
Abstract
Background and Purpose:
Port-site metastasis (PSM) is a rare complication of laparoscopic intervention in urologic malignancies. Of the greater than 50 reported cases of PSM in the urologic oncology literature, only 9 have occurred after surgery for renal-cell carcinoma (RCC). We report a 10th instance of RCC metastasis—in this case to the camera-port site after robot-assisted partial nephrectomy (RAPN). To our knowledge, this case is the first reported PSM of RCC after RAPN.
Patient and Methods:
A 68-year-old man underwent an uncomplicated right RAPN for a 4-cm right renal mass (stage T1aN0M0). Five months later, he was found to have metastatic disease with an isolated peritoneal recurrence at the camera-port site. Biopsy of the lesion confirmed RCC, and the lesion was surgically resected. A comprehensive MEDLINE search for all published studies of port-site recurrences after laparoscopic renal surgery for RCC was performed.
Results:
Nine cases of PSM after successful laparoscopic radical or partial nephrectomy for locally confined RCC have been reported. Proposed etiologic factors for port-site recurrence include biologic aggressiveness of the tumor, patient immunosuppression, local wound factors, and technique-related factors. We report an unusual case of PSM to a camera port that was not used for specimen manipulation or extraction.
Conclusion:
PSM after laparoscopic renal surgery for RCC is a rare occurrence. Our case, in which PSM occurred without specimen bag rupture or extraction through the port in question, highlights the importance of local and systemic factors in contributing to PSM occurrence. We also demonstrate that when PSM is the only site of disease recurrence, it can be successfully managed with minimally invasive surgical resection.
Introduction
PSM has been reported with multiple malignancies, most commonly in the gynecologic and surgical literature. 6 –8 The first known occurrence of PSM after a urologic procedure was in 1994, when Stolla and associates 9 reported a case of subcutaneous metastasis of bladder transitional-cell carcinoma (TCC) after laparoscopic pelvic lymph node dissection. Since then, more than 50 PSMs have been reported in the setting of urologic surgery. 10
