
Abstract
Treatment of patients with staghorn calculi with percutaneous nephrolithotomy can be challenging, often necessitating multiple tracts or sessions for complete stone clearance. Although open anatrophic nephrolithotomy can result in higher stone-free rates, it is rarely performed because of increased morbidity. To provide a minimally invasive alternative, we developed the technique of robot-assisted anatrophic nephrolithotomy (RANL) incorporating ice slush for renal hypothermia. Three patients with staghorn calculi (mean total stone volume 12887.67 mm3) underwent RANL with iced cold ischemia. A GelPOINT™ port was used for ice slush insertion. Intracorporeal temperatures were <9°C within 30 minutes of cold ischemia. Mean console and cold ischemia times were 167 and 56.7 minutes, respectively. Mean blood loss was 100 mL. There were no complications. Two patients had residual fragments measuring 13 mm, and two 9 mm stones, respectively. RANL with iced cold ischemia is a safe and feasible option that may be considered in patients with staghorn stones. Further study is needed to refine the technique and assess long-term functional outcomes.
Introduction
Percutaneous nephrolithotomy (PCNL) remains the treatment standard for patients with staghorn calculi. 1 Recent studies have revealed stone-free rates after PCNL for staghorn calculi to be between 47% and 57%. 2,3 Currently, open stone surgery is an alternative in situations when a staghorn calculus is not expected to be removable by a reasonable number of PCNLs and/or ancillary procedures. 1 Such stones may be dealt with by open anatrophic nephrolithotomy (ANL) with ice slush renal hypothermia. 4 Although laparoscopic ANL has been described by several groups, 5 –7 these procedures have been performed under warm ischemia. Removal of complex stones may necessitate a longer ischemic time and, in particular, cold ischemia would be renoprotective. 8 Furthermore, a robotic technique may offer greater precision for reconstruction while instrumentation such as robotic ultrasound or bulldog clamps can also be used.
We recently described a technique for renal hypothermia (intracorporeal cooling and extraction [ICE]) during robot-assisted partial nephrectomy (RPN). 9 We now present our technique of robot-assisted ANL (RANL) using ice slush cold ischemia for treating patients with staghorn calculi. This series represents the early experience between two robotic urologic teams operating at a single tertiary referral stone center. A video demonstrating the technique accompanies this article (see footnote).
Technique
1. Imaging: All patients underwent plain abdominal radiography and CT with three-dimensional (3D) reconstruction for stone volume assessment (Fig. 1).
2. Inclusion criteria: Patients with type 2 or 3 staghorn calculus using previously established criteria. 10
3. Exclusion criteria: Solitary kidney, bleeding diathesis, and age <18 years.
4. Cystoscopy: A ureteral stent was placed immediately before the robotic procedure.
5. Patient position: Standard flank position with 30-degree tilt. All pressure points were padded and protected. Upper and lower body warmers were used to maintain core temperature.
6. Port placement: A GelPOINT™ device was used for delivery of ice saline slush and stone removal. The GelPOINT was inserted through a 3 to 4 cm incision at the paramedian line. After establishing pneumoperitoneum, the 12-mm camera port and 8-mm assistant port were placed through the GelPOINT (Fig. 2). Under direct vision, two 8-mm robotic ports were placed along with a 12-mm assistant port using the Airseal™ for insufflation.
7. Docking: The robot is docked over the ipsilateral shoulder at a 30-degree angle from the patient's spine.
8. Kidney dissection: A 0-degree camera lens was used throughout. A fenestrated bipolar grasper was used in the nondominant hand and monopolar hook in the dominant hand. The bowel was mobilized to expose the renal pedicle. The renal vessels were encircled with vessel loops to facilitate clamping after ice slush delivery. The kidney was completely mobilized within the Gerota fascia.
9. Robotic ultrasonography: A robotic ultrasound probe was used to locate renal calculi and assess overlying parenchyma. The line of incision(s) was marked with cautery, either on atrophic parenchyma overlying the stone, or if parenchyma was normal, on the Brodel line immediately posterior to the convexity of the kidney.
