
Abstract
Objective:
To show the benefit of trocar-sharpened needles for image-guided prostate biopsy compared with standard bevelled needles in patients.
Materials and Methods:
Twenty-four men underwent magnetic resonance imaging-targeted fusion-guided transperineal saturation prostate biopsy, each with half standard bevelled and half trocar-sharpened needles. All taken biopsies were scored (1=worse to 5=best) by one urologist for the following criteria. (1) Accuracy of matching between planned and performed biopsy. (2) Histologic quality of the sample. (3) Elegance, which is the easiness to take the biopsy in proper time, planned position, and best histologic quality. Afterward, the histologic sample quality was evaluated by a blinded pathologist. To show a possible training effect, blinded untrained junior residents performed biopsies in four men (103 cores).
Results:
Overall, 600 single biopsies were analyzed. The trocar-sharpened needles demonstrated a significantly (p<0.05) better scoring for accuracy and elegance rated by the urologist. The histologic quality scored by the pathologist was superior. Moreover, significantly lower target errors with trocar-sharpened needles were achieved by untrained residents, but not by the experienced user.
Conclusion:
Using trocar-sharpened needles helps urologists to perform targeted prostate biopsy more elegantly and accurately. In addition, the histopathologic sample quality was superior, which may directly improve diagnostic certainty. There is an undeniable training effect in image-guided biopsy and unexperienced users can significantly reduce target errors with trocar-sharpened needles.
Introduction
P
To reduce underdiagnosis found in 30% 4 using conventional transrectal ultrasound (TRUS) biopsy, 5 the integration of imaging is a promising method. For multiparametric magnetic resonance imaging (mpMRI), it has been shown by multiple groups that clinically significant PC can be visualized and detected. 6,7 The detection rate is associated with tumor volume and grade and has a sensitivity up to 92% and a specificity up to 100% for larger tumors. 8 –11 However, Roethke et al. published sensitivities of only 26% in lesions smaller than 5 mm. 12 Furthermore, prostatic tumors are often heterogeneous and may contain in more than 60% high-grade lesions of 0.3 mL. 13 Extracting histology especially out of small lesions is crucial for a reliable diagnosis. 14
Systematic biopsies with freehand TRUS guidance have suboptimal detection rates. 15 Since in-bore MR-guided prostate biopsies are limited in clinical routine, 8,16 –19 a combination of ultrasound (US) and MRI seems to be a more practicable alternative. 5,20 –26 Our group previously described a perineal prostate biopsy platform (BiopSee®; MedCom, Darmstadt, Germany), 27 which integrates preinterventional mpMRI-data with periinterventional US. In phantom validation studies, the overall targeting error of MRI/TRUS-fusion biopsies was around 1 mm. 28 However, in clinical routine, we experience deviation away from the planned needle trajectory when using conventional needles due to their not centered bevelled needle tip. Driving these needles to the planned intraprostatic positions can be time-consuming and especially for less experienced users difficult because of the permanent deviation away from the bevel. These characteristics compromise the accuracy and the diagnostic reliability especially in small lesions.
To overcome these limitations, we suggested a novel needle-tip design (Fig. 1), with its tip more centered like a standard trocar placement set for laparoscopic surgery, to achieve less deviation and target lesions more easily during image-guided biopsy. In a phantom model, we have shown a significantly higher accuracy with the trocar-sharpened biopsy needle with an overall target error of only 0.13 mm. 29 In this study, we report about the first clinical application and show the potential benefit of trocar-sharpened needles for image-guided prostate biopsy compared with standard bevelled needles in patients.