PSM after laparoscopic extirpative surgery for renal-cell carcinoma (RCC) is extremely rare. An international review of 2604 cases by Micali and colleagues 8 in 2004 identified no instances of port-site recurrence. We performed a comprehensive MEDLINE search for published reports of PSM after laparoscopic nephrectomy or partial nephrectomy for RCC. In total, nine cases of PSM from RCC were identified. 11 –19
We report a 10th case of RCC metastasis to a port site, and the first known case to occur after robot-assisted partial nephrectomy (RAPN).
Patient and Methods
Case report
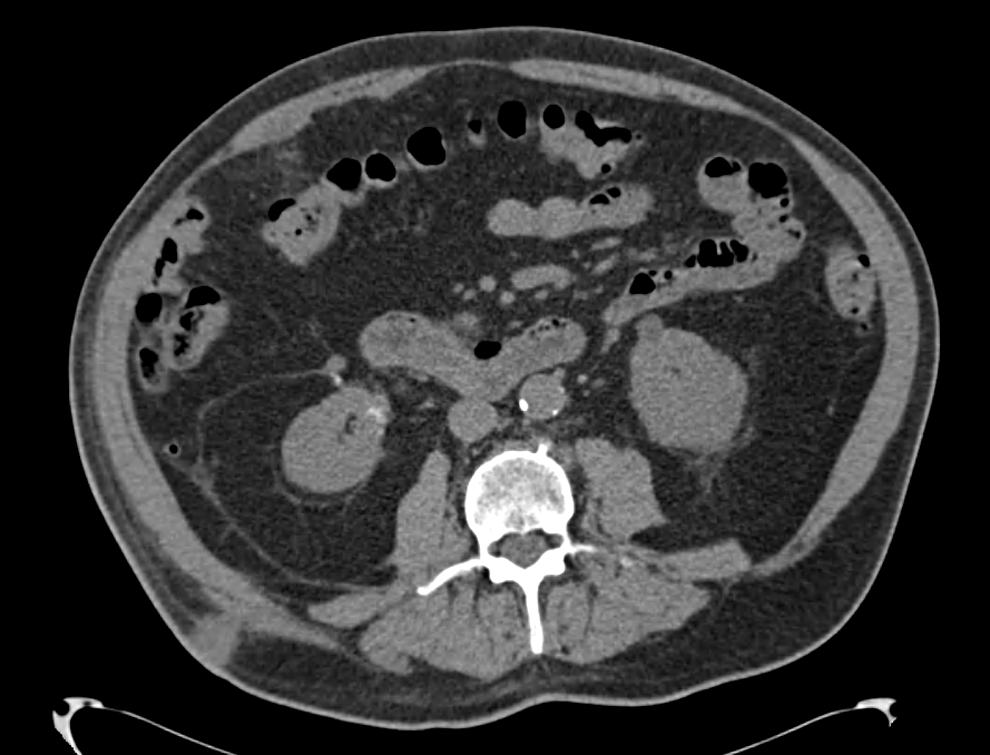
A 68-year-old man was incidentally discovered to have a 4-cm right renal mass (Fig. 1) with a nephrometry score of 10a. There was no radiographic evidence of lymph node involvement or distant metastasis. He successfully underwent RAPN in October 2011. During the resection, the mass was not obviously violated. The specimen was placed into an entrapment sack and extracted intact through the assistant port site. The extraction site was reapproximated at the fascia with an 0 polyglactin suture. The subcutaneous tissue at all sites was irrigated and the skin edges reapproximated with a stapling device. Pathologic examination revealed a 3.9 cm T1a clear-cell, Fuhrman grade 3/4 RCC with negative margins results (Fig. 2). Five months later, in March 2012, routine follow-up CT revealed a 1.7 cm mass located on the abdominal wall (Fig. 3) at the camera port site used during the initial resection. Of note, this site was not used for specimen extraction. The patient was otherwise free of disease recurrence and completely asymptomatic. Ultrasound-guided biopsy of the abdominal wall mass showed metastatic RCC that stained strongly for RCC-immunoperoxidase (Fig. 4). In the absence of other metastatic disease, the patient was scheduled for resection of the PSM.

Preoperative CT demonstrating an incidental 4-cm right renal mass.
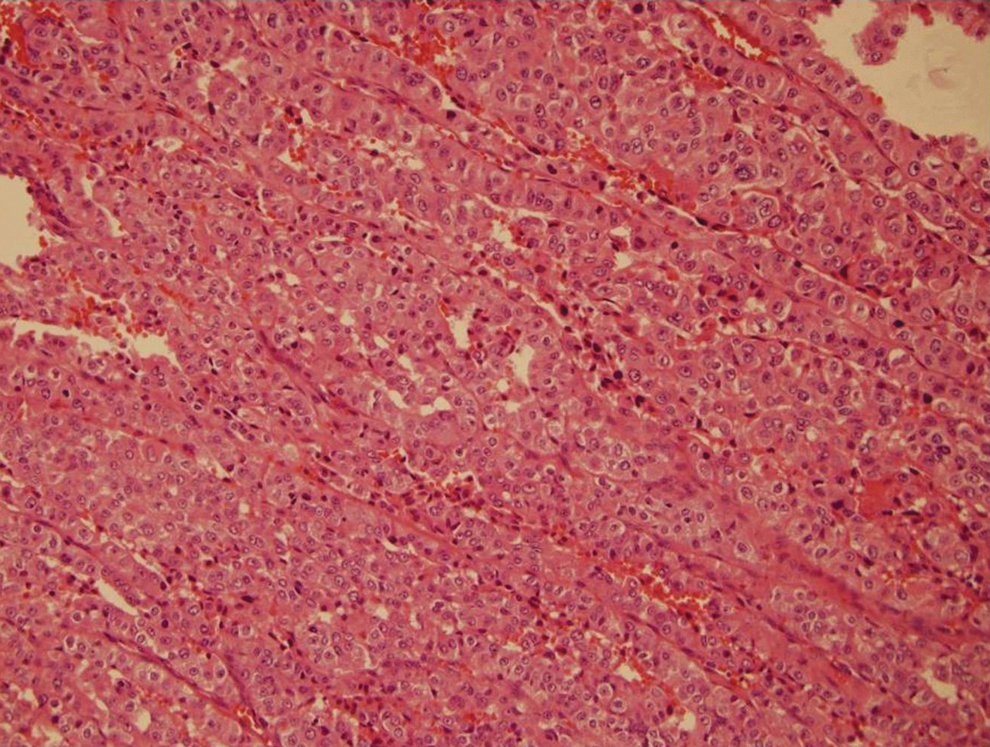
Surgical pathology section of the right kidney showed clear-cell tumor cells with Fuhrman grade 3.