10. Ice slush delivery: Ice slush was inserted through the GelPOINT using modified syringes as described previously. 9 Ice slush was loaded into multiple modified syringes 5 minutes before clamping in preparation for rapid delivery. Ice was placed directly onto the kidney surface while in one patient, ice was placed within a modified laparoscopic bag placed over the kidney with the string cinched and clipped at the hilum. Before inducing renal ischemia, 12.5 g of mannitol was infused. The renal artery was clamped with robotic bulldogs followed by the renal vein to maintain core temperature and visualization (Fig. 3). Repeated injections of ice slush were performed to cover the entire kidney surface. Renal parenchymal and core body temperatures were measured using thermal probes placed in the kidney and esophagus, respectively (Fig. 3).
11. Nephrolithotomy: After ice delivery, the premarked portion of the renal capsule was incised with the monopolar hook. Ice was reapplied as needed while on clamp. The hook was exchanged for a Prograsp™ to help grasp stones. For larger stones, a fenestrated double bipolar was also used (Fig. 4).
12. Stone retrieval: Stones were either placed in a retrieval bag or extracted immediately through the GelPOINT (Fig. 4). Smaller stones were removed using the 10-mm sucker. After inspecting all calices robotically, robotic ultrasonography was redeployed to assess stone clearance.
13. Renorrhaphy: A sliding-clip technique was used for renorrhaphy with a robotic needle-driver in the dominant hand. 3-0 poliglecaprone was used for suturing the inner layer of the collecting system, while a running barbed suture (2-0 V-Loc™) was used for the outer layer. Hemostatic agents were applied to the closure.
14. Drainage: Excess slush was removed with suction. A drain was brought through the lower 8-mm robotic port site. The ureteral stent was removed 3 weeks later.

Preoperative three-dimensional CT demonstrating left-sided type 2 staghorn calculus.
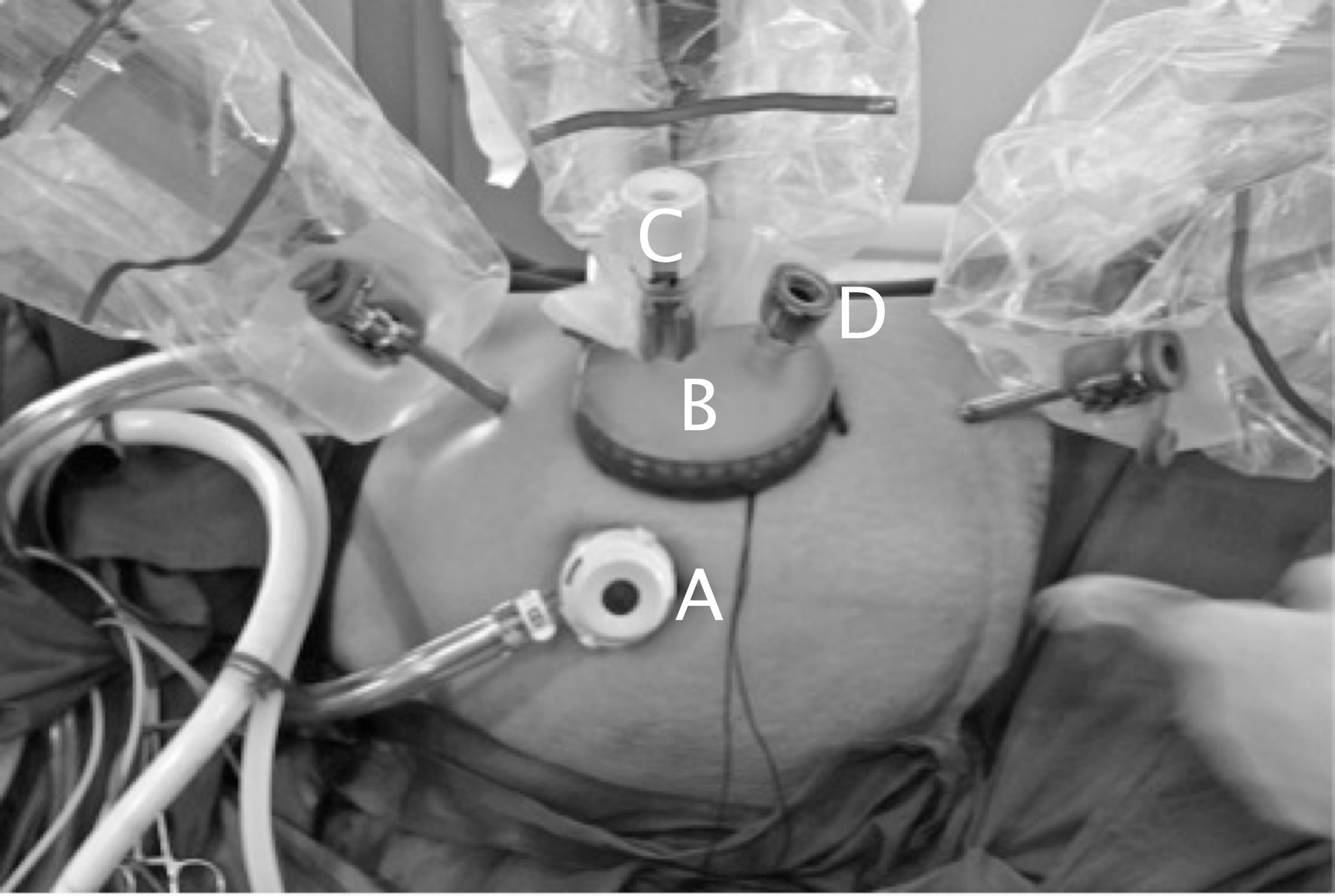
Patient position and port placement for left-sided robot-assisted anatrophic nephrolithotomy demonstrating:

Robot-assisted anatrophic nephrolithotomy

Nephrolithotomy being performed using Prograsp™ in left hand and double fenestrated grasper in right hand.
