and the collecting system. 13 Decreased blood loss during surgery is important to obtain better results in partial nephrectomy. In OPN, surgeons can easily control bleeding, but especially when performing laparoscopic procedures, better techniques are needed to control bleeding, such as compressive cables 14 and radiofrequency devices. 20,21 The knowledge of pig kidney intrarenal arteries could help in OPN and LPN research, because the pig is the most suitable animal model for this procedure.
McDougall and colleagues, 4 using cable-tie compression and hilar clamping, observed arterial bleeding from the incised surgical surface in one pig. They suspected that a small upper pole segmental artery had not been included in the hilar occlusion. This artery could be the apical artery that was found in the cranial pole of the pig kidney in 32.97% of cases and can arise from the cranial division of the renal artery, near the renal hilus. 15 Moreover, the apical artery could be difficult to be included in the hilar occlusion because its origin is often precocious. 15 The apical artery, if present, was injured in all cases of sections at less than 1.5 cm from the hilus.
One limitation of this study could be the fact that we did not evaluate the blood flow, because the arterial injuries were assessed ex vivo. Concerning the position of the intrarenal arteries and its relationship with the collecting system, however, the results could be compared with previous findings in humans.
The dorsal branch of the cranial division of the renal artery, in 68.13% of cases, gives a dorsal artery to the dorsal hilar zone. The arterial supply related to the ventral midzone of the kidney is also from branches of the cranial division of the renal artery. 15 When the resection was made at 0.5 cm from the hilus, the cranial division of the renal artery was damaged (6.25%) and the dorsal and ventral hilar zone lost its main blood supply. Actually, this fact may explain other complications, such as urinary leakage 5,10 and renal necrosis 4 described in the pig model.
The retropelvic artery in humans was related to the superior infundibulum in 57.33% of the cases. 16 It has been demonstrated in humans that this artery can be injured in cranial pole nephrectomies with sections at less than 1.0 cm from the hilus. 17 These injuries can lead to loss of an important part of renal tissue, because in humans, this artery can supply more than 50% of the renal parenchyma, 22 while in pigs the main artery is the cranial division of the renal artery, which can supply more than 70% of the renal parenchyma. 23 The retropelvic artery in pigs, when present, supplied only 16.67% of the kidney. 23 Moreover, the retropelvic artery in the pig kidney did not show the same relationship with the superior infundibulum as in humans, suggesting that the cranial pole of pig kidney would not be a good model for transposing to humans. 15
When we evaluated the arterial damage and the loss of renal tissue, however, the findings in pigs were similar to those from humans, 17 although the arterial nomenclature is different. This means that, in terms of importance, the cranial division of the renal artery in pigs is similar to the retropelvic artery in humans. Therefore, the pig kidney is a good model for human partial nephrectomy, as long as the transection is at most 1.0 cm away from the hilus so that a vascular insult similar to what would be encountered in a human is created.
When nephrectomies were performed at the hilus and at 0.5 cm from the hilus, the cranial division of the renal artery was transected in one (6.25%) case, and its ventral and dorsal branches were transected in 14 (87.50%) and 13 (81.25%) cases, respectively. On the other hand, in nephrectomies performed at 1.0 cm and 1.5 cm cranial to the hilus, there was no injury to the cranial division of the renal artery and the arterial supply for the midzone of the kidney was preserved as in the human. 17 In the group in which the sections were performed at 1.0 cm from the hilus, only the dorsal and ventral branches of the cranial division of the renal artery were injured in 33.33%. This demonstrated that the cranial division of the renal artery in pigs is as important as the retropelvic artery in humans, regarding the arterial supply of the hilar region, even presenting a different relationship with the upper portion of the kidney collecting system (Fig. 4).