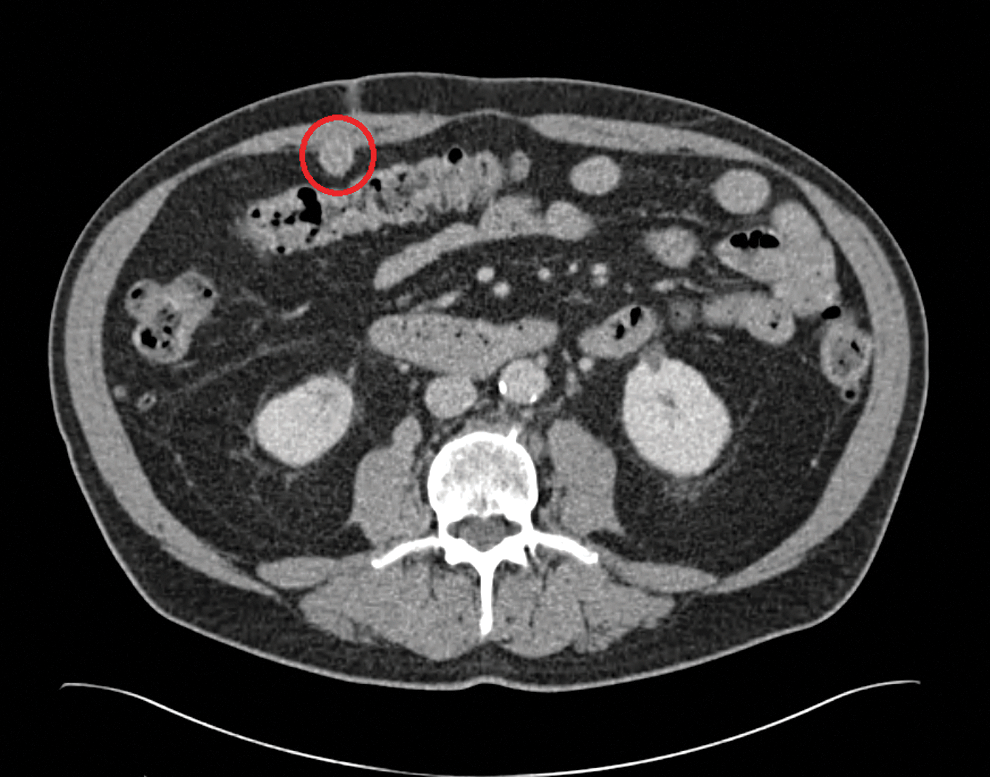
Routine follow-up CT 5 months after robot-assisted partial nephrectomy for renal-cell carcinoma revealed a 1.7 cm mass located on the anterior abdominal wall at the previous camera-port site.
