
Abstract
Purpose:
The aim of the present study was to investigate the learning curve and perioperative outcomes in 200 consecutive patients with prostate cancer who underwent robot-assisted radical prostatectomy (RARP).
Patients and Methods:
Between August 2006 and August 2011, 200 patients with prostate cancer underwent RARP and were enrolled in this study. We prospectively collected the demographic data and analyzed the pathologic and functional outcomes. The operative outcomes analyzed were total operative time, estimated blood loss (EBL), positive surgical margin (PSM), incontinence, and perioperative complications. We also evaluated the relationship between the surgeon's experience and operative variables.
Results:
The sloping learning curve for this surgeon showed that total operative time was strongly correlated with the accumulation of experience for the initial 25 cases (|rs|=0.71, P<0.001). The average EBL was not strongly correlated with additional experience (|rs|<0.7). The PSM rate for the first 50 cases was significantly higher than that of the next 150 cases (34.8% vs 19.4%, P=0.035). The complication rate among the first 50 patients was significantly higher than that among the remaining 150 patients (32% vs 12.7%, P=0.002). The incontinence rate at 12 months was significantly higher for the first 100 cases compared with that for the next 100 cases (9.0% vs 1.0%, P=0.009). For the surgeon to optimize total operative time, PSM rate, complication rate, and incontinence rate, slope learning curves of 25, 50, 50, and 100 cases were needed.
Conclusions:
The functional and pathologic results of this minimally invasive procedure seemed to be promising. Distinct learning curves were observed with respect to operative time, PSM, complication rate, and incontinence rate. Exposure to 100 surgeries would be necessary for a surgeon to adequately master the required skills.
Introduction
Robot-assisted radical prostatectomy (RARP) is now typically performed using the da Vinci surgical system (Intuitive Surgical, Sunnyvale, CA) as one of the standard procedures for the treatment of patients with prostate cancer and has dramatically changed the landscape of conventional LRP. Because this technique does not need the urologist to overcome a steep and long learning curve, more than 85% of prostatectomies in the United States were performed using RARP in 2009. 9 RARP provides the urologist with superior three-dimensional vision and substantial freedom of movement. This device transmits the surgeon's movements smoothly by compensating for any hand tremors. RARP also boasts ergonomics that are far superior to those of LRP. 10
In Japan, however, RARP is still in the introductory phase; to our knowledge, no previous study has described the perioperative outcomes of RARP in a large number of patients. This study was designed to evaluate the utility of robot-assisted surgery. In this article, we present intraoperative data and pathologic and functional outcomes associated with the initial 200 cases of RARP performed by a single surgeon. The ethics committee at Tokyo Medical University approved this study.
Patients and Methods
Between August 2006 and August 2011, a total of 352 patients with localized prostate cancer underwent RARP. The surgeries were performed by seven surgeons at Tokyo Medical University Hospital. Among the patients, 200 underwent the procedure by a single surgeon (KY), who had considerable expertise in open RP (approximately 500 surgeries performed) but no experience in laparoscopic surgery. During the study period, he performed 10 robot-assisted radical cystectomies after performing more than 60 RARPs. In the initial 100 cases, the surgeon was assisted by a fellow as patient-side assistant; these cases were included in the study. We prospectively collected the associated perioperative data: Demographics and perioperative outcomes, including pathologic and functional results.
The surgeon in this study had not performed a conventional laparoscopic surgery before performing his first RARP, although he had extensive experience with open radical prostatectomy (ORP). In March 2006, the surgeon participated in a 2-day training course under the guidance of Prof. Vipul R. Patel at the department of urology, Ohio State University. The surgeon's first RARP was performed in August 2006. As we have previously reported, Prof. Patel mentored the surgeon during his 10th and 11th RARP surgeries.
The operations were performed as previously described by Patel and associates 11 with minor modifications. In brief, the bladder neck preserving procedure was attempted for all cases using two different approaches: Anterior or lateral. We introduced the lateral approach from tcase #38. The posterior rhabdosphincter reconstruction technique was performed just before vesicourethral anastomosis, 2 which was initiated in case #28. Positive surgical margins (PSM) were defined as the presence of cancer tissue on the inked surface of the specimen. Postoperative continence was defined as no use or the use of only one safety pad. We evaluated postoperative urinary continence based on the patients' responses to the interview we conducted at each follow-up clinic visit.