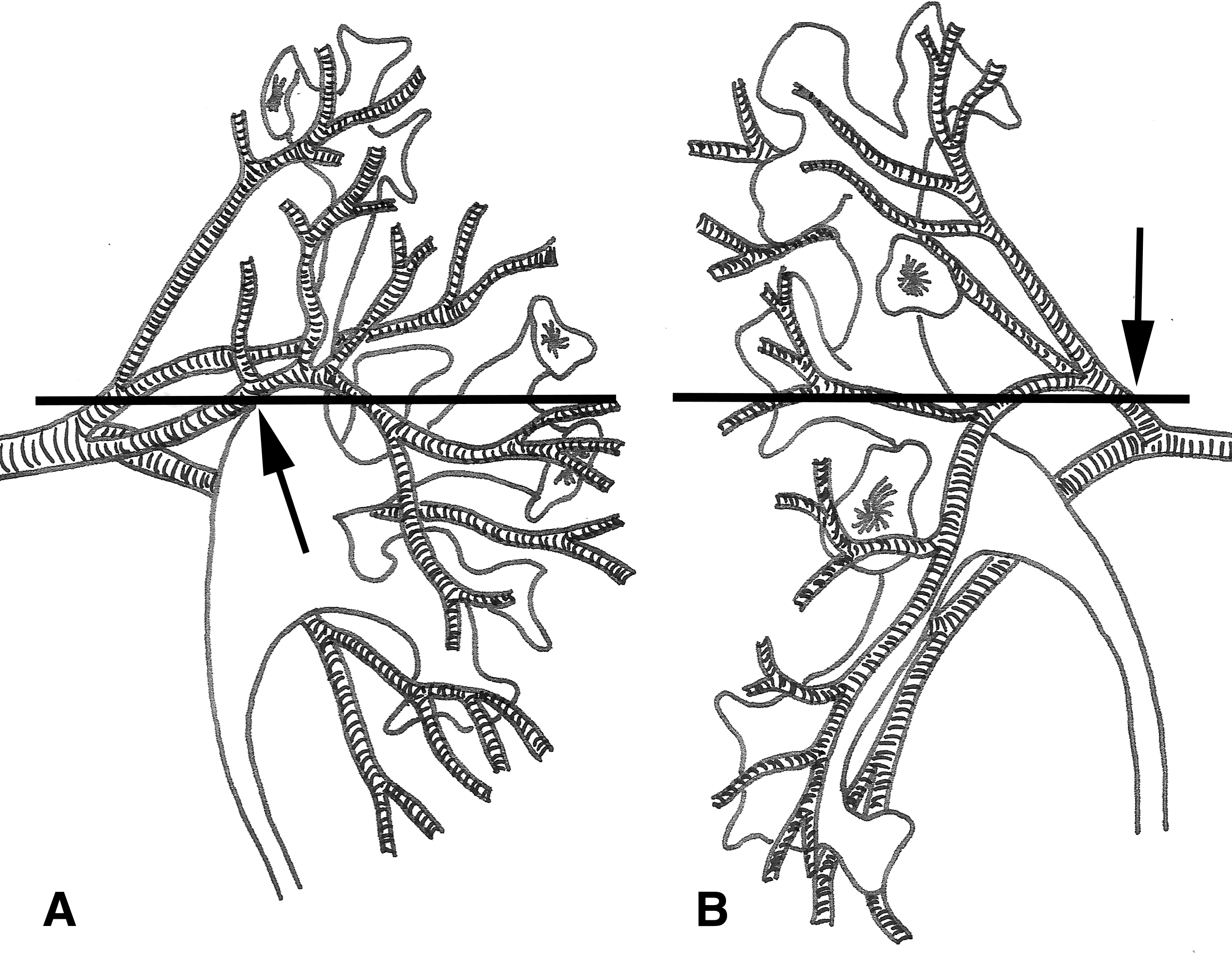
Posterior view of endocast (collecting system and arteries) of human right kidney
There is no difference between the distance from the section plane and the origin of the dorsal and ventral hilar branches, which supply the renal midzone. Considering both dorsal and ventral hilar branches together, the distances between the origin of the hilar branches and the different sites of the section of each group presented a statistically significant difference, as listed in Table 2. Although the distances between the section plane and the retropelvic artery in humans 17 are smaller than the distances between the section plane and the hilar branches in pigs, the groups where the section was performed at more than 1.0 cm cranial to the hilus presented the smallest injury rate of major arteries in humans 17 and pigs. This demonstrated that the arterial damage and the loss of renal tissue in pigs and humans were similar when the partial nephrectomy was performed at the same distance from the hilus, even with different distances between the section plane and the origin of the main arterial supply for the renal midzone.
Conclusion
Although the retropelvic artery in pigs was not related to the superior infundibulum, our results demonstrated that the cranial pole nephrectomy in pigs at less than 1.0 cm from the hilus caused significant damage to the cranial division of the renal artery and its branches (Table 1), leading to significant loss of renal tissue in the renal midzone (Fig. 2A). These findings are similar to the results found in human kidneys 17 and demonstrate that, as regards the arterial damage and loss of renal tissue, the cranial pole of the pig kidney can be useful as an experimental model for partial nephrectomy.
Footnotes
Acknowledgments
This study was supported by grants from the National Council of Scientific and Technological Development (CNPq), Foundation for the Coordination of Higher Educational and Graduate Training (CAPES), and Foundation for Research Support of Rio de Janeiro (FAPERJ), Brazil. The authors are grateful to Richard Medeiros of Medical Editing International for editing the final manuscript.
Disclosure Statement
No competing financial interests exist.