
Abstract
Conventional articulating instruments for laparoendoscopic single-site (LESS) surgery have three major drawbacks: Weak articulating force, internal and external crowding, and mirror imaging and motion. The RoboHand™ is a recently developed novel articulating instrument. The goal of its development was to minimize the abovementioned three major drawbacks. In an ex vivo test, the joint force of the RoboHand was 2.5 to 3 times stronger than that of the LaparoAngle™ or the SILS™ instrument. In the porcine nephrectomy model, the operative times in the RoboHand group (28.8±6.6 min) were shorter than those in the LaparoAngle group (39.7±5.4 min), although not significant (P=0.146). The RoboHand prototype seems to be superior to other articulating laparoscopic instruments in its mechanical properties, such as joint force, and not to be clinically inferior to LaparoAngle for LESS. We describe the techniques for using this innovative instrument and discuss its advantages.
Introduction
L
In laparoscopic surgery, the traditional triangulation of the instruments is a critical point for surgical success, because this technique facilitates many surgical maneuvers. The single-port technique with conventional multiport laparoscopic instruments, however, does not provide the potential for triangulating the instruments used. To overcome this difficulty, instruments for LESS, such as prebent or articulating instruments, were developed. 6,9 Still, LESS performed with articulating instruments has three major drawbacks: Weak articulating force, internal and external crowding, and mirror imaging and motion.
The RoboHand™ (Movasu, Inc., Seoul, Korea) is a recently developed novel articulating instrument that has 7 degrees of freedom (Fig. 1). The distal tip can be independently bent 90 degrees both in up-and-down and right-and-left directions. The tip also freely rotates 360 degrees in axis of the instrument regardless of the bending status. The detailed use is available in the supplementary video at
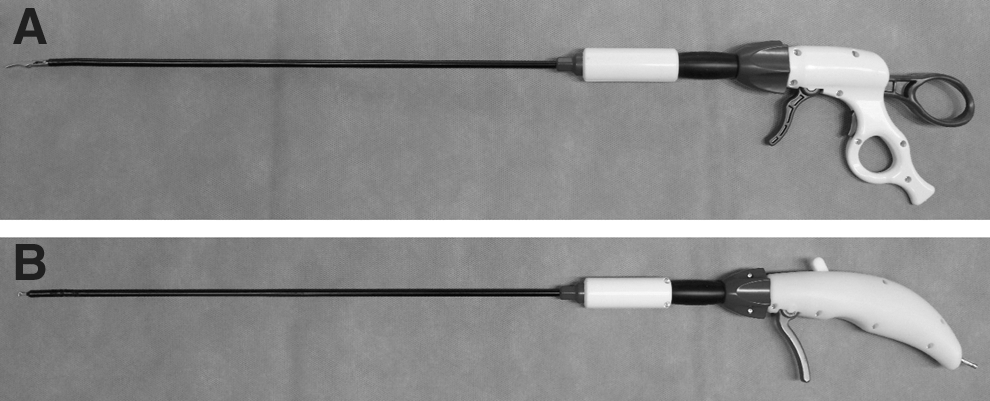
The appearance of the RoboHand™ (Movasu, Inc., Seoul, Korea), a novel articulating laparoscopic instrument.
The current experimental study aimed to evaluate the clinical utility of the RoboHand based on its prototype. We compared its bending force with that of conventional articulating instruments. We also conducted a comparative in vivo test between the RoboHand and a conventional articulating instrument, the LaparoAngle™ (Cambridge Endoscopic Devices, Framingham, MA), in a porcine model.
Technique
Ex vivo test
The bending forces of the joint were compared with those of conventional articulating instruments, the second version of the LaparoAngle and the SILS™ hand instrument (Covidien, Mansfield, MA). All of the evaluated products were the shorter versions of each product. The bending forces of the joint, from a neutral position to 20 degrees in a state of position locking, were measured by a digital push-pull gauge (Fig. 2). The angle was measured between the shaft and the end-effector of the instrument. Because the RoboHand has two joints that are independently articulated in an orthogonal direction, we measured the bending forces in each direction. The direction of the proximal joint was defined as the yaw direction, and the direction of the distal joint was defined as the pitch direction.
