
Abstract
Objectives:
To evaluate and compare perioperative outcomes of robotic partial nephrectomy (RPN) using robotic and laparoscopic ultrasound probe for tumor identification.
Materials and Methods:
Data from 75 consecutive RPN procedures using a laparoscopic ultrasound probe (January 2009- November 2010) and 75 consecutive RPN procedures using a robotic ultrasound probe (November 2010- November 2011) were collected. Perioperative outcomes of the two groups were retrospectively analyzed.
Results:
A total of 72 patients underwent 75 consecutive RPN using the laparoscopic ultrasound probe followed by 73 patients who underwent 75 consecutive RPNs using the robotic ultrasound probe. Characteristics were similar between groups, and tumors had a similar complexity (mean nephrometry score 6.6 vs. 6.8, p=0.534), mean operating room time (234 vs. 218 min, p=0.095), mean console time (173 vs. 156 min, p=0.071), mean blood loss (171 mL vs. 164 mL, p=0.79), and positive tumor margin rates (1.2% vs. 2.2%, p=1) did not achieve significance. All patients are free of cancer recurrence after a mean follow up of 25.7 months in the laparoscopic probe group and of 10.2 months in the robotic probe group.
Conclusions:
Robotic ultrasound probes for tumor identification during RPN had comparable perioperative outcomes and surgical margin rates as a laparoscopic ultrasound probe, but with the advantage of surgeon autonomy.
Introduction
Tumor identification during partial nephrectomy that is necessary for oncologic control can be facilitated by intraoperative ultrasonography. 9 –13 RPN using a laparoscopic ultrasound probe requires the probe to be controlled by the bedside assistant. A robotic ultrasound probe enables the surgeon, rather than the assistant, to control the probe. We evaluate our experience with RPN using a robotic ultrasound probe under surgeon control and compare the outcomes to RPN using a laparoscopic ultrasound probe.
Materials and Methods
RPN was performed using a laparoscopic ultrasound probe for tumor identification by an experienced robotic kidney surgeon in 75 consecutive surgeries in 72 patients between January 2010 and November 2010. From November 2010 till November 2011, we performed another set of 75 consecutive surgeries on 73 patients with the utilization of a robotic ultrasound probe.
Our RPN technique and subsequent modifications have been previously described. 6,14 After hilar dissection, kidney mobilization and opening of Gerota's fascia to expose the renal capsule in the region of the tumor intraoperative ultrasound was used for tumor identification and delineating of margins of resection. Regardless of the probe type used, the transducer was placed circumferentially along the edge of the tumor to identify the junction between tumor and normal parenchyma. The ultrasound images were displayed as a picture-on-picture image on the console screen using the TilePro feature 15 of the da Vinci surgical system (Intuitive Surgical, Sunnyvale, CA). The renal capsule was scored with cautery approximately a probe-width distance away from the tumor edge to provide an adequate margin of normal parenchyma. The renal hilum was then clamped (or in selected cases, left unclamped), and tumor excision was carried out along the scored line.
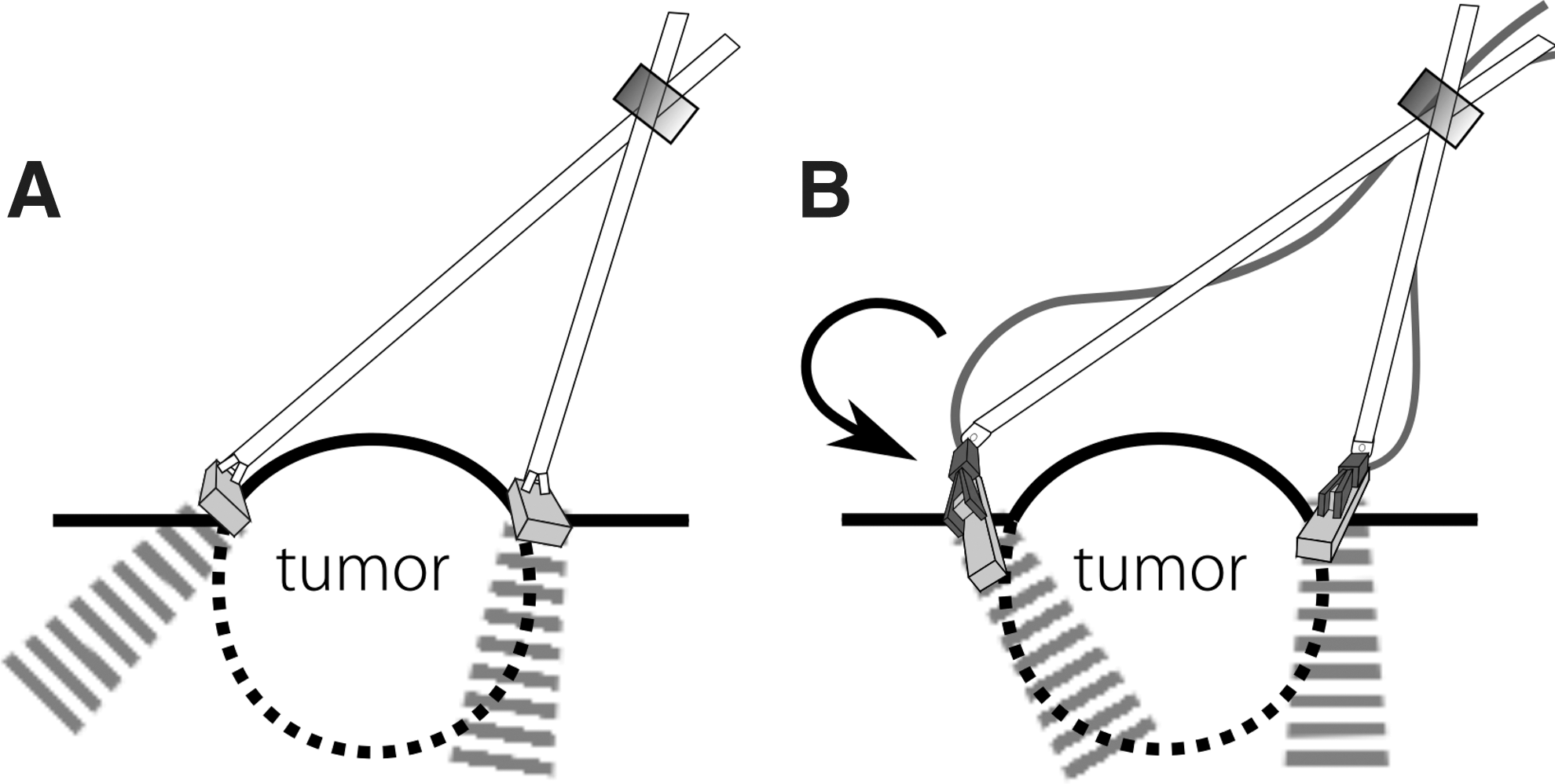