Equipment
• da Vinci® Surgical System, Si (Intuitive Surgical Inc., Sunnyvale, CA)
• Fenestrated bipolar (Maryland) forceps, hook, large needle driver, double fenestrated forceps (Intuitive Surgical Inc., Sunnyvale, CA)
• GelPOINT™ Advanced Access Platform (Applied Medical Inc., Rancho Santa Margarita, CA)
• Applied Medical Kii: CTF73 - 12 mm port×1 (Applied Medical Inc., Rancho Santa Margarita, CA)
• Laparoscopic suction 10 mm (Sklar Instruments Inc., West Chester, PA)
• Nadiad laparoscopic bag 11
• ProART™ robotic ultrasound transducer 8826 (BK Medical, Peabody, MA)
• Reliance robotic bulldog clamp (Scanlan International, Saint Paul, MN)
• Airseal® insufflation system and 12-mm port (SurgiQuest Inc., Milford, CT)
• Mon-a-therm™ temperature probe 400TM (Covidien, Mansfield, MA)
• 2-0 V-Loc™ barbed suture (Covidien Inc., New Haven, CT)
• 3-0 Monocryl SH needle; 0 Vicryl CT-1 needle (Ethicon Inc., Cincinnati, OH)
• Hem-o-lok clip (Teleflex Medical Inc., Research Triangle Park, NC)
• Lapra-Ty clips (Ethicon Endo-Surgery Inc., Cincinnati, OH)
• Hemostatic agents: Floseal (Baxter Inc., Deerfield, IL); Tisseel (Baxter Inc., Deerfield, IL); Surgicel SNoW™ (Ethicon Inc., Cincinnati, OH)
Role in Urologic Practice
Results
RANL was achieved in all cases with successful introduction of ice slush and stone extraction under cold ischemia. Table 1 provides demographic, perioperative, and postoperative data on patients who underwent RANL. Renal intracorporeal temperatures of <15°C were achieved within 8 minutes of cold ischemia, and there was no drop in core body temperature over 0.5°C during any procedure. Intracorporeal temperatures were <9°C within 30 minutes of cold ischemia (Fig. 3). Two patients were known intraoperatively to have incomplete stone clearance. A Malecot drain was placed in one of these patients after pyonephrosis was discovered after removal of calculi from an interpolar calix. There were no intraoperative or postoperative complications. No patient needed a blood transfusion or developed sepsis. Plain abdominal radiography on postoperative day 2 confirmed complete stone clearance in one patient (Fig. 5) and residual fragments in two patients, measuring 13 mm in one and two 9-mm fragments in the second (Fig. 6). Complete stone clearance was achieved after a mini-PCNL in both these patients (single tract, second day discharge). Follow-up at 1 month demonstrated no change in renal function as estimated by the creatinine clearance (Table 1).