Data analysis
The operative outcomes analyzed were total operative time, estimated blood loss (EBL), pathologic results, and perioperative complications. We also evaluated a learning curve for total operative time, EBL, PSM rate, incontinence rate, and complication rate. Thirty patients who were treated with neoadjuvant hormone therapy before undergoing RARP were excluded from the PSM analysis. Potency was not evaluated in this study because only a limited number of patients replied to the International Index of Erectile Function questionnaire.
We plotted a sloping learning curve by referring to previous reports. 6,12,13 Namely, outcomes were grouped according to number of procedures performed by the surgeon into eight chronologic groups. Among these 200 patients, the results of the first 25 cases were compared with those of the remaining 175 cases, the first 50 with the remaining 150, the first 75 with the remaining 125, and so on. To evaluate the effect of the surgeon's experience on dichotomous outcomes, chi-square tests were used to assess the statistical trend of the differences between the groups evaluated. P values<0.05 were considered statistically significant. The effect of the surgeon's experience on total operative time and EBL was assessed using the Spearman rank-order correlation coefficient. We also calculated the absolute value of the correlation coefficient (|rs|). |rs| values were determined for each chronologic group. |rs|≥0.7 and P values<0.05 were considered strongly correlated with surgeon volume. Once |rs|≥0.7 and P values<0.05 were obtained, we performed additional analysis to compare between groups using the Mann-Whitney U test. All statistical analyses were performed using STATA (ver. 11.0; StataCorp, College Station, TX).
Results
Patient demographics are shown in Table 1. There was no significant association between the surgeon's experience and any other variable (age, serum prostate-specific antigen [PSA] level, clinical T stage, prostate volume, biopsy Gleason score, D’ Amico's risk classification, pathologic T stage, pathologic Gleason score, or the frequency of nerve-sparing procedures). The median follow-up period was 35 (range, 23–80) months.
SD=standard deviation; PSA=prostate-specific antigen.
The operative and postoperative data are shown in Table 2. The nerve-sparing procedure was performed in 96 (48.0%) patients, including 82 unilateral and 14 bilateral cases.
SD=standard deviation.
PSM was found in 40 (23.5%) of 170 patients. The PSM rates were 9.8% for pT2 and 54.2% for pT3. A total of 36 complications, with no cases of mortality, were seen in 30 patients. No intraoperative complication was observed. The postoperative complications observed are shown in Table 3. Eight (4.0%) patients temporarily needed prolonged use of a urethral catheter (for 3–7 additional days) because of acute urinary retention. Urinary leakage from the anastomosis was seen in five patients; the problem resolved with extended catheter placement (1–2 weeks).
The total operative time, EBL, PSM rate, incontinence rate, and complication rate of the first 50, second 50, third 50, and last 50 cases are shown in Table 4. The average total operative time was 190 minutes (range, 129–413 min). As graphically depicted in Figure 1, the sloping learning curve for this surgeon showed that total operative time was strongly correlated with the accumulation of experience for the initial 25 cases (|rs|=0.71, P<0.001). Total operative time, however, was not strongly correlated with the surgeon's experience over the next 175 cases (Fig. 1). Total operative time of the initial 25 cases was significantly longer than that of next 175 cases groups (P<0.01). The average EBL was 250 mL (range, 0–1000 mL), and EBL was not correlated with the accumulation of experience for the initial 25 cases (|rs|=0.2809, P=0.1737, Fig. 2). EBL of the initial 25 cases was not significantly different from that of the next 175 cases groups (P>0.05).
