
Abstract
Background and Purpose:
The minimally invasive nature and effectiveness of shockwave lithotripsy (SWL) has made it one of the primary treatment modalities for urinary tract calculi. Several factors determining the success of SWL treatment have been studied, including stone factors (ie, location, size, and composition) and patient factors (ie, patient habitus and skin-to-stone distance). Our objective was to determine if either the assisting radiologic technologist or the amount of fluoroscopy time used has an impact on SWL success.
Patients and Methods:
We compared the outcome of 536 SWL treatments across three radiologic technologists. We also evaluated the average amount of fluoroscopy time used in treatment success vs failures in this same cohort. The outcomes measured were stone-free and successful fragmentation rate at 2 weeks and 3 months. Successful fragmentation was defined as being either stone free, having residual sand, or with an asymptomatic fragment ≤4 mm on radiography of the kidneys, ureters, and bladder.
Results:
The patients treated by the three different radiologic technologists were comparable with respect to body mass index, stone side and location, presence of ureteral stent, and mean stone area (mm2). The stone-free and successful fragmentation rates at 2 weeks and 3 months between the three radiologic technologists were not significantly different. When examining fluoroscopy time, we found a significantly greater mean fluoroscopy time was used in treatments with successful fragmentation at 2 weeks (3.16 min vs 2.72 min, P=0.0001) and 3 months (3.12 min vs 2.75 min, P=0.0015) compared with treatment failures.
Conclusion:
The radiologic technologist did not have a significant impact on SWL treatment outcome at 2 weeks and 3 months. Successful SWL fragmentation at 2 weeks and 3 months, however, was associated with a greater amount of fluoroscopy time, suggesting that using fluoroscopy to ensure accurate targeting during SWL is important for successful fragmentation.
Introduction
Conversely, little research exists on the effect of operator characteristics on SWL treatment success. The treating urologist has been shown to affect treatment outcome, 10 as well as the learning curve for radiation technologists. 11 To our knowledge, however, both the comparative effect of different assisting radiologic technologists and the effect of fluoroscopy time on SWL treatment outcome have never been examined. Our objective was to determine if either the assisting radiologic technologist or the amount of fluoroscopy time used has an impact on SWL treatment success.
Patients and Methods
Patient selection and provider characteristics
All patients treated at the St. Michael's Hospital Kidney Stone Centre (SMHKSC), in Toronto, Canada, are entered into a prospectively maintained database called Lithotrack.™ Using the Lithotrack database, we completed a retrospective chart review of 546 patients who had undergone SWL between July 2001 and October 2009, for either ureteral or renal stones and had complete 2-week and 3-month follow-up at SMHKSC. All patients were treated with the Phillips Lithotron Ultra electrohydraulic lithotripter under intravenous sedation with propofol, fentanyl, and midazolam. All patients included in the study had only undergone a single SWL treatment; no patients had undergone re-treatment before 2-week or 3-month follow-up.
In total, 11 different urologists performed SWL treatments in the study cohort, with 8 main urologists performing 98.33% of the treatments. Three different radiologic technologists were involved in SWL treatments, and they were rotated in a relatively uniform basis with the various treating urologists. All three radiologic technologists have a similar level of expertise. Technologist 1 has approximately 10 years of experience with SWL, whereas technologists 2 and 3 each has approximately 4 years of experience. All three technologists work almost exclusively in the SWL unit.
Measurement and statistical analysis
Patient demographics (ie, age, sex, and body mass index [BMI]) and stone characteristics (ie, size, location, side, and presence of stent) were recorded for all 546 patients. In addition, provider information (ie, performing radiologic technologist and treating urologist) and treatment parameters (ie, treatment time, amount of fluoroscopy time, number of shocks administered, maximum energy used, and estimated radiation dose for each treatment) were also recorded for all patients. The fluoroscopy time and estimated radiation dose for each treatment are calculated automatically by the Phillips Lithotron Ultra lithotripter.
The outcome measured in all patients was stone-free and successful fragmentation rate at 2 weeks and 3 months, as determined by radiography of the kidneys, ureters, and bladder (KUB) at follow-up. Successful fragmentation was defined as being either stone free, having residual sand, or with an asymptomatic fragment ≤4 mm on KUB radiography.