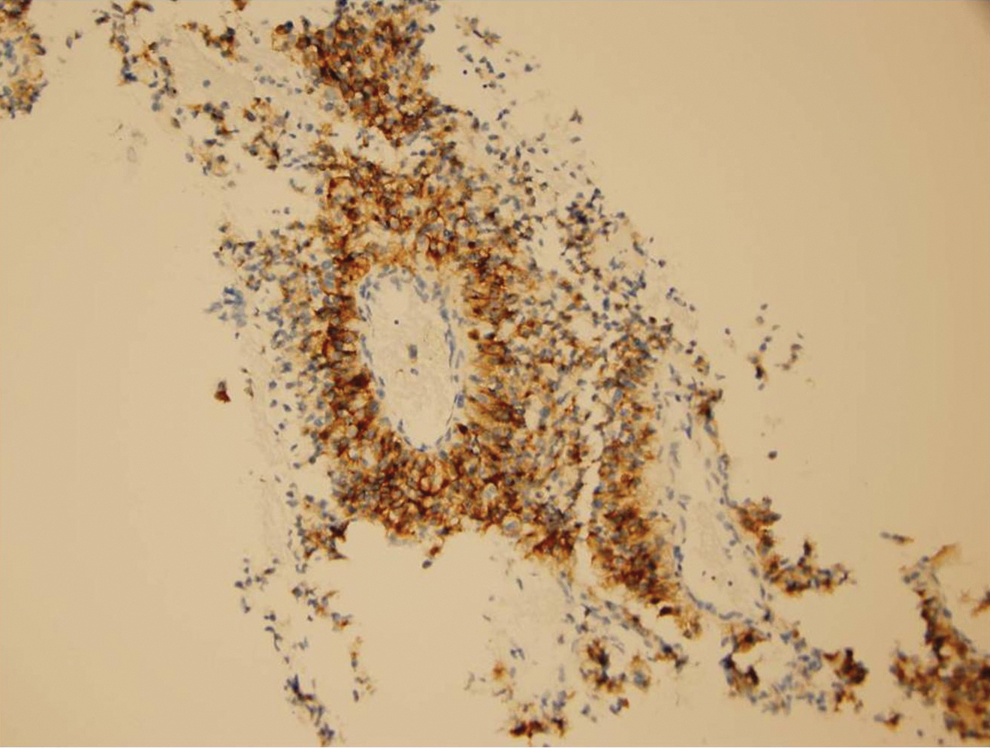
Biopsy sample of the port-site mass stained strongly for renal-cell carcinoma-immunoperoxidase.
With the patient in the left lateral decubitus position using a retroperitoneal approach, the peritoneum was entered after the retroperitoneal space was developed. The mass was well visualized (Fig. 5A) and was circumferentially excised with wide margins (Fig. 5B). The mass was then placed in an entrapment sack. The posterior rectus fascia was closed with 2-0 polyglactin suture, which was reinforced with Weck Hem-o-lok clips (Teleflex, Research Triangle Park, NC). Hemostasis was ensured after the insufflation pressure was decreased to 5 mm Hg, the specimen was extracted, and the port sites were closed. Blood loss was minimal, and the patient was discharged home on postoperative day one. Pathologic examination of the PSM demonstrated a 3.4-cm granular variant clear-cell RCC with negative margins results. A follow-up CT scan 3 months later did not reveal new metastatic disease or locally recurrent disease in the kidney or at the camera-port site (Fig. 6).