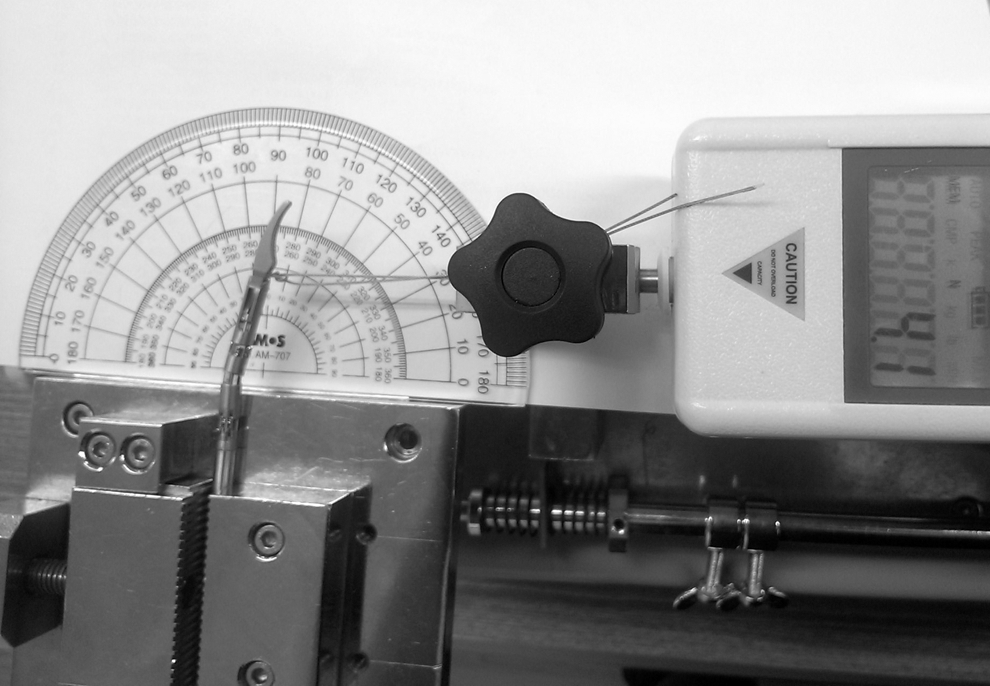
Measurement of the bending force using a digital push-pull gauge.
In vivo test
The study was conducted after obtaining approval from the Institutional Animal Care and Use Committee at the Seoul National University Bundang Hospital (Seongnam, South Korea). Six cross-bred female pigs weighing between 25 and 40 kg were included in the experiment. One surgeon with previous experience in LESS performed 12 nephrectomies in the lateral position under general anesthesia. Either the RoboHand or the second version of the LaparoAngle was used in two nephrectomies per pig, and general laparoscopic instruments were shared among the procedures. The laterality of the nephrectomies was alternately assigned in consecutive order. Single-port access was achieved through a 3-cm midumbilical incision using the OCTO™ Port (Dalim SurgNet, Seoul, Korea). We used a 5-mm, 50-cm–long 30-degree laparoscope (Karl Storz, Tuttlingen, Germany) with a right-angle light cable adaptor.
Each nephrectomy was divided into three steps, including the mobilization of the renal pedicle, the clipping and division of the renal pedicle, and the mobilization of the whole kidney. We used the same port for each pig so that the port access time was not included in the operative time. We divided 12 nephrectomies into two groups: The RoboHand group vs the LaparoAngle group. To confirm the feasibility and the safety, operative time and estimated blood loss (EBL) were compared between the groups. Intraoperative adverse events were also monitored.
Equipment
• SafetyHook (hook electrode), curved scissors, Johan forceps, Maryland forceps of RoboHand
• OCTO Port
• 5-mm, 50-cm–long 30-degree laparoscope with a right-angle light cable adaptor
• General rigid laparoscopic instruments
Role in Urologic Practice
The RoboHand had the highest bending force in both directions among all of the instruments (Table 1). It was convenient to use: Each joint could be easily modulated and locked and generated less internal and external crowding because the proximal joint and handle were not prominent. No mechanical problems or technical difficulty arose when nephrectomies were performed using the RoboHand. Porcine nephrectomies were successfully completed in 12 kidneys. The operative times in the RoboHand group (28.8±6.6 min) were shorter than those in the LaparoAngle group (39.7±5.4 min), but the difference was not significant (P=0.146). There was also no significant difference in EBL between the RoboHand (6.8±2.8 mL) and the LaparoAngle (7.4±3.0 mL) groups (P=0.843). No adverse events occurred during any of the surgeries.
N (Newton)=kg·m/s2.
Below the lower limit of measurement.
Compared with either pitch or yaw direction of RoboHand.