The chi square test (categorical variables) and analysis of variance (continuous variables) were used to compare the patient demographics, stone characteristics, and treatment parameters across the patient cohorts treated by each technologist. To assess the effect of the radiologic technologist, the chi square test was used to compare treatment outcome (ie, stone-free and successful fragmentation rate at 2 weeks and 3 months) for the 546 SWL treatments across the three radiologic technologists. Next, multivariable logistic regression analysis was performed to adjust for possible confounding of the relationship between radiologic technologist and treatment outcome.
To assess the effect of fluoroscopy time, we compared the mean fluoroscopy time used in treatments with successful fragmentation vs failures using the Student t test. Multivariable logistic regression analysis was then performed to adjust for possible confounding of the effect of fluoroscopy time on treatment success by BMI, presence of stent, stone size, and location. The t test was also used to compare the mean estimated fluoroscopy dose in treatment successes vs failures, to evaluate the resultant difference in radiation exposure between these two groups. All statistical analysis was performed using SAS software version 9.2 (SAS institute, Cary, NC). A P value of 0.05 was used to indicate statistical significance.
Results
Of the 546 patients retrospectively reviewed, complete patient demographics and stone characteristics were available on 536 patients. The BMI was missing for 10 patients (4 for technologist 1, 5 for technologist 2, and 1 for technologist 3). As such, these 10 patients were excluded. The 536 patients treated by the three different radiologic technologists were comparable with respect to age, BMI, stone side and location, presence of ureteral stent, and mean stone area (Table 1). Of note, the groups did differ significantly with respect to sex distribution; however, this was adjusted for using logistic regression analysis (see below). In terms of treatment parameters, the patients treated by the three different radiologic technologists were comparable for mean number of shocks and treatment time (Table 2). The mean maximum voltage across the three technologists approached statistical significance (P=0.05); however, the largest difference, which was between technologistd 2 and 3, was only 0.17 kV. This certainly does not represent a clinically significant difference that would be expected to influence treatment outcome. Nevertheless, similar to sex, this was adjusted for using logistic regression analysis (see below).
P value significant (<0.05).
SD=standard deviation; BMI=body mass index; UPJ=ureteropelvic junction; UVJ=ureterovesical junction.
SD=standard deviation.
Univariate analysis with the chi square test showed that the stone-free and successful fragmentation rates at 2 weeks and 3 months across the three different radiologic technologists were not statistically significantly different (Fig. 1). Logistic regression analysis controlling for the difference in sex distribution and mean maximum voltage across the three groups also showed no significant effect of technologist on successful fragmentation and stone-free rates, respectively, at either 2 weeks or 3 months. Logistic regression analysis was also used to evaluate the effect of the technologist on treatment outcome while controlling for the treating urologist. After adjusting for the treating urologist, the radiologic technologist was still not a significant predictor of stone-free or successful fragmentation rates at 2 weeks or 3 months.