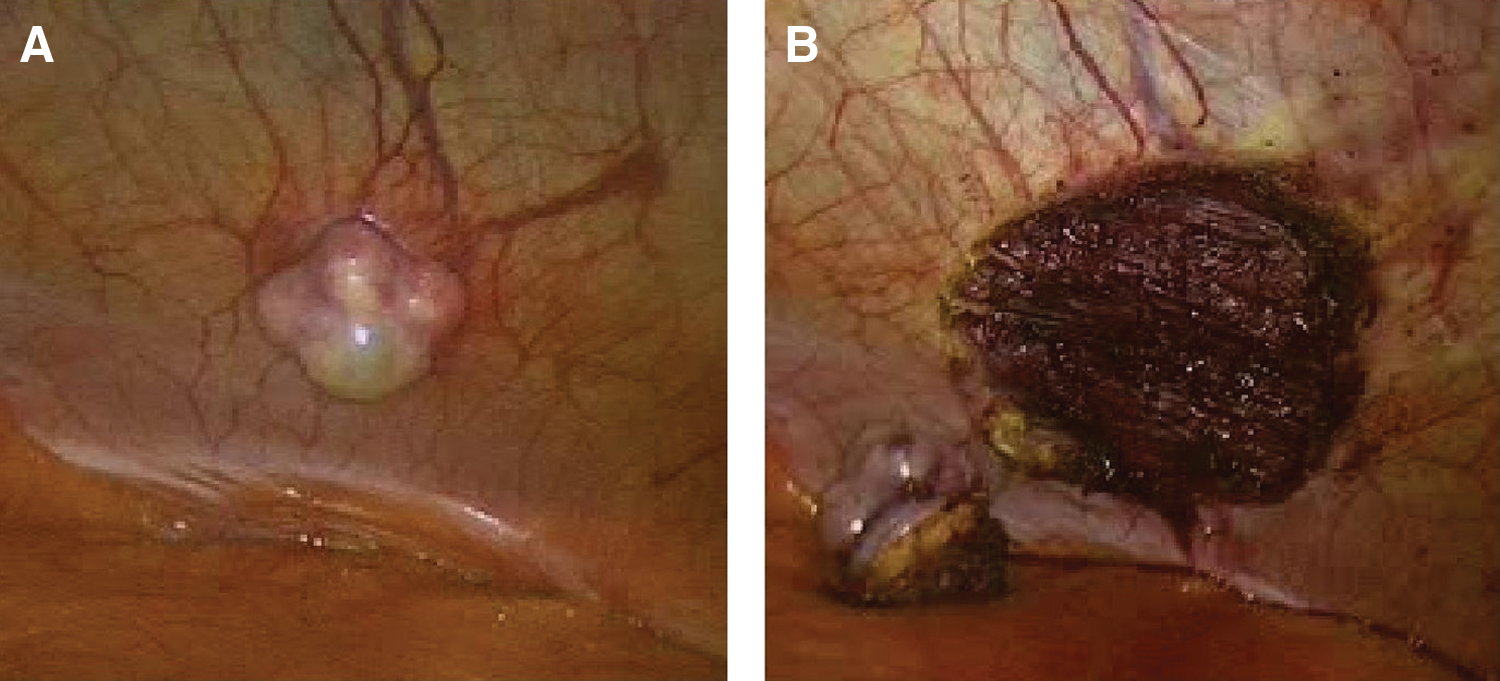
The abdominal wall mass before and after resection.
Follow-up CT scan 3 months after resection of the port-site mass demonstrated no disease recurrence.
Discussion
The risk of loco-regional disease dissemination and recurrence after laparoscopic surgery for abdominal and pelvic malignancies is well documented in the gynecologic and surgical oncology literature, with an incidence ranging up to 5% for gynecologic malignancies and 4% for colorectal cancer. In one report, port-site metastasis developed in 70 (17.1%) of 409 patients with incidental gallbladder cancers discovered during laparoscopic cholecystectomy, 70% of which occurred in the port used for extraction of the specimen.
Laparoscopy been applied extensively to manage malignancies in urology and, in recent years, several reports of PSM and tumor seeding have been published in the urologic literature. The reported incidence of port-site seeding in the literature is variable, because some studies suggest an incidence as high as 21%. 20 Most authors agree, however, that the rate of port-site seeding is rare (<1%), 21 and some report that these rates are similar to rates of wound seeding noted in open procedures. 2 Indeed, an international survey of 19 urologic laparoscopic centers performing a total of 18,750 laparoscopic procedures for urologic malignancies found tumor seeding in 13 cases (0.1%). 8 Furthermore, the majority of port-site recurrences reported in this survey represented TCC, including four cases of incidental TCC after simple nephrectomy and three cases of TCC after nephroureterectomy for suspected TCC. The remaining six cases included four laparoscopic adrenalectomies for lung cancer metastasis and one case each of laparoscopic pelvic lymphadenectomy for penile squamous cancer and retroperitoneal lymph node dissection for nonseminomatous germ-cell testicular cancer. 8 Of note, this review by Micali and coworkers 8 identified no instances of port-site recurrence in 2604 cases of laparoscopic radical nephrectomy (LRN) for RCC.