In the first group, we used a four-directional laparoscopic probe introduced through the assistant port, enabling four-directional movement of the probe by the bedside assistant (Fig. 1A). In the second group, an intraoperative ultrasound was performed with a robotic ultrasound probe. Technical characteristics of both probes are presented in Table 1. All RPN procedures were performed by an experienced surgeon and a bedside assistant with more than 100 cases of experience. The robotic probe was introduced through the primary assistant port, either by dropping it down a 12 mm trocar or by passing it with a microfrance grasper through a 15 mm trocar, which facilitates faster needles exchange, laparoscopic sponge deployment and enables specimen bag placement and tumor extraction. The probe consists of a transducer with a grooved ridge that fits the robotic grasping instrument and a flexible cable connecting the transducer to the externally located ultrasound console (Fig. 1B). The surgeon can grasp the notch on the back of the transducer, enabling the ultrasound to be controlled directly by the robotic surgeon.

Data received from manufacturer representative.
Patient demographics and perioperative outcomes from both groups were analyzed. Tumor characteristics as well as R.E.N.A.L. nephrometry scores were assessed based on preoperative CT images. Postoperative complications using the Clavien scale were recorded and evaluated. 16 Statistical significance of comparison between the samples was assessed via t-test and chi-square test for continuous and categorical values, respectively. Fisher exact test was used for variables with two categories. Analyses were performed by a statistician using SAS 9.2 for Windows (Carey, NC).
Results
There were 75 consecutive RPN procedures performed in 72 patients using the laparoscopic ultrasound probe, and 75 consecutive RPN procedures were performed in 73 patients using the robotic ultrasound probe. Three patients in the laparoscopic group and 2 patients in the robotic group underwent a second RPN procedure for contralateral tumors. The two patient groups had similar patient characteristics (Table 2). Both groups had similar tumor characteristics, including R.E.N.A.L. nephrometry scores (6.6 vs. 6.8), except the robotic probe group had a slightly higher endophytic component (42.8 vs. 55.3%, p=0.004). Perioperative outcomes are shown in Table 2. The robotic ultrasound probe group had similar outcomes to the laparoscopic probe, including operating time (234 vs. 218 min), mean console time (173 vs. 156 min), mean warm ischemia time (WIT) (19.4 vs. 19.0 min), mean estimated blood loss (171 vs. 164 mL), and positive surgical margins (1.2% vs. 2.2%). There was no statistically significant difference in measured variables between groups when controlling for tumor size and complexity in univariate or multivariate analysis. One patient with a positive margin in the laparoscopic probe group underwent a completion nephrectomy with final pathology negative for cancer.
Tumor nephrometry score of 11.
Number per tumor resected.
ARF requiring dialysis, delayed splenic bleed requiring exploration, pseudoaneurysm requiring embolization.
ICU admission for elevated blood pressure, splenic bleed requiring repair, pseudoaneurysm requiring embolization.