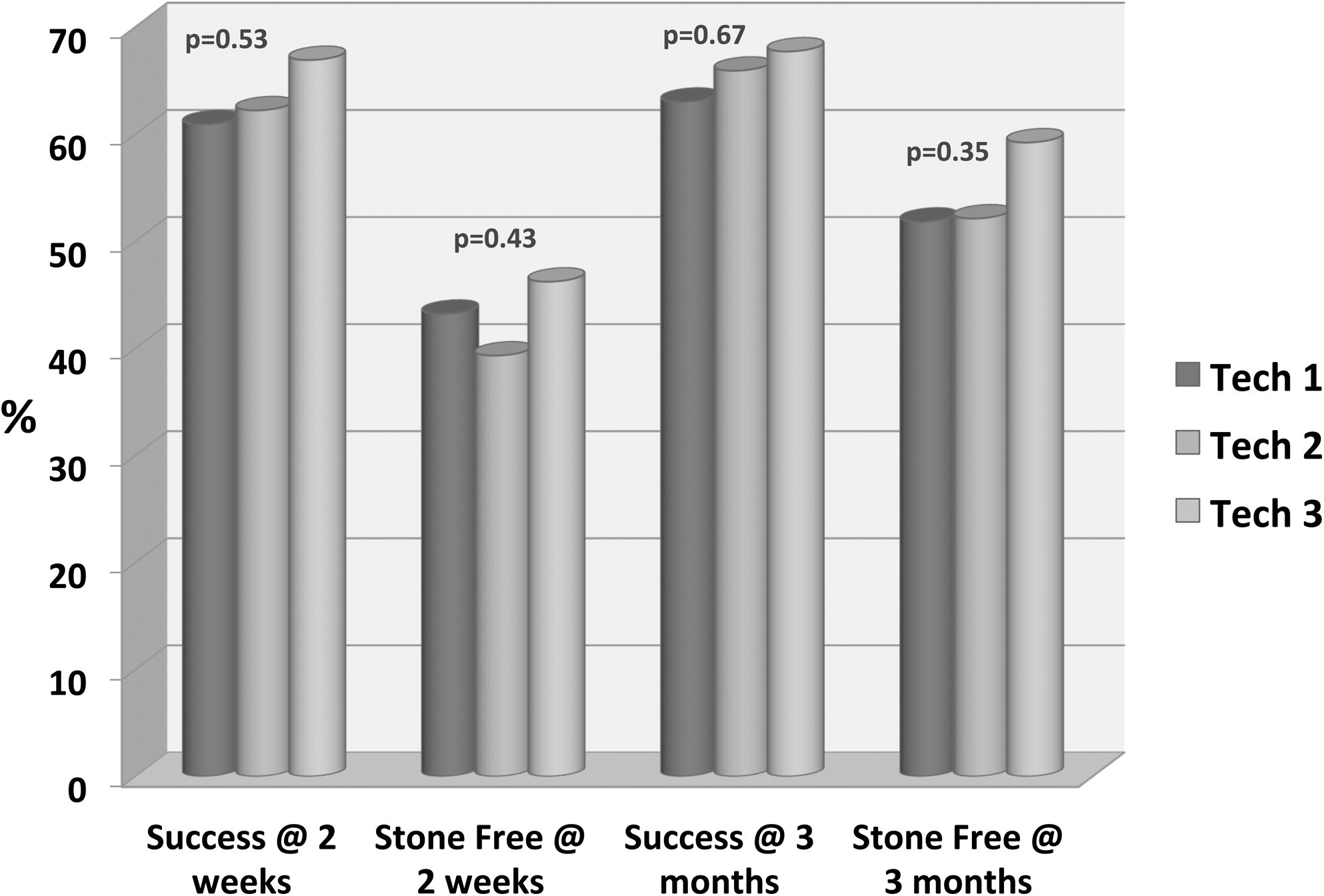
Comparison of successful fragmentation and stone-free rates across three radiologic technologists.
When examining fluoroscopy time, unadjusted analysis with the Student t test demonstrated that a significantly greater mean fluoroscopy time was used in treatments with successful fragmentation at 2 weeks (3.16 min vs 2.72 min, P=0.0001) and 3 months (3.12 min vs 2.75 min, P=0.0015) compared with treatment failures (Fig. 2). Likewise, fluoroscopy time differed significantly for stone-free rate at 2 weeks (3.16 min vs 2.88, P=0.028); however, no statistical difference was found at 3 months (3.08 vs 2.88, P=0.088) (Fig. 3).