The RoboHand has three major advantages relative to conventional articulating instruments. First, it tends to enhance the articulating force over that of conventional instruments. One of the major problems of currently used articulating instruments is their weak joint force, which cannot meet surgeons' needs. 10 This problem is particularly maximized when the surgeon needs to achieve traction. The current products are bent in the opposite direction of the traction, even when the joint is locked. The RoboHand, however, provides a robust sustaining force in addition to an additional articulating force in the same direction (Fig. 3). Thus, its clinical utility is even higher than the utility indicated by the numerical results obtained in this study. This additional force is derived from the natural forward direction of joint articulation when using the RoboHand. In contrast, the LaparoAngle and SILS hand instruments provide a reverse direction for joint articulation.
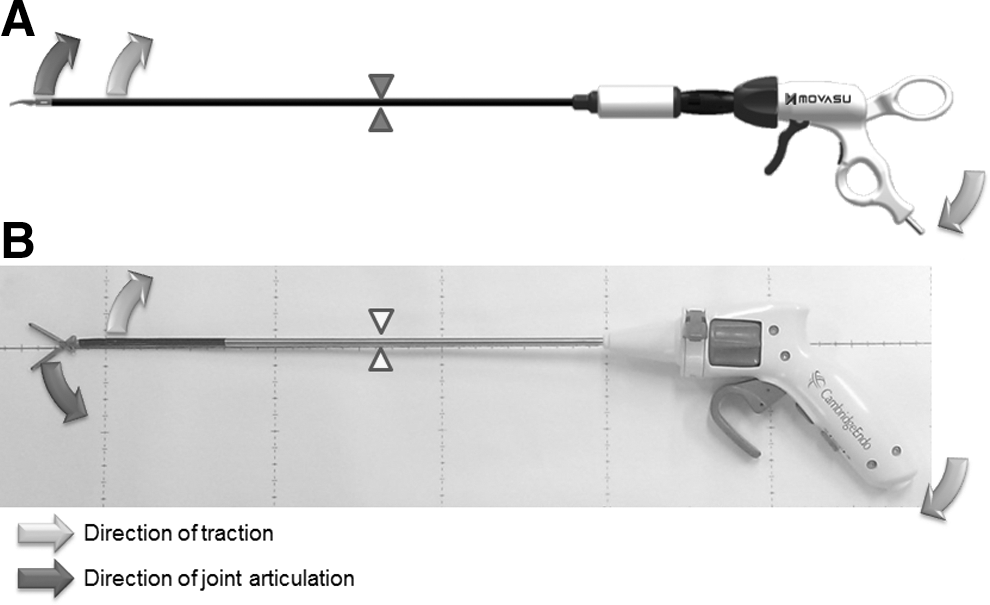
The directions of traction and joint movement.
In addition, the RoboHand™ was designed to have the lowest profile among articulating instruments to prevent external crowding (Figs. 4 and 5). The large, bulky handle of conventional articulating instruments remains suboptimal. 11 The bulkiest portion of the RoboHand has a width of only 23 mm, which is approximately half that of other instruments and represents the smallest proximal joint and handle that an operator can comfortably use to perform critical surgical procedures. The RoboHand has two lengths—ie, a short (35 cm) and a long (45 cm) version. The appropriate choice between these two instruments further enables the surgeon to prevent the clashing of instruments outside of the port.