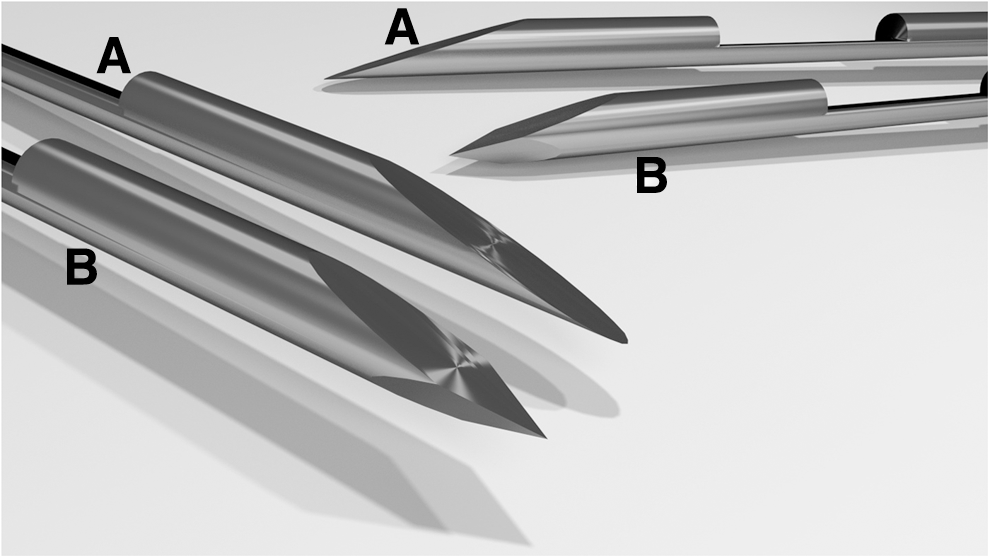
Standard bevelled needle (
Patients and Methods
After written informed consent, 20 consecutive men with a median age of 67 were included in the first part of the study (497 cores). Nineteen men had a suspicion of PC with PSA levels between 3.9 and 22.7 ng/mL, and four patients were suspicious on digital rectal examination (cT2). One had a transurethral resection of a prostatic adenoma 15 years ago, and one had experimental high-intensity focussed US therapy 2 years ago for intermediate-risk PC. All men underwent preinterventional mpMRI at 3 Tesla without an endorectal coil, as described previously. 27 Seventeen men had at least one suspect lesion on imaging.
During the following transperineal MRI-targeted prostate biopsy with software registration (MedCom), the US probe was fixed to a custom-made mechanical stepper. 27 Rotation and probe depth are tracked by built-in encoders. A biopsy template for needle insertion is placed on the stepper. After setting up the system, a three-dimensional dataset is acquired by recording a series of transversal two-dimensional images while pulling back the probe. Segmentation of the prostate and lesions, as well as registration to the MR-dataset is software assisted with manual control. Next, virtual biopsy cores are planned depending on the prostatic volume and amount of lesions on mpMRI (18 to 30 cores, mean 25±2.5). The biopsy procedure itself starts by rotating the US probe to the planned biopsy core, which is visualized with an augmented reality live image in the sagittal plane. While inserting the biopsy needle, deviations from the planned trajectory can be recognized easily and in real time. The final biopsy position is marked on the screen and the deviation toward the planned position is calculated automatically by the system (Fig. 2).
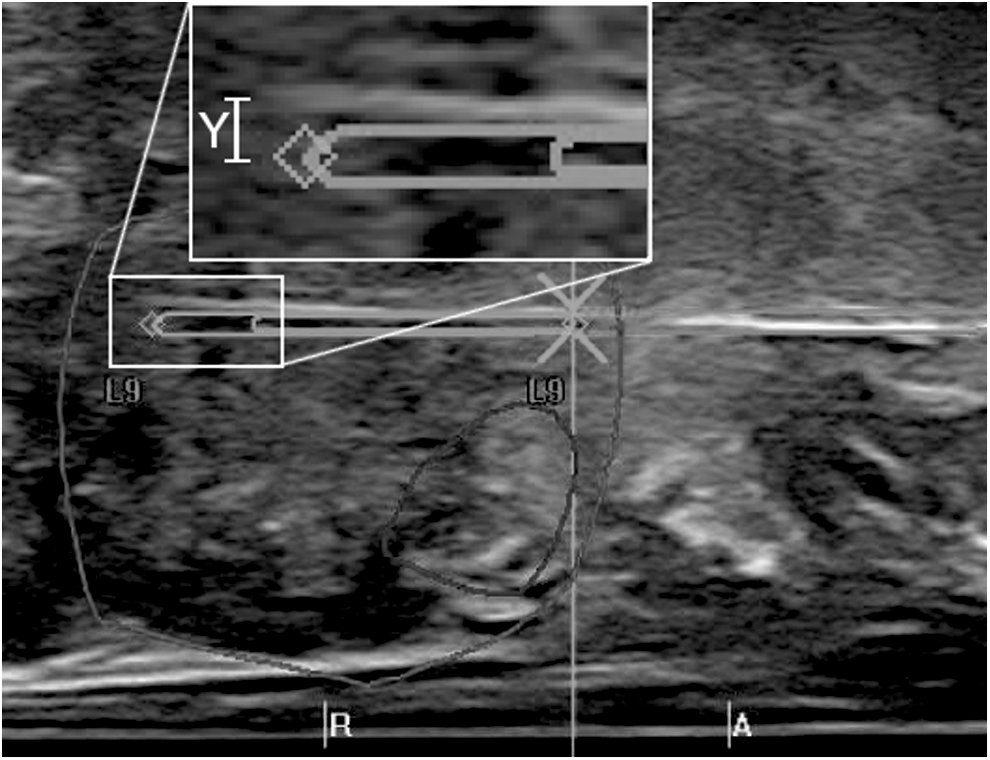
Sagittal live image during the biopsy procedure. Deviation of standard bevelled biopsy needle in transversal plane between the planned trajectory and the biopsy can be recognized immediately (Y).
Half of the biopsies were taken with conventional bevelled and the other half with trocar-sharpened needles. Both needles were 18G, with a length of 240 mm, same stiffness and same possible sample length up to 19 mm (Uromed KG, Oststeinbek, Germany). In each patient, one half of the prostate was biopsied with one of the needles. Both the order of the needles and which half of the prostate was biopsied with which needle-type was assigned randomly. Each single biopsy was immediately scored (1=worse to 5=best) by the