ASA=American Society of Anesthesiologists; BMI=body mass index; CCI=Charlson comorbidity index; RPN=robotic partial nephrectomy; WIT=warm ischemia time; EBL=estimated blood loss; eGFR=epidermal growth factor receptor; OR=operating room; LOS=length of stay.
Significant differences between the cohorts are highlighted in bold.
Functional outcomes noted by mean epidermal growth factor receptor (eGFR) preoperative results compared with the laparoscopic group were 75.3 versus 78.6 followed by mean eGFR at 1 month postoperatively 70.4 versus 72.3. After a mean follow up of 25.7 and 10.3, there was no evidence of radiographic recurrence.
Discussion
Intraoperative ultrasonography is useful during partial neprectomy for tumor identification to facilitate complete tumor removal. Gilbert et al. reported the use of intraoperative ultrasonography to identify renal cell carcinoma in patients with non-palpable tumors. 9 Assimos et al. reported the use of intraoperative ultrasonography in partial nephrectomy for the identification of tumor margins for deep intraparenchymal lesions. 10 Several other studies have described the use of intraoperative ultrasound during PN for tumor identification to help achieve negative margins and identify potential satellite lesions. 11 –13
The use of intraoperative ultrasonography has also found application in RPN, where the surgeon can take advantage of the ultrasound image superimposed as a picture-on-picture display on the console screen using the TilePro feature. 15,17 However, RPN using a laparoscopic ultrasound probe renders the surgeon dependent on the assistant to control the probe. The robotic ultrasound probe enables the precision of a robotic instrument as well as direct surgeon control. Yakoubi et al. described the use of the robotic ultrasound probe in laboratory conditions, reporting advantages of direct surgeon control and less instrument clashing in the external operative field. 18 Our group previously described the feasibility of RPN using a robotic ultrasound probe in 22 patients. 19 We now report our updated experience in 75 patients and compare outcomes with RPN patients in whom a laparoscopic probe was used. Our study demonstrated that the robotic ultrasound probe achieved comparable perioperative outcomes and surgical margins rates to RPN with a laparoscopic ultrasound probe but with the benefit of surgeon autonomy.
Both groups had tumors of similar complexity as defined by R.E.N.A.L. nephrometry scores, 20 although the robotic ultrasound group had a higher tumor endophytic percentage. Sun and colleagues reported that percent endophytic component is the single element of the nephrometry score system for which independent practicing urologists would recommend intraoperative ultrasound, 21 suggesting its unique importance. There was a trend toward a shorter mean console time in the robotic group by approximately 17 minutes (p=0.07). A larger study is warranted to further examine this trend.
Although adequate mobilization of the kidney can allow a laparoscopic ultrasound probe to achieve sufficient identification of tumors in challenging locations during RPN, this requires more dissection by the surgeon and less autonomy over probe control. Examples of challenging angles for a laparoscopic ultrasound include the far edges of the tumor, in which the probe and/or the kidney should be turned to place the probe flat on the kidney surface parallel to the tumor edge (Fig. 2). It can be especially challenging with tumors in a posterolateral or upper pole location. We had an experienced assistant for all cases. The surgeon independence offered by the robotic ultrasound probe could be more important when an experienced assistant is not available. However, we feel that a skilled bedside assistant is still important for other steps of the surgery. We found that the use of a 15 mm assistant trocar allows the robotic probe to be passed conveniently with a laparoscopic grasper. We have routinely utilized a 15 mm assistant port, as it facilitates faster needle exchanges, laparoscopic sponge placement, specimen bag deployment, and tumor extraction. However, a 15 mm trocar is not required to use the robotic probe, and those who prefer a 12 mm assistant port can have the robotic probe introduced in a drop-in fashion.
The robotic ultrasound probe lacks a hinging/articulation mechanism that is intrinsic to the laparoscopic probe, which may contribute to its lower cost. In the course of the study, we subjectively observed that the robotic probe resulted in less probe slippage and eliminated the need of probe grabbing for readjustment. This could make it less susceptible to mechanical issues with prolonged use. Future studies are needed to evaluate whether this would translate into financial savings. We did not do a formal cost analysis to assess whether it would be beneficial for centers already performing intraoperative ultrasound with a laparoscopic probe to purchase a robotic ultrasound probe. However, the majority of cost for an intraoperative ultrasound is for the ultrasound machine, not the probe. If centers doing RPN have already made the purchase of an ultrasound machine for an intraoperative ultrasound that is compatible with a robotic ultrasound probe, then the additional cost for a robotic ultrasound probe could be justified given the increased surgeon independence.
Conclusion
Use of a robotic ultrasound probe for tumor identification during RPN yielded comparable perioperative outcomes and surgical margin rates as RPN performed with a laparoscopic ultrasound probe, but with the advantage of surgeon control of probe movements and independence from the assistant.
Footnotes
Disclosure Statement
No competing financial interests exist.