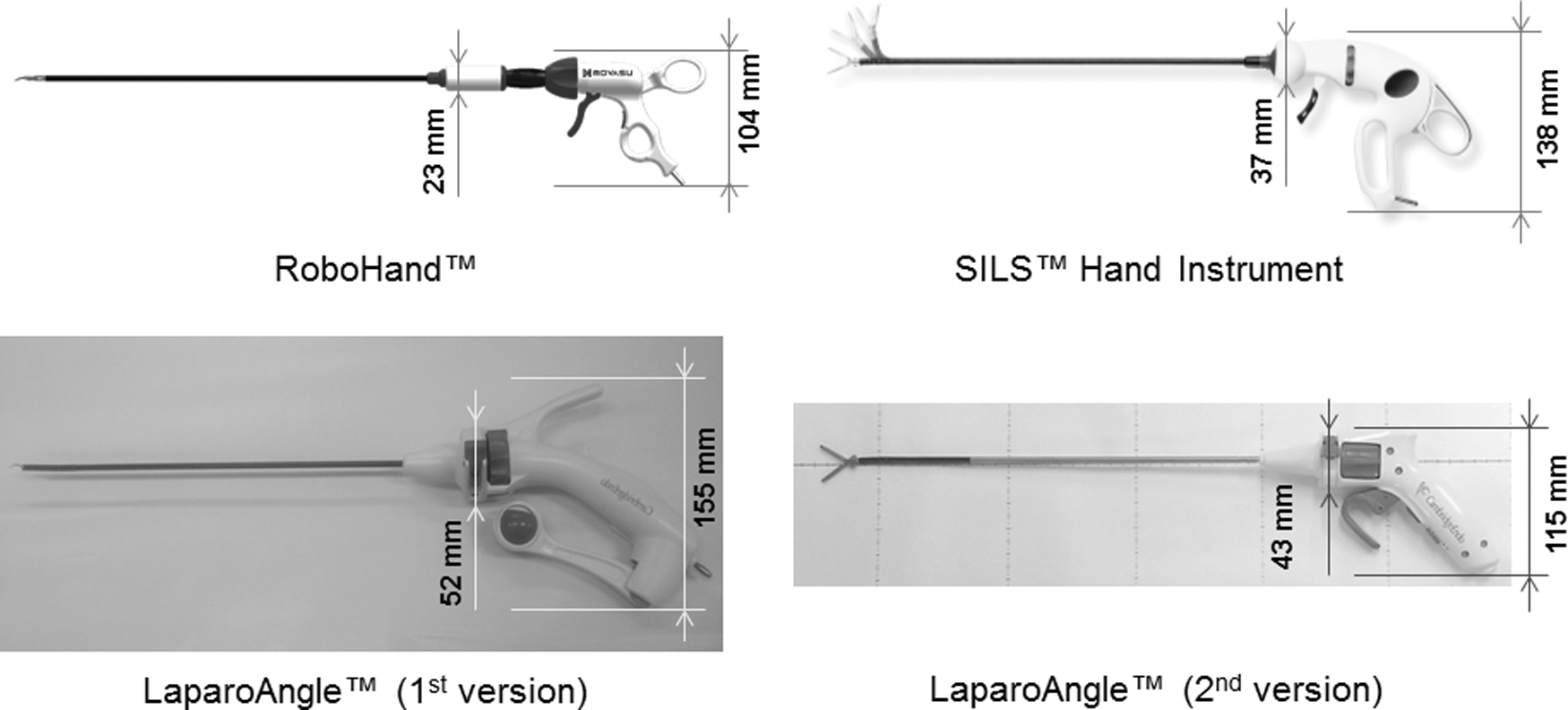
The RoboHand™ has the lowest profile among instruments.
Comparison of external crowding between the RoboHand™ and the LaparoAngle™.
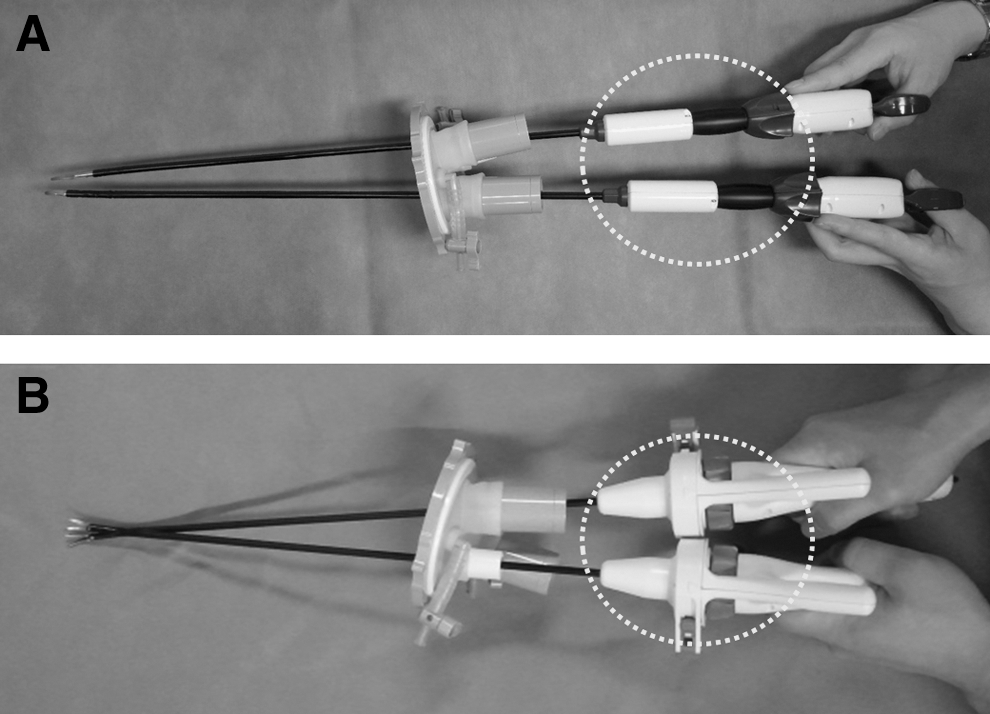
Furthermore, the RoboHand eliminates mirror imaging and motion. Conventional articulating instruments are used only in crossed positions because of their bulky handles and reverse articulating directions. The RoboHand can be used, however, in either the parallel or the crossed position because of its lower profile and forward articulating direction (Fig. 6). When used in the parallel position, internal clashing is greatly decreased, and the ergonomic forward imaging and motion in a parallel position enhance hand-eye coordination.