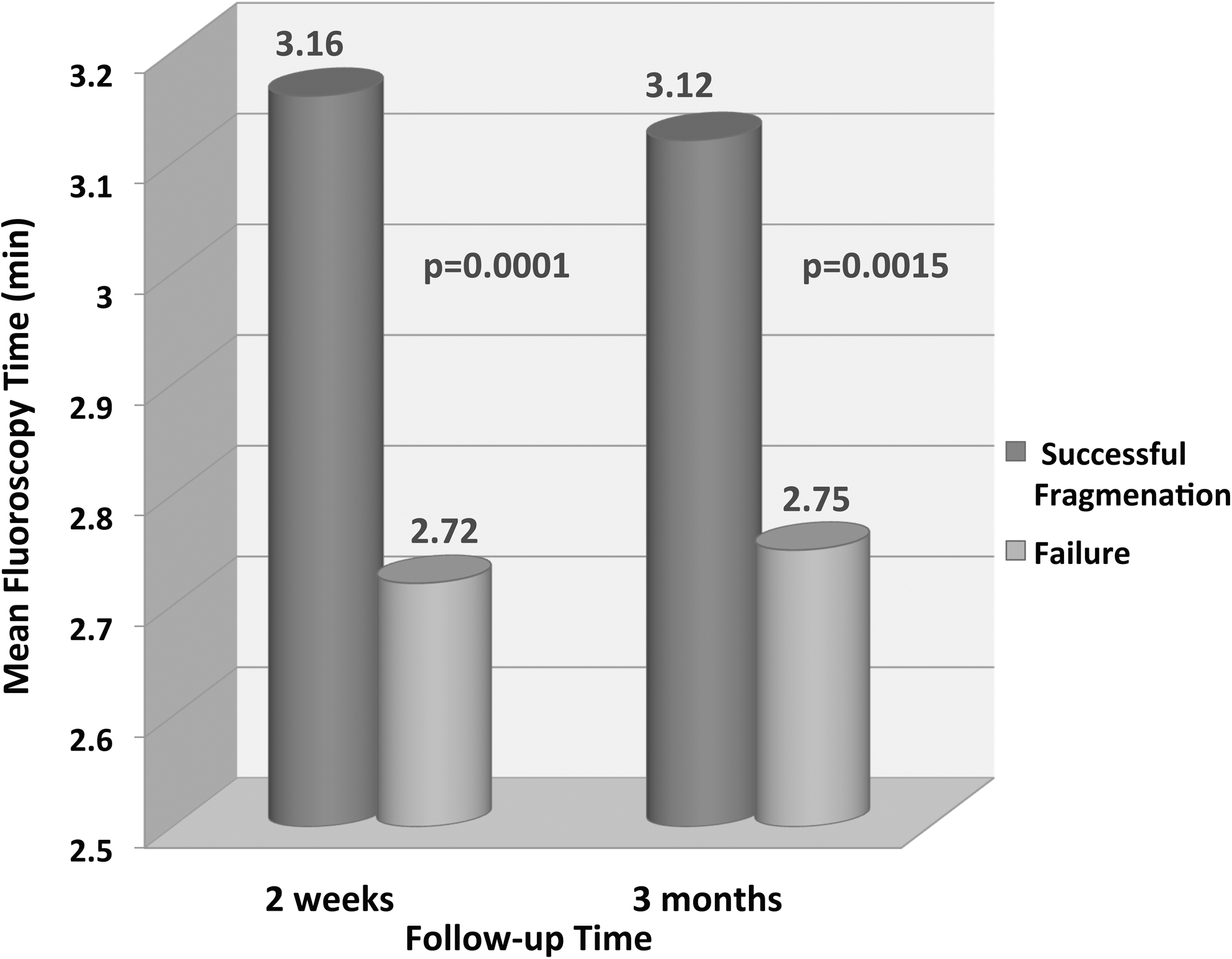
Comparison of fluoroscopy time based on successful fragmentation.