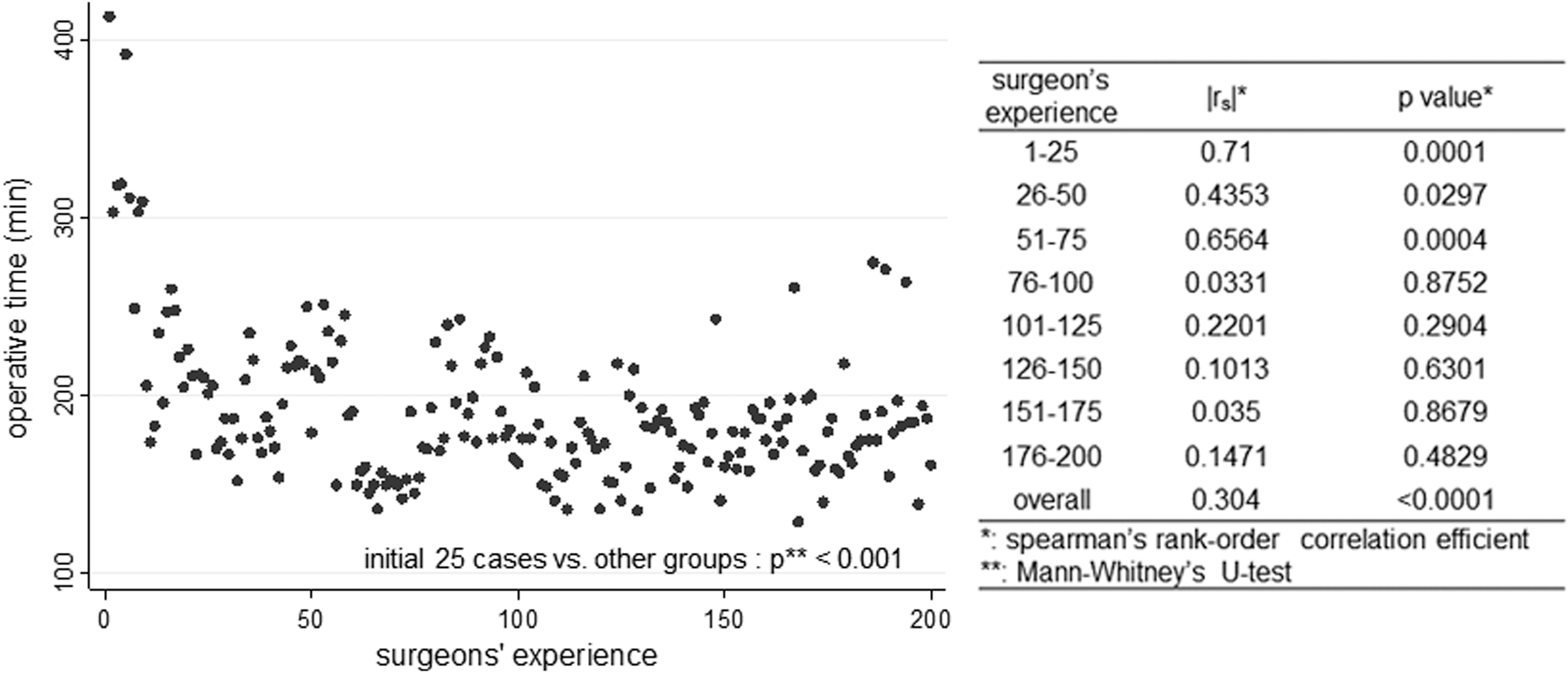
Total operative time inversely correlated with surgeons' experience in the initial 25 cases.
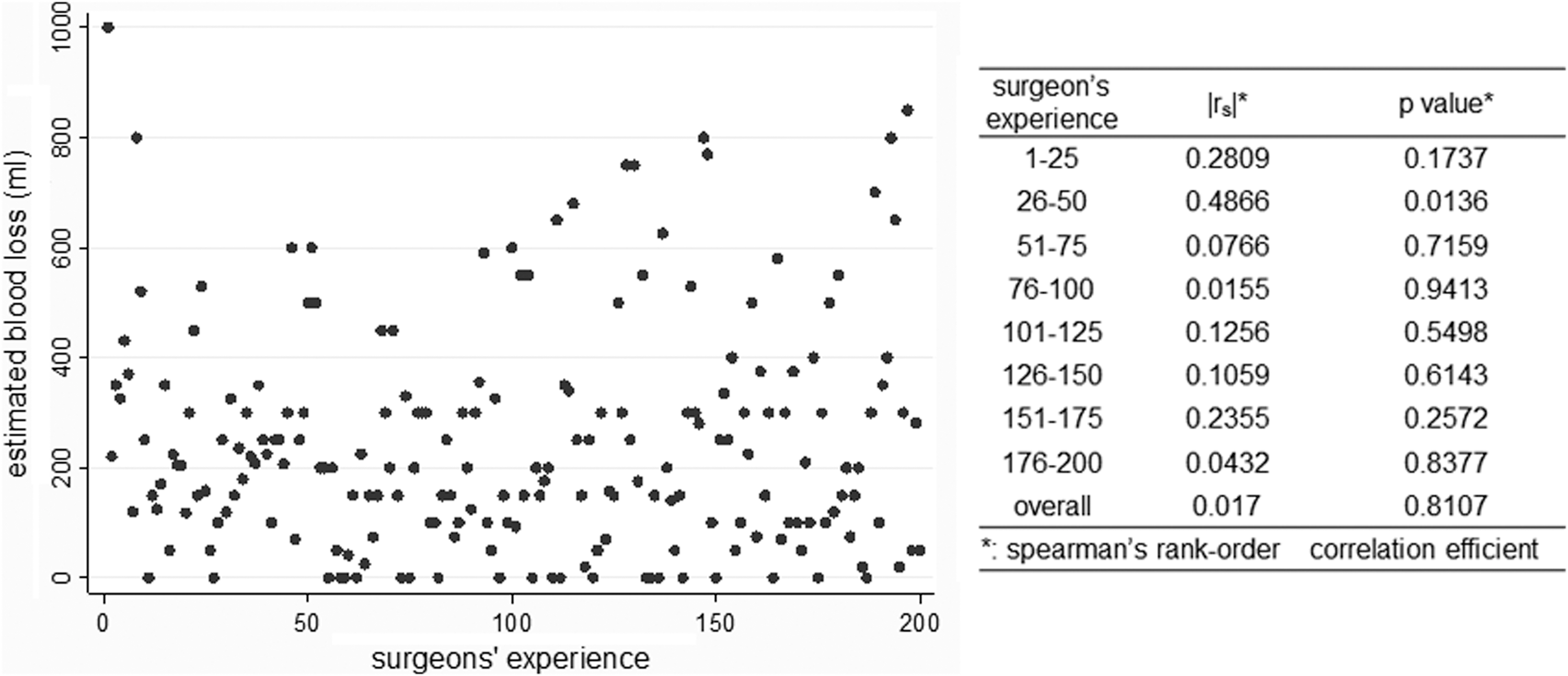
Estimated blood loss did not decrease with surgeons' experience.
EBL=estimate blood loss; SD=standard deviation; PSM=positive surgical margin.
The PSM rate for the first 50 cases was significantly higher than that of the next 150 cases (34.8% vs 19.4%, P=0.035). Although the PSM rate of the first 50 cases with pathologically organ-confined disease was not correlated with the surgeon's experience (12.5% vs 8.9%, P=0.321), the PSM rate of the first 50 cases with pathologically extracapsular extension disease was significantly correlated with the surgeon's experience (81.8% vs 48.6%, P=0.029). The complication rate was also correlated with the surgeon's experience.
The complication rate among the first 50 patients was significantly higher than that among the remaining 150 patients (32% vs 12.7%, P=0.002). Among these 200 patients, 129 (64.5%), 176 (88.0%), and 192 (96.0%) patients achieved continence at 3, 6, and 12 months, respectively. The incontinence rates at 3, 6, and 12 months are shown in Table 4. The incontinence rate at 3 months was significantly higher for the first 50 cases compared with the next 150 cases (50.0% vs 30.7%, P=0.006). The incontinence rate at 6 months was significantly higher for the first 100 cases compared with that for the next 100 cases (19.6% vs 5.0%, P=0.002). Similarly, the incontinence rate at 12 months was significantly higher for the first 100 cases compared with that for the next 100 cases (9.0% vs 1.0%, P=0.009). The skills necessary to achieve an acceptable total operative time, PSM rate, complication rate, and incontinence rate had slope learning curves of 25, 50, 50, and 100 cases, respectively (Table 5).