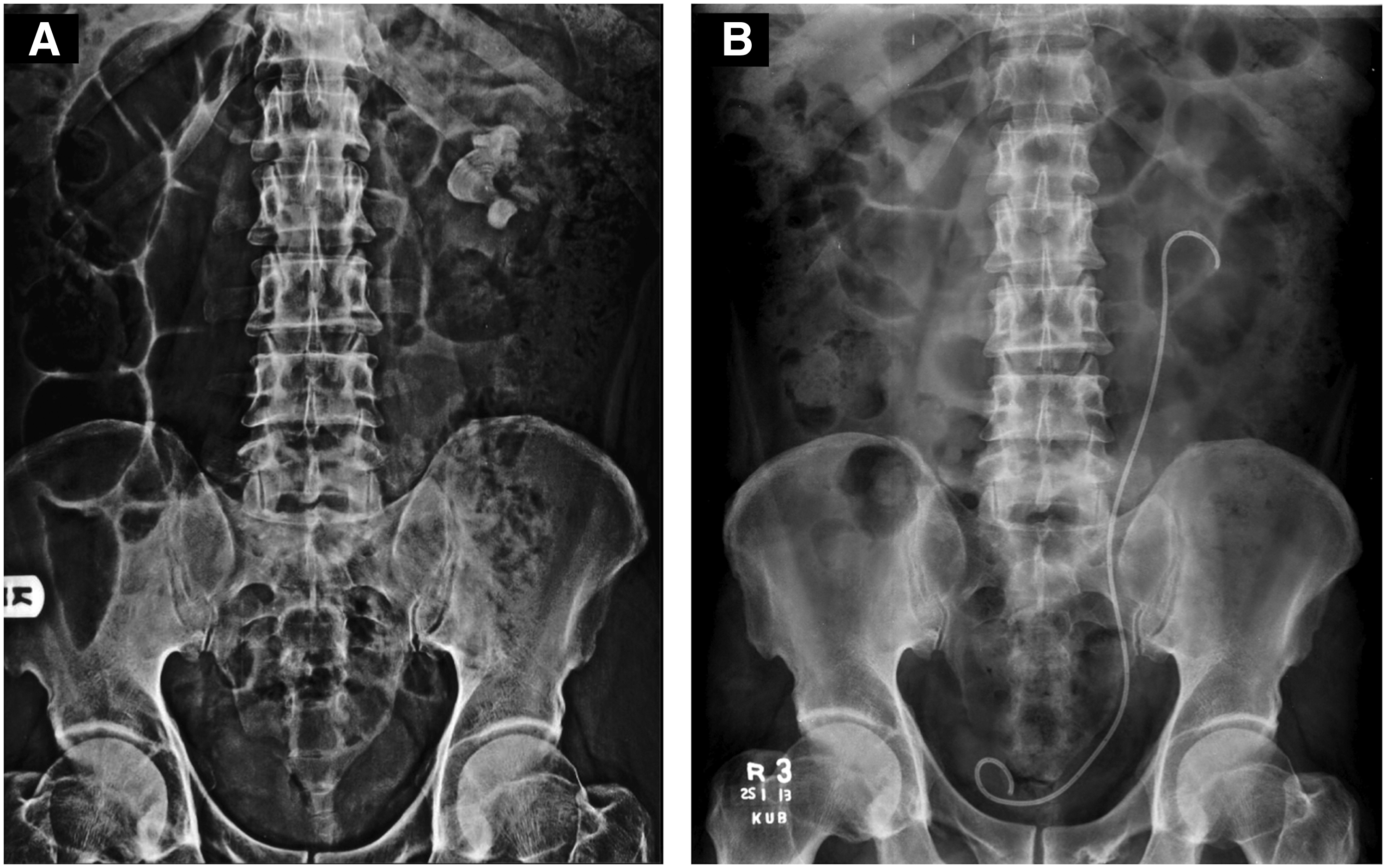
Complete stone clearance.