Very few cases of port-site recurrences after laparoscopic extirpative surgery for RCC have been reported. After the first report of a solitary port-site recurrence by Fentie and associates 11 in 2000, there have been only eight additional reports of port-site tumor recurrence after laparoscopic radical or partial nephrectomy (Table 1). We report a 10th case in which tumor metastasis at a robotic port site developed 5 months after uncomplicated RAPN for localized RCC.
For port-site tumor recurrence to occur, several conditions must be present. There must be release of viable cancer cells from the tumor. There must be a mechanism by which these tumor cells are transported to the port site. Last, implantation of the tumor cells at the port site and subsequent growth must occur. It has been hypothesized that several factors may aid in this process, namely (1) the biologic aggressiveness of the tumor, (2) local wound factors, (3) host immune responses, and (4) laparoscopic surgical techniques. 4
Tumor aggressiveness as defined by stage and Fuhrman grade may have a significant impact on port site and overall incidence of tumor recurrence. 22 –24 Of note, three of the nine previously reported cases of PSM after laparoscopic radical or partial nephrectomy for RCC were associated with locally advanced, stage T2 or higher tumors. Moreover, all cases of port-site recurrence after laparoscopic extirpative surgery for RCC that are described in the literature have been associated with intermediate to high-grade tumors (Fuhrman grade 2 or greater). Indeed, the first of these cases occurred in association with a tumor displaying Fuhrman grade 4 histopathology with sarcomatoid elements. The case we present represents a port-site recurrence of an early-stage (T1N0M0), high-grade (Fuhrman grade 3) tumor, reminiscent of the case reported by Castillo and colleagues. 17
Local wound factors may aid the implantation and proliferation of tumor cells at a port site. It has been demonstrated that cancer cells have high proliferation potential within healing skin incisions or intestinal anastomosis. 25 Tumor cells may implant more successfully during early wound healing, adhering to fibrin deposited at the site of surgical trauma as a part of normal healing. 26 Furthermore, the presence of growth factors at the wound site may promote the survival and propagation of these cancer cells. Perhaps the port-site incision is more conducive than the laparotomy incision for tumor seeding, as some animal studies and anecdotal experience seem to imply. 27 In light of these risks, repair of the peritoneum at the trocar entry site may reduce the risk of tumor implantation and subsequent recurrence. 28
Depressed immune function may also contribute to tumor recurrence and metastasis. Overall immune function is diminished in the perioperative period because of several mediating factors, including anesthetic agents, opioids, surgical trauma, blood transfusions, temperature changes, pain, and psychological stress. 29 In animal models, surgical trauma has been shown to reduce natural killer cell activity and promote tumor metastasis. 29,30 Furthermore, Chueh and coworkers 31 reported a case of PSM after bilateral hand-assisted laparoscopic nephroureterectomy for TCC in a renal transplant patient, underscoring the role of immunosuppression in the development of PSM. Similarly, Yildrim and colleagues 32 reported an unusual case of port metastasis in a renal transplant patient who underwent uneventful laparoscopic cholecystectomy for benign gallbladder disease and subsequently received a diagnosis of adenocarcinoma of the colon with isolated colon cancer metastasis at the cholecystectomy port site. The physical distance between the surgical site and the unsuspected colon tumor, which the authors note had not been manipulated at the time of cholecystectomy, only serves to emphasize the role of host immunity in the development of PSM.
Interestingly, three of the previously reported cases of PSM after laparoscopic extirpative surgery for RCC occurred in patients who had compromised immune function because of other medical conditions. One patient had chronic renal failure and one had alcoholic cirrhosis, both associated with compromised immune function. 33,34 A third patient had diabetes mellitus, a condition also resulting in depressed immunity. In the case presented here, the patient also had a history of diabetes mellitus for 15 years and was currently receiving a two-drug regimen.