|rs|: spearman's rank-order correlation efficient.
Discussion
To our knowledge, the present report is the first to document favorable pathologic and functional RARP outcomes in Japan. We demonstrated that RARP is indeed suitable even for Japanese patients, who tend to have pelvises that are anatomically narrower compared with those of American and European patients. We also document an approach that accelerated the learning curve with equivalent perioperative outcomes compared with previous reports on conventional LRP. 14
Over the last decade, RARP has emerged as the main alternative to ORP, especially in the United States. 11,15,16 Complicated laparoscopic procedures are simplified by robot assistance, which reduces the number of cases necessary for surgeons to hone their skill set. This approach may also provide more favorable oncologic and functional results compared with conventional LRP and ORP. 15,17 In Japan, RARP has generated significant interest among urologists. In this report, we have shown that the learning curve for total operative time, pathologic PSM rate, and postoperative continence rate were stabilized by the 25th to 100th cases, even if a surgeon did not have any experiences with LRP, as previously demonstrated. 18,19
Despite these favorable results, robot-assisted surgery is still in an introductory phase in Asia, especially in Japan. This is because the advantages, in terms of perioperative outcomes, might still be insufficient to warrant the higher costs of robot-assisted surgery. Therefore, confirmed surgical benefits will be necessary to validate the performance of RARPs in Japan.