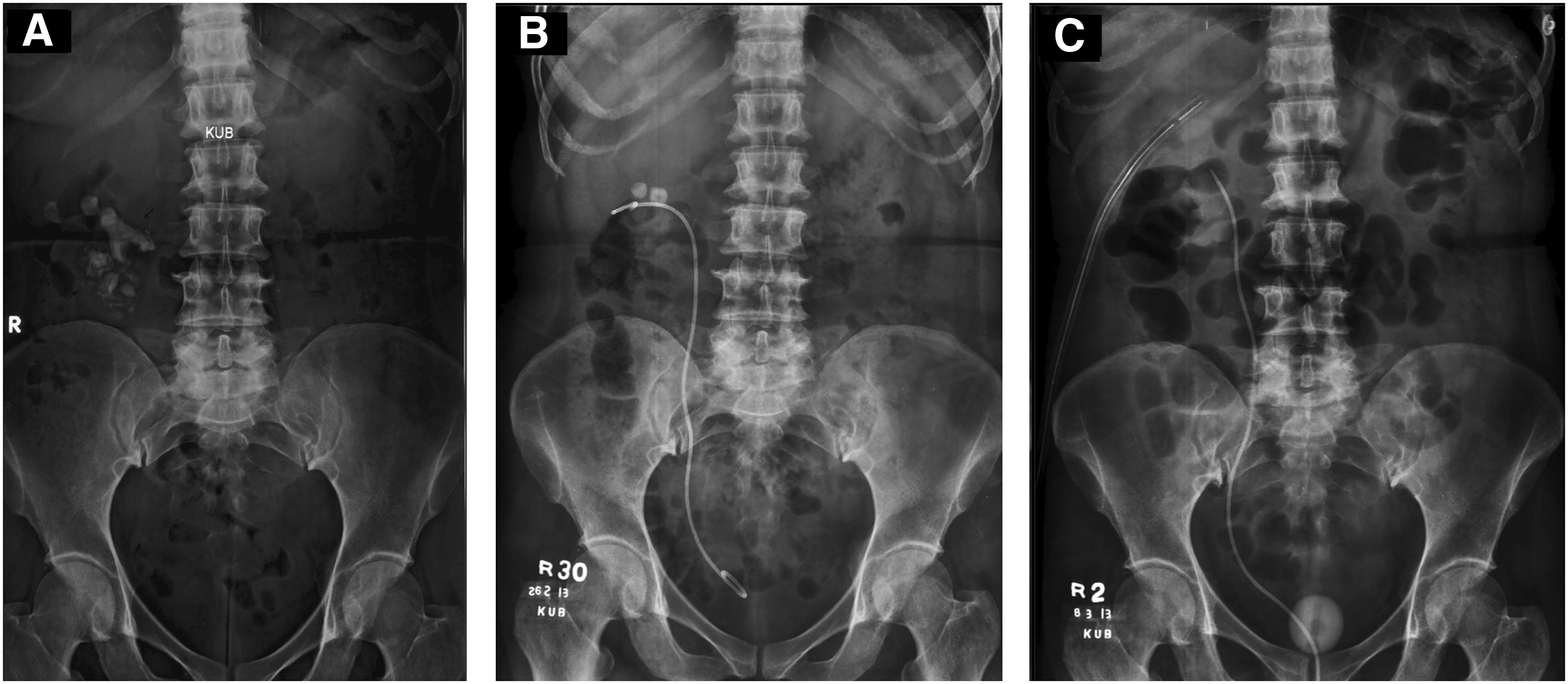
Incomplete stone clearance after robot-assisted anatrophic nephrolithotomy.
Demographic, Peri- and Postoperative Data on Patients Undergoing Robot-Assisted Anatrophic Nephrolithotomy with Ice Slush Renal Hypothermia
PCNL=percutaneous nephrolithotomy; ASA=American Society of Anesthesiologists; 3D=three-dimensional; VAS=visual analog scale.
Discussion
Kaouk and colleagues
12
first reported on laparoscopic ANL in a porcine model. Since then, laparoscopic ANL has been performed at a few centers,
5
–7,13,14
but only one case was performed under cold ischemia.
13
A summary of the data on laparoscopic ANL is provided in Table 2. Although ischemic times in our study were longer than in previous laparoscopic ANL series,
5
–7,14
our times were under cold ischemia, which is renoprotective. The cold ischemia time in the report by Deger and associates
13
was 45 minutes. The reason for the paucity of studies using cold ischemia is the difficulty in obtaining renal hypothermia during minimally invasive surgery.
15
There are no reports of ANL under cold ischemia with robot assistance
Summary of Studies Assessing Laparoscopic Anatrophic Nephrolithotomy
TP=transperitoneal; WI=warm ischemia; RP=retroperitoneal; ns=not stated; CI=cold ischemia.
It is difficult to obtain complete stone clearance of staghorn calculi with PCNL. A recent global multi-institutional survey showed stone-free rates to be 57% for staghorn vs 82% for nonstaghorn stones. 2 The stone-free rate for a complete staghorn calculus is even lower; in the United Kingdom, a national audit revealed this to be only 34%. 3 While open ANL for staghorn calculi may result in better stone-free rates (80%–100%), 17,18 it is hindered by greater blood loss, pain, and longer recovery. 19 A procedure that allows complete stone removal in one sitting with minimal morbidity would provide a definitive and cost-effective alternative to endourologic treatments over multiple sessions.