Several factors related to laparoscopic surgical technique have been implicated in contributing to port-site recurrence after LRN. These include the use of pneumoperitoneum, trocar site contamination, organ and tumor morcellation, and the method of specimen retrieval.
There is debate in the literature as to whether gas insufflation/desufflation during laparoscopy has an effect on the dissemination of tumor cells. Several studies have suggested that CO2 insufflation does have an impact on the movement of tumor cells within the peritoneal cavity and subsequent implantation at port sites. 35,36 Jones and coworkers 37 noted a three-fold incidence in PSM in a hamster model of tumor cell suspension when pneumoperitoneum was compared with the results of the laparotomy only group. Wittich and associates 38 found that aerosolization of tumor cells does occur during CO2 laparoscopy, but that the number of intraperitoneal tumor cells needed for metastases to occur by this mechanism is extremely high. To address this, others have suggested that gas leakage around the port sites leads to a “chimney effect.” 39 Per the chimney effect hypothesis, the continued leakage of gas around and through the trocar results in a cumulative buildup of tumor cells at the port site, thus promoting PSM. Tseng and coworkers 40 demonstrated that tissue trauma at trocar sites, combined with leakage of CO2, led to enhanced tumor growth at these sites. Nevertheless, studies by Hubens and colleagues 41 failed to confirm these findings, and the role of the chimney effect remains unclear.
Another hypothesis posits that CO2 itself stimulates tumor growth either through a direct effect on tumor cells or by interfering with local defense mechanisms. Jacobi and associates 42 compared the effect of CO2 and helium on colon adenocarcinoma growth after 30 minutes of pneumoperitoneum. Abdominal wound tumors developed in a significantly greater number of animals in the CO2 group when compared with the helium and anesthesia control groups. In another study, Jacobi and coworkers 43 demonstrated that subcutaneous tumor growth is stimulated by CO2 independent of intraperitoneal pressure. Kuntz and colleagues 44 suggested that because lower pH has a recognized negative impact on local defense mechanisms, this could explain the higher incidence of PSM during laparoscopy with CO2 compared with other gases. The hypothesis that CO2 stimulates tumor growth, however, was refuted in a study by Tsivian and associates 45 that showed that CO2 pneumoperitoneum does not increase the invasive potential of tumor cells. Others have also found that CO2 pneumoperitoneum is not essential for the development for PSM. 22,23 Further studies to define the role of CO2 insufflation in port-site recurrences are needed.
In addition to the potential effects of pneumoperitoneum on the transfer of tumor cells, it has also been proposed that malignant cells may be transferred from the tumor to the port site by the aggressive manipulation of the tumor with laparoscopic instruments and the subsequent withdrawal and reinsertion of these contaminated instruments. Hewett and associates 46 were the first to demonstrate this concept in a pig model. In his study, Hewett determined that malignant cells were rarely found in CO2 exhaust (1/30 port filters), but were more readily cultured from port washings (2/10 ports) and instrument washings (4/10 laparoscopic instruments). Other studies corroborate this finding and conclude that the exfoliation of tumor cells secondary to aggressive surgical manipulation increases the risk of port site tumor seeding, while the risk of port site recurrence decreases with increased laparoscopic experience. 47 –9 The importance of minimizing tumor manipulation is underscored by Greco and colleagues' 18 PSM case in which specimen rupture occurred during laparoscopic partial nephrectomy. Irrigating port sites with povidone-iodine at the completion of the case may lower the risk of port-site recurrence. 50 Local application of cytotoxic agents, such methotrexate and cyclophosphamide, has also been shown to be effective. 51,52
It is our practice to perform intact specimen extraction within an entrapment bag in all cases of suspected renal malignancy. The case of port-site recurrence reported by Iwamura and coworkers 13 occurred in a setting in which an entrapment bag was not used, and the free specimen was removed through an unprotected incision, perhaps contributing to the risk of PSM. The case of RCC metastasis at the hand port (used for specimen extraction) after hand-assisted LRN reported by Chen and colleagues 15 provides an additional example of PSM when an entrapment bag was not used. The use of an entrapment sack for specimen retrieval to minimize port-site contamination has now been widely adopted.