performing urologist for three criteria. The accuracy is defined as the impression of matching the planned and performed biopsy. The macroscopic tissue quality of the sample was evaluated by the urologist after biopsy, and if there was not enough good tissue, the biopsy was repeated and scored as 1. Last, the elegance of biopsy was reviewed. It is defined as the easiness to take the biopsy in proper time at the planned position and with best histologic quality. After the procedure, the histologic quality was evaluated again by one blinded experienced genitourinary pathologist. He did not know which biopsy needle was used and scored according to the sample volume, crushing defects, and fractionation of every biopsy core.
To determine a possible training effect, two unexperienced urologists starting residency, who never performed either perineal or transrectal biopsy before, biopsied another two patients each under supervision by an experienced user (55 and 48 cores). For the second resident, the needle type was changed after each biopsy. Both novices were blinded to the needle type they were using.
Statistical analyses were performed using the open source software PSPP (V0.8.0, licenced under GPLv 3,
Results
There were 497 single biopsies done and evaluated by an experienced urologist who performed more than 100 MRI-targeted prostate biopsies previously. In 120 cores (21.74%) PC was found. Overall, 11 of 20 men were diagnosed with PC: four patients had Gleason 6 (3+3), one had both a Gleason 6 and a 3+4 lesion, two had Gleason 3+4 tumors, three had Gleason 4+3, and one had a Gleason 9 (4+5) tumor. The results for the criteria elegance, accuracy, histologic quality, and the target error in the transversal plane are shown in Table 1.
Means without unit (1=worse to 5=best) except for target error in the transversal plane (mm).
For elegance and accuracy scored by the urologist as well as for histologic quality rated by the urogenital pathologist, two-tailed t-tests show a significant difference between both needle types (p<0.05). The p-value for macroscopic histologic quality rated by the urologist is 0.08 and the p-value for the target error calculated for the transversal plane is 0.38.
If the data are split in biopsy cores targeting MRI-suspicious lesions (40 trocar-sharpened, 42 bevelled needles) and conventional systematic biopsies (207 and 208, respectively), the histologic quality shows a significant difference for the targeted suspect lesions, both rated by the urologist (4.23±1.03 and 3.57±1.32, p=0.01) and rated by the pathologist (3.7±0.52 and 3.07±1.05, p=0.001).