Staghorn morphometry as assessed by 3D CT has been recently proposed for planning PCNL. 10 This system categorizes staghorn stones into three types based on the probability of multiple tract(s) and stage(s) to become stone-free: Type 1 (total stone volume [TSV] <5000 mm3 with <5% unfavorable calix stone volume) would necessitate a single tract and stage, type 2 (TSV 5000 <20,000 mm3, 5%–10% unfavorable calix stone volume) would necessitate a single tract–single/multiple stages or multiple tract-single stage, and type 3 (TSV >20,000 mm3 with >10% unfavorable calix stone volume) would need multiple tracts and stages. There is, therefore, room for improvement in the surgical management of type 2 and 3 staghorn stones.
In our series, all patients had type 2 stones. We hypothesized that RANL might be better at tackling these stones than PCNL. However, we were unable to successfully clear all stones in two patients. In one patient, the remaining fragment could not be located robotically despite identification on robotic ultrasonography. To avoid further parenchymal incisions that might compromise renal function, it was decided to leave these fragments for ancillary treatment. Antegrade nephroscopy through the port could be a useful adjunct, although we did not use it in this case. The second patient was noted to have pus, so prolonged measures for stone retrieval were avoided. While we did not achieve a 100% stone-free rate, we demonstrated RANL with cold ischemia to be feasible with no complications or transfusions, and rapid recovery for the patient. There were no changes in the glomerular filtration rate as estimated by the creatinine clearance. The small volume residual fragments were easily treated with a single tract mini-PCNL, rendering all patients stone free within a month. Nevertheless, there were significant residual stones in two patients immediately after RANL.
For RANL we altered our previous ICE technique 9 and used a modified laparoscopic bag 11 to help keep the ice around the kidney. Large quantities of ice slush can be injected rapidly via the GelPOINT without losing insufflation or extending an incision. This method is less cumbersome than that described for inducing renal hypothermia during laparoscopic surgery. 15 A further advantage of the GelPOINT is the ability to immediately retrieve stone fragments and minimize loss into the peritoneal cavity. The ICE technique offers advantages typically reserved to open ANL—namely, the ability to ice the kidney to extend the window for complete stone removal and to easily remove stone fragments. Compared with a pure laparoscopic approach, the robotic technique may offer more rapid reconstruction of the collecting system, thereby shortening the ischemic time. With concomitant use of robotic ultrasonography, stones may also be identified. Given the extent of stone burden, current endourologic procedures might have resulted in more residual stones necessitating multiple surgeries, potentially leading to increased morbidity and treatment cost. Further study, ideally a randomized study comparing PCNL and RANL, could help evaluate which technique leads to maximal stone clearance, as well as determine the overall costs associated with each method for stone clearance.
Notwithstanding, certain limitations of our technique should be addressed. Specialized robotic instruments for stone retrieval are lacking. While we did not clamp the posterior branch of the renal artery to identify the Brodel line as some advocate, 4 intraoperative ultrasonography contrast with occlusion of the posterior branch may help visualize a watershed avascular area suitable for incision. This methodology has been used during RPN. 20 Although we have used the ICE technique successfully via a retroperitoneal approach, 9 we did not try it in these patients. The retroperitoneal approach may be better at containing ice as well as any leak postoperatively. Finally, whether RANL is an advance in the minimally invasive management of staghorn calculi needs further investigation in more patients and longer follow-up, especially to determine any changes in renal function. We hypothesize that RANL may be most beneficial in patients with type 3 staghorn calculi with more peripheral stone burden than pelvic burden.
Conclusion
Robot-assisted ANL with ice slush renal hypothermia is a feasible technique for selected patients with staghorn calculi. While stone-free rates do not yet approach those of the open series, this should improve with refinement of the technique and development of robotic instrumentation and ancillary equipment.
Footnotes
Acknowledgments
Khurshid R. Ghani is supported by a Fellowship from The Urology Foundation. We thank Ethicon Endo Surgery Inc., Baxter Inc., Covidien Inc., SurgiQuest Inc., and Applied Medical Inc., for providing equipment used in this study.
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.