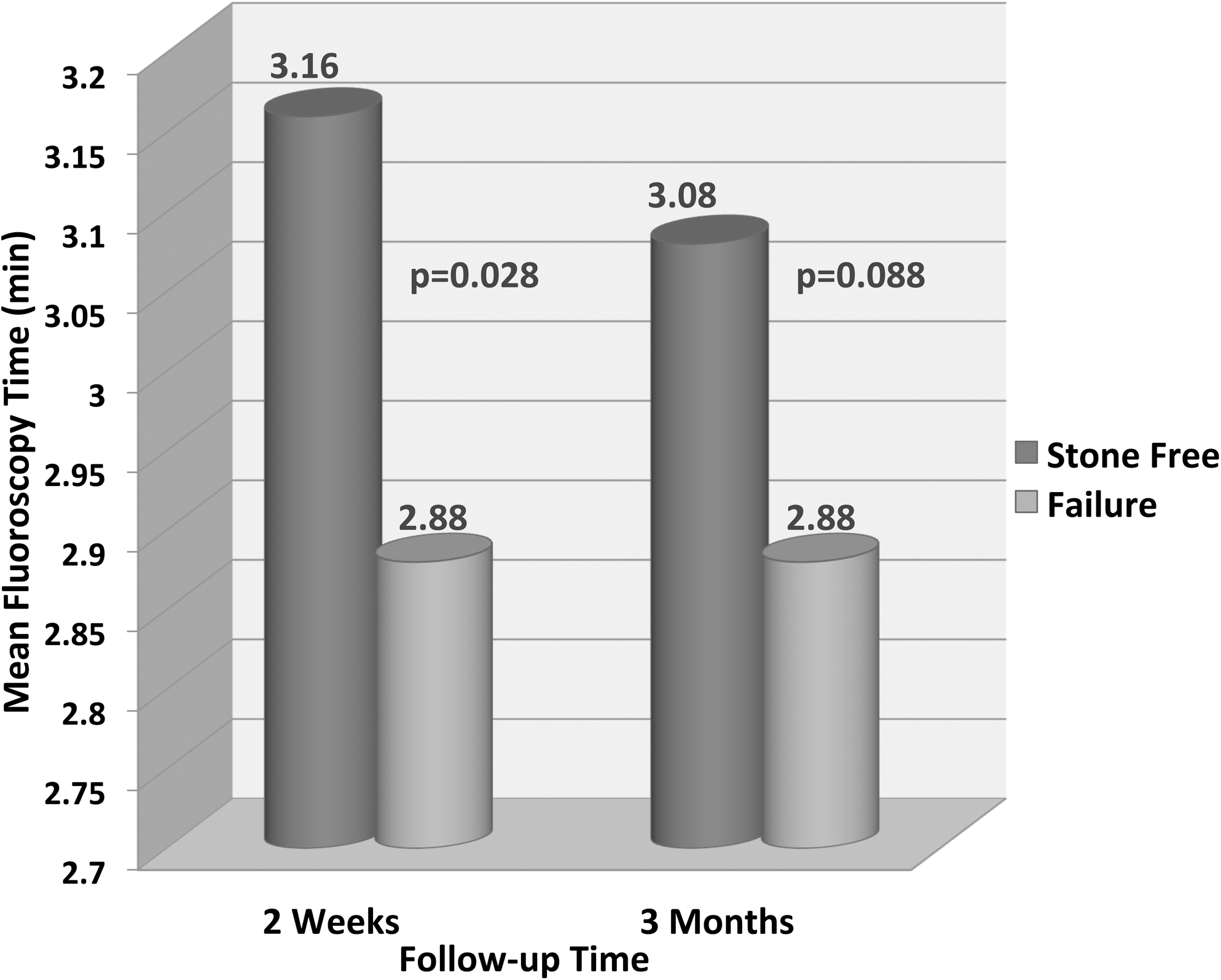
Comparison of fluoroscopy time based on post-treatment stone-free status.
Similarly, multivariable logistic regression analysis showed that fluoroscopy time remained a significant predictor of successful fragmentation at 3 months (odds ratio 1.3, 95% confidence interval 1.1, 1.5, P=0.0029) after adjusting for BMI, presence of a stent, and stone size and location.
Lastly, the mean radiation dose (dGy/cm2) between treatments with successful fragmentation vs failures at both 2 weeks and 3 months was not significantly different (Table 3). Equally, the mean radiation dose (dGy/cm2) between stone-free patients and failures at 2 weeks and 3 months was also not statistically significantly different (Table 3).
Discussion
Several stone parameters 3 –7 and patient demographics 3,6 –9 have been thoroughly evaluated for their ability to predict SWL outcomes in an attempt to determine which patients are most likely to have success after SWL therapy and as such, who is best treated with this modality. In our study we examined two operator characteristics, the radiologic technologist and fluoroscopy time to determine their impact on SWL treatment success. We chose to examine both stone-free rates and the rate of successful fragmentation. We think that the latter is an important outcome because it relates to the efficiency of fragmentation and is unaffected by the collecting system anatomy and the ability of the kidney to clear small stone fragments.