Another method for extraction is specimen morcellation, which leads to a more cosmetically appealing result than the usual 7-cm incision necessary for intact specimen removal and is performed at many centers. While some long-term studies have shown specimen morcellation to be oncologically safe, 52,53 the role of morcellation in the pathogenesis of PSM remains controversial. A study by Urban and coworkers 54 found that intact entrapment sacks were impermeable to tumor cells and even to bacteria. Of the 24 sacks tested, however, 4 had pinhole perforations when morcellation of pig kidneys was performed. Moreover, morcellation was performed in three of the nine previously reported cases of RCC PSM the role of specimen morcellation in the development of port-site recurrence in these three cases can certainly not be excluded. In fact, Castilho and colleagues 12 attributed their case of PSM to microperforations in the entrapment bag during morcellation and have since modified their technique to open extraction. Of note, Castilho and associates 12 performed their specimen morcellation in a plastic bag, which others have shown to be particularly vulnerable to perforation. When used, specimen morcellation should be performed with great care in an impermeable, nylon-reinforced entrapment bag and under direct vision to minimize the risk of tissue spillage and subsequent wound contamination.
The factors that contribute to PSM likely also play a role in postsurgical peritoneal carcinomatosis. Unlike PSM, intra-abdominal metastasis of RCC can occur as a first presentation of RCC, outside of the setting of surgical manipulation. 55 Peritoneal carcinomatosis, however, has also been noted in the setting of partial nephrectomy. In 2008, Masterson and Russo 19 reported two cases of peritoneal carcinomatosis, one that occurred 2 years after hand-assisted partial nephrectomy for RCC and another that occurred after laparoscopic cryoablation for RCC. Ultimately, both patients in these cases received extensive surgical resection. Although they did not have details from the original surgery, the authors noted that the pathology sample in the first case was fragmented, suggestive of an intraoperative tumor violation. While surgical factors could certainly play a major role in peritoneal carcinomatosis, biologic factors should not be understated. Adrenocortical carcinomas, for instance, have very high rates of peritoneal carcinomatosis (83%) after laparoscopic resection, despite adherence to oncologic principles. 56
Indeed, the importance of biologic factors likely plays a very large role in PSM. Highshaw and associates, 57 for example, reported on a case in which a patient underwent LRN for RCC, followed by resection of a sacral chordoma 6 weeks later. Although the two surgeries had different sites of dissection and were completely discontinuous, the patient was later found to have a sacral chordoma metastasis to one of the laparoscopic ports used for LRN. Similarly, while it is unclear the exact cause of PSM in our case, our experience underscores the importance of factors outside of surgeon control. In our case, the tumor was not violated, surgical margins had negative results, an entrapment bag was used, and the specimen was removed intact. The occurrence of a PSM at the camera-port site despite these precautions highlights the other factors that contribute to PSM. Aerosolization caused by pneumoperitoneum, escaping air causing a chimney effect, and/or seeding of tumor into liquid suspension could all have contributed to transport of microscopic amounts of tumor to the camera port. There, tumor cells were able to take root despite irrigation of the wounds, perhaps because of a combination of global and local factors. Ultimately, however, we were able to manage the isolated PSM in this instance with a minimally invasive approach.
Conclusion
The incidence of port-site recurrence after LRN is rare, and its etiology is likely multifactorial. Several measures can be taken to minimize the risk of PSM: (1) Rigorous adherence to oncologic surgical techniques with minimal handling of the tumor, (2) trocar fixation and avoidance of gas leakage along the trocar tract, (3) intact extraction or morcellation within an impermeable bag under direct vision, and (4) povidine-iodine irrigation of the laparoscopic instruments and port-site wounds when appropriate. Although improper technique involving specimen manipulation and extraction has been implicated in the etiology of PSM, the current occurrence of PSM at the camera-port site underscores the importance of tumor and wound-related factors, host immunity, and other technical considerations in the etiology of PSM.
Footnotes
Disclosure Statement
No competing financial interests exist.