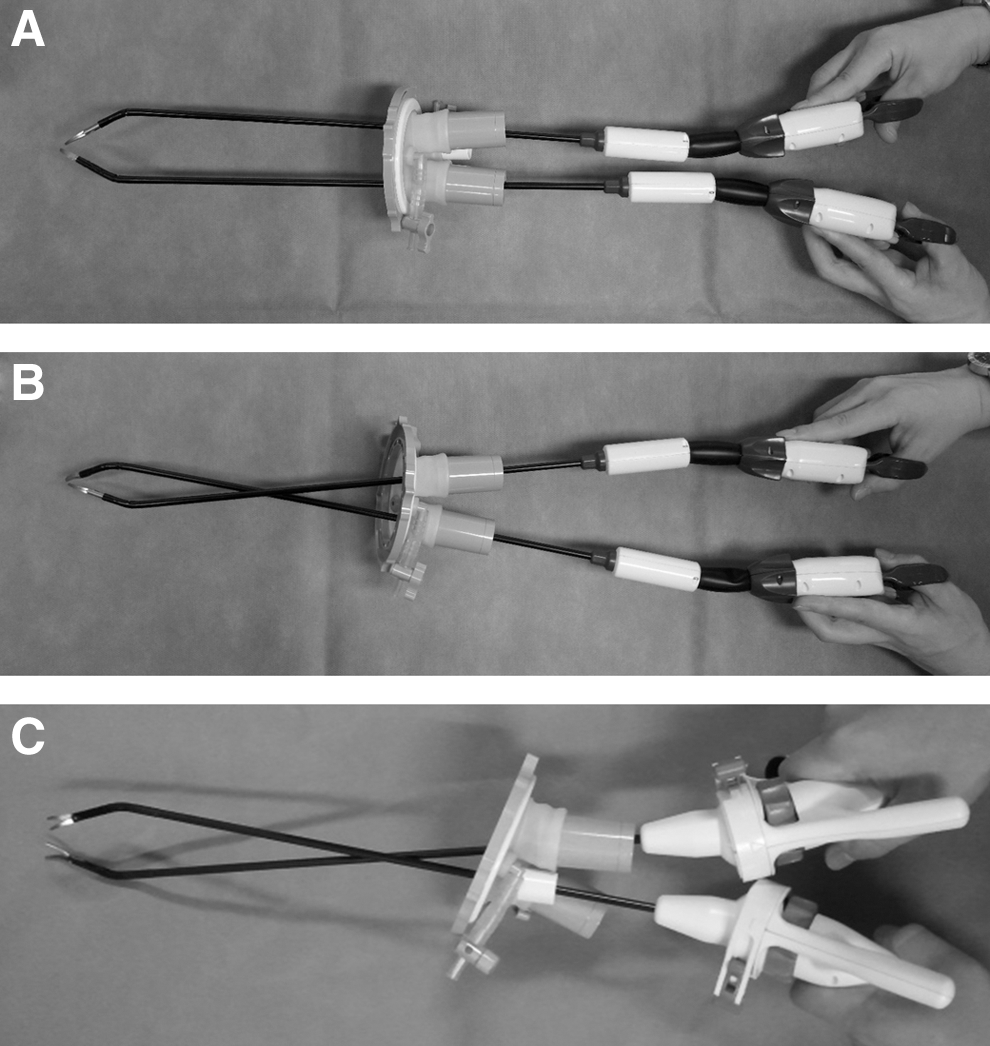
The RoboHand™ can eliminate the limitations of mirror imaging by being used in a parallel position. The RoboHand can be used in either the parallel
The SafetyHook is an electrocautery hook for the RoboHand instrument. The hook of the SafetyHook can be exposed or concealed by simple actuation, which allows the surgeon to perform electrocautery more safely. When the hook is concealed, it can be used as a traction instrument. This feature improves patient safety and provides multipurpose use (Fig. 1B).