Our results did not demonstrate any statistically significant difference in either successful fragmentation or stone-free rates at 2 weeks and 3 months across our three radiologic technologists. This suggests the assisting radiologic technologist did not have a discernable effect on treatment outcomes at our center. Of note, however, at our institution, only three technologists are involved with SWL treatments, and all three have considerable experience with SWL. This may account for the relative equivalence across our radiologic technologists.
In a different institution where numerous technologists, many with limited experience, are involved with SWL treatments, the impact of the radiologic technologist would likely be quite different. In fact, a study by Lee and associates 11 demonstrated the impact of the radiologic technologist learning curve on the efficacy of SWL. In this study, as the technologists became more experienced, the stone-free rate improved. Thus, the generalizability of our findings is limited to institutions with experienced radiologic technologists. Nevertheless, our review does provide new information on the impact of experienced radiologic technologists on SWL treatment success. Repetition of our study in an institution with numerous radiologic technologists of varying levels of proficiency would be an informative next step.
Conversely, we found that mean fluoroscopy time was significantly different between treatments with successful fragmentation vs failure at both 2 weeks and 3 months, suggesting that using fluoroscopy to ensure accurate targeting during SWL is important for success. Notably, the observed difference in mean fluoroscopy time between treatments with successful fragmentation vs failure corresponded to a small, statistically nonsignificant difference in radiation dose between the treatment successes and failures. This is important, considering that patients who are not treated successfully with one SWL treatment will likely be exposed to more radiation moving forward from subsequent diagnostic and therapeutic imaging compared with those patients treated successfully. This would be primarily a result of more follow-up KUB radiography and CT scans, as well as further treatments with fluoroscopic guidance (ie, SWL, ureteroscopy or percutaneous nephrolithotomy) to manage their persistent stone disease.
Also of note, the lithotripter fluoroscopy uses a very coned-in image, which lowers the total body radiation exposure compared to KUB radiography and CT scans. Ultimately then, a small increase in fluoroscopy time during SWL treatment, without a significant increase in radiation exposure, can help to significantly increase treatment success and thereby potentially avoid a much greater exposure to radiation as a result of a failed treatment.
To our knowledge, the effect of fluoroscopy time on SWL treatment success has not been examined. A previous study from our center by Logarakis and colleagues 10 examined the variation in clinical outcome after SWL based on the treating urologist. As part of this retrospective review, we compared the mean fluoroscopy time used across 12 different treating urologists during SWL treatments. We found that the urologist with the greatest treatment success also had a significantly greater mean fluoroscopy time. This study certainly points toward a potential relationship between improved success rates and increased fluoroscopy time; however, potential important confounders of this relationship, such as the stone size and location, are not controlled for in our previous study. Also of importance, our previous study did not directly compare mean fluoroscopy time in treatment successes and failures.
In our present study, we directly compare mean fluoroscopy time across treatment successes and failures and perform multivariable logistic regression analysis to adjust for potential confounding by BMI, presence of a stent, and stone size and location on the relationship between fluoroscopy time and treatment success. Adjusted analysis demonstrated that fluoroscopy time remained a significant predictor of success, providing more definitive support for the relationship between fluoroscopy time and successful SWL fragmentation.
A limitation to our fluoroscopy time analysis, however, is that we have not adjusted for stone density. It is possible that more radiodense stones are easier to see and thus easier to target, necessitating less fluoroscopy time, but are conversely denser and thereby less likely to fragment. Future studies that assess the impact of fluoroscopy time on SWL treatment outcomes will need to account for the effect of stone density.
Conclusion
The radiologic technologist did not have a significant impact on SWL treatment outcome at 2 weeks and 3 months at our center. Successful fragmentation at 2 weeks and 3 months, however, was associated with a greater amount of fluoroscopy time. This suggests that using fluoroscopy to ensure accurate targeting during SWL is important for successful fragmentation.
Footnotes
Disclosure Statement
No competing financial interests exist.