We introduced RARP in 2006. In 2008, we reported the perioperative outcomes of our initial 24 RARP cases. 20 Over the last 2 years, RARP has become a routine surgical procedure for patients with prostate cancer at our institution. Indeed, RARP accounted for 95% of all RPs in our institution. Here we evaluated our recent 4-year experience of RARP and confirmed its feasible perioperative utility.
Several studies in other countries have reported a learning curve for initial RARP experiences. In initial cases, EBL and operative time ranged from 145 to 570 mL and 202 to 498 minutes, respectively; these values improved to 75 to 500 mL and 130 to 195 minutes, respectively, when the surgeon had performed the procedure in 100 to 300 cases. 8,11,13,21 These parameters were similar to those used in this report.
In terms of pathologic PSM, overall PSM rate as previously reported from several high-volume centers with 250 or more cases ranges from 9.3% to 33.3%. The PSM rate among pT2 and pT3 cases ranges from 5.4% to 13.0% and from 31.9% to 45.0%, respectively. 3 Our overall PSM rate was 23.5% and 9.8% for the pT2 stage, values that are comparable with contemporary LRP and RARP series.3,8,22 –25 In our series, the overall PSM rate for the first 50 cases was 34.8%, which was significantly higher than that observed for the next 150 cases (19.4%).
Several modifications to RARP surgical techniques have been described in an effort to reduce the PSM rate. 26 As we reported in our previous series, 27 the dorsal venous complex (DVC) was ligated initially; however, after case 70, the DVC was first incised without ligation. Thereafter, the DVC was ligated with a running suture. Complete dissection of the apex and posterior aspect of the prostate and a complete nerve-sparing procedure might have been accomplished with an increased knowledge of the fascial anatomy. Experience of performing RARP in a large number of patients would improve the technical expertise of the surgeons and help achieve a good PSM rate. Of note here, the proportion of patients with intermediate- or high-risk disease is considerably higher (70.5%) in this study than in series from high-volume centers in North America. 28 Notably, these findings may be because of demographic differences and the way they manifest during PSA screening.
As for postoperative functional results, Tewari and colleagues 29 compared ORP and RARP. In their study, the RARP group achieved adequate continence earlier than the ORP group (84% and 98% at 12 months postoperatively. In our study, the continence rate among the first 100 cases was slightly low; however, for the next 100 cases, values were similar to those presented in previous reports (Table 4). As described previously, the surgical techniques were improved with increased experience. We reported that some of these techniques significantly improved the recovery rates of continence. 2
The lateral approach to bladder neck preservation, bladder neck reconstruction, anterior reconstruction, and Rocco double-layered posterior reconstruction were significantly associated with early recovery of urinary continence in univariate analysis. In particular, the Rocco double-layered posterior reconstruction was specifically important. The continence rate was improved possibly because of the increased experience associated with the enhancement of these techniques.
Zorn and coworkers 21 reported that complication rate was not correlated with the number of surgeries performed by the surgeon. Nevertheless, he reported that all four open conversions in that series occurred in the first 25 cases. The previously reported complication rate ranged from 1.0% to 41.7%. The overall complication rate in our study was 17.5%, which was similar to that in other studies.
This study had certain limitations. First, it was a retrospective analysis of data collected from patients who were treated with RARP by only one surgeon who was a first-generation robotic surgeon in the country; hence, our results might not be applicable to other RARP series. Considering that the learning curve for RARP may differ according to surgeons or institutions, a study involving several surgeons is needed. Second, the assessment of continence (including no validated questionnaires and open interviews) has not yet been standardized; thus, a different data collection method could yield different results. Nevertheless, this study provides important insights into the learning curve of RARP in Japan.
Experience of performing the procedure in a considerable number of cases is essential to achieve expertise in RARP technique; however, gaining experience in prostatectomy is difficult for each single surgeon because of the relatively low morbidity rate of prostate cancer in Japan. From the present report, however, we believe this clinical disadvantage can be overcome by making every effort of self-practicing in a training surgery system and show acceptable results of RARP. We believe that the results in the present study may encourage many urologists who have just initiated robot-assisted surgeries. We continue to investigate the positive features of RARP in Japan.
Conclusions
We conclude that the pathologic and functional results of RARP seem to be promising. In this study, total operative time, PSM, complication rate, and incontinence rate were related to distinct learning curves. The skills necessary to achieve an acceptable total operative time, PSM rate, complication rate, and incontinence rate had sloping learning curves of 25, 50, 50, and 100 cases, respectively. Exposure to 100 surgeries would be necessary for a surgeon to adequately master the required skills.
Disclosure Statement
No competing financial interests exist.