Similarly, when dividing data by the tumor detected in the core (74 trocar-sharpened, 36 bevelled needles) or not (173 and 214, respectively), a significant difference between the two needles for histologic quality as rated by the pathologist remains for positive cores (3.9±0.29, respectively, 3.66±0.76, p=0.019).
The results of the four extra patients in whom 103 biopsies were performed by two untrained junior residents also showed significantly better results for the trocar-sharpened needle in elegance, accuracy, and histologic quality, rated by both by the pathologist and the urologist (Table 1). Moreover, for the novice urologists, significant differences were shown for target errors in the transversal plane (novice 1: 0.55 mm vs. 1.07 mm, p=0.004, novice 2: 0.74 mm vs. 3.12 mm, p=0.0002).
Discussion
Image-guided prostate biopsy is gaining worldwide acceptance and is being implemented in the clinical routine in more and more centers for optimal diagnostics of small suspect prostatic lesions. Lately, the integration of mpMRI imaging has been proven to be superior for the purpose of detecting clinically significant cancer. 30 MpMRI-targeted fusion-guided transperineal prostate biopsy became the new standard in our clinic 3 years ago.
In a previously published cohort of over 100 patients using the BiopSee-platform, the procedural targeting error was around 3 mm. 27 One source of this error besides soft tissue movement is the intrinsic deviation of the used conventional bevelled biopsy needle while pushing it into the prostate. Experienced users can compensate this characteristic, but need more time and often have to reposition and reinsert the needle in the prostate. This elongates anesthesia time and may cause more prostatic damage with all possible complications. A centered trocar-sharpened needle tip leads to a significantly better target error that has been shown not only in our previously presented phantom study but also in other applications such as spinal anesthesia. 29,31 In the first clinical evaluation presented here, we found slightly better target errors, but without a significant difference between both needle styles for an experienced user. This result can easily be explained because of the long experience with bevelled needles of the urologist performing the biopsies within this study and the use of live US that visualizes the deviation for immediate correction. To show the training effect, two untrained urologists who did not know which needle was used performed another 55 and 48 biopsies. Herein, the new needle design demonstrated a significantly lower target error. The lower overall target error of the novice compared with the experienced user may be explained by the lower number of cores, the direct teaching by an experienced user, and the longer procedural time the junior used to perform biopsies in a perfect manner instead of in a clinical routine.
More importantly than target errors, the overall clinical application of the novel trocar-sharpened needles was successful. From the urologist's point of view, the novel design is significantly more elegant and more precise to use than the conventional needle. This means no reinsertion or correction of the needle, which may lead to less tissue damage and shorter procedural time. Since the needles could not be blinded to the experienced user, these values are subjective. A difference in the overall macroscopic tissue quality was not seen by the urologist. However, the pathologist who did not know which core was taken by which needle noted a significant advantage of the trocar-sharpened needles. This improved sample quality may translate to a higher diagnostic reliability.
In MRI-targeted biopsies from suspect lesions, the urologist rated better tissue core quality in trocar-sharpened needles compared with bevelled needles. This was confirmed by the pathologist. The quality of biopsies positive for tumor, which is not known by the urologist, also was superior in the trocar-sharpened cohort as rated by an experienced genitourinary pathologist. This leads to the conclusion that the trocar-sharpened needles increase the sample quality even though the body of the needles except for their tips is not different. This might be explained by reduced friction within the tissue of the novel tip design. The more complex tip design leads to an increased production cost and a slightly higher whole sale price (currently 17.90 Eur vs. 12.90 Eur in Germany).
A limitation of the current study is that there is no way to blind an experienced user to the used needle style. Furthermore, we used a scaled scoring system from 1 to 5, which can be used differently between individuals. To overcome this problem, all classifications were done by the same person.
Conclusion
The novel trocar-sharpened needle style improves the performance of taking image-guided biopsies as well as the histologic quality. Since these novel needles are safe to use for all image-guided biopsy procedures such as CT-guided biopsy, urologists could apply them for superior quality.
Footnotes
Acknowledgment
The authors thank Mr. Werner Knopp of Uromed KG, Oststeinbek, Germany for his support in the production of the novel needle design.
Disclosure Statement
Boris Hadaschik received research support from Uromed. For the remaining authors, no competing financial interests exist.