Some authors have evaluated LESS with using conventional laparoscopic instruments and claimed that articulating instruments may not be strictly necessary. 12 These instruments, however, should be inserted through a single incision site to perform LESS, and thus the true challenges to be overcome are technical, including minimizing the triangulation of conventional laparoscopic instruments, the clashing of instruments, and the negative effects of their poor ranges of movement. 13 To counteract these drawbacks, articulating and prebent instruments have been developed. 9,14 –17 No instrument has thus far overcome the limitations of LESS completely, however.
Using an articulating instrument, the surgeon can perform delicate operating maneuvers with a higher level of complexity. When performing dissections or resections, the operator can situate the instruments in their proper positions and directions using the locking mechanism. The crucial drawback of conventional articulating instruments, however, is their suboptimal articulating power. Given the weak sustaining force of these articulating instruments, many surgeons prefer to use conventional laparoscopic instruments in their other hand. 13,16
The usual operative force for endosurgical dissection ranges from 2 to 20 N (Newton=kg·m/s 2 ). 18 In a porcine model, forces between 10.3 and 14.5 N were needed to securely tie off the ureter, renal artery, and renal vein. 10 Although the RoboHand did not achieve an absolutely satisfactory sustaining force, it did demonstrate a trend of augmented articulating power. The bending force of the RoboHand reached 2.5 to 3 times that of current articulating laparosopic instruments. Furthermore, the joint force of the RoboHand has much room for improvement, as we have only evaluated the prototype. Higher articulating force does not cause unintended injury of tissue, because the surgeon can control it by haptic feedback like conventional rigid laparoscopic instruments. Suboptimal actuation of the instrument has more possibility of tissue damage.
Prebent instruments that can simply make a triangulation have been introduced. 15 Stolzenburg and associates 9 performed a comparative evaluation in a dry and wet laboratory of conventional, flexible, and prebent instruments to determine their effectiveness and maneuverability, and found that prebent instruments were superior because they were easy to use and less time-consuming, even for less experienced surgeons. The use of prebent instruments enables the surgeon to exert greater force on the tip during surgery relative to other types of instruments. The limited degrees of freedom are important shortcomings of prebent instruments, however. During surgery, the directions of the instruments can be critical to advance to the next step of the procedure, and the limitation of movement can cause difficulties for inexperienced surgeons. A surgical task using prebent instruments reported by Tracy and colleagues 2 was expected to necessitate a steeper learning curve relative to the flexible instrument.
We concur with the concept of the trade-off between flexibility and maneuverability 19 ; however, if an articulating instrument is used not in a flexible state but in a rigid position-locked state, its maneuverability may be the same as that of a prebent instrument. Furthermore, if an articulating instrument can be easily switched between flexible and rigid states, it can benefit from both higher degrees of freedom and maneuverability. We believe that the RoboHand is one such instrument. Its functionality, including position locking and unlocking, can be easily controlled by one hand alone, which maximizes ergonomic control and operability.
LESS is one of the most rapidly evolving procedures in the field of minimally invasive surgery. The technique using this innovative articulating laparoscopic instrument might enhance operability and clinical outcomes for any kind of LESS in urology.
Conclusion
The RoboHand prototype seems to be superior to other articulating laparoscopic instruments in terms of its mechanical properties, such as joint force. In addition, the RoboHand seems to not be inferior to the LaparoAngle for LESS nephrectomy. Official products will soon be released, and the RoboHand may prove itself to be clinically useful for overcoming the present obstacles of LESS instruments.
Footnotes
Acknowledgments
This research was financially supported by the Ministry of Knowledge Economy (MKE) and the Korea Institute for Advancement of Technology (KIAT) through the Research and Development for Regional Industry.
All of the experiments were conducted after obtaining approval from the Institutional Animal Care and Use Committee (IACUC) at the Bundang Hospital of Seoul National University (Seongnam, South Korea). The IACUC number is BA1204-102/027-01.
We wish to thank Ji Yeon Hwang, a veterinarian at the Seoul National University Bundang Hospital, for caring for the animals. We also thank Dr. Pradeep P. Rao (Mamata Hospital, Maharashtra, India) for his scientific comments.
Disclosure Statement
Dr. Chang Wook Jeong is a stockholder of Movasu, Inc. For the remaining authors, no competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.