
Abstract
Background and Purpose:
A unilateral paravertebral (PVB) block with catheter can provide extendable analgesia without physiological changes. The objective of this study was to assess the efficacy of PVB bupivacaine for providing perioperative pain relief in adults undergoing percutaneous nephrolithotomy (PCNL) under general anesthesia.
Methods:
Fifty American Society of Anesthesiologists Grade I, II patients, aged 18 to 65 years, were included in this prospective, randomized, controlled, observer blinded trial. PVB group patients received preinduction 20 mL of 0.5% bupivacaine in the T9–10 paravertebral space and a catheter in addition to general anesthesia. Control group patients received only general anesthesia. All patients received intravenous fentanyl (2 μg/kg on induction, 0.5 μg/kg on 20% increase in heart rate or mean blood pressure) and paracetamol every 6 hours. Postoperative pain was assessed using the visual analog scale (VAS) (0–10 cm) at rest and movement by a blinded observer at 0, 1, 2, 4, 6, 12, and 24 hours postoperatively.
Results:
Data of 48 patients were analyzed. Intraoperative fentanyl requirement was higher in the control group (2.74±0.75 μg/kg [95 % confidence interval (CI) 2.42, 3.05]) than the PVB group (2.07±0.26 μg/kg [95 % CI 1.96, 2.18]), (P=0.0001). Time to first postoperative analgesic requirement was longer in the PVB group (120 min [30-570]) than the control group (30 min [0-180]), (P=0.0000). The VAS on rest (0, 1, 2, and 12 h) and movement (all time points) were significantly lower in the PVB group. Postoperative fentanyl consumption was lower in this group (175 μg [25-475]) compared with the control group (525 μg[(150-1275]), (P=0.0000).
Conclusions:
Unilateral PVB block with catheter provided effective perioperative analgesia for PCNL.
Introduction
P
Managing this pain with opioids can lead to sedation, nausea, vomiting, and constipation, which defeat the purpose of this minimally invasive procedure. A unilateral paravertebral (PVB) block with a catheter offers the option of providing extendable perioperative pain relief without the above side effects or the physiologic derangement associated with local anesthetics in the central neuraxial space. 7,8
Two randomized controlled trials have assessed the efficacy of the PVB block for PCNL. 9,10 In one study, lumbar PVB was performed and a catheter inserted for providing intraoperative surgical anesthesia, 9 whereas in the other, a one-time multiple level thoracic PVB (T10–T12 level) was administered at the end of surgery to provide postoperative analgesia. 10
No study has assessed whether a single level ipsilateral PVB block with catheter would provide intraoperative and postoperative pain relief and improve the quality of recovery in patients undergoing PCNL under general anesthesia.
The aim of this randomized controlled trial was to ascertain the above parameters.
Methods
The study was approved by the Institutional Ethics Committee and registered with the clinical trial registry of India (CTRI/2011/091/000101).The primary end point was to compare pain at rest in patients with or without a PVB block using a visual analog scale (VAS). The secondary end points were comparison of VAS pain on movement, intra- and postoperative fentanyl requirement, peak expiratory flow rates (PEFR) at 6 and 24 hours postoperatively, tramadol consumption after transfer to a ward, and the quality of recovery (QoR) at 24 hours postoperatively. Anticipating 2-cm difference in the VAS as the desired difference with a standard deviation (SD) of 2 cm (observed in a previous study of PVB), 11 the estimated sample size was 22 per group with α=0.05 and power of 90%. Assuming a 10% attrition, we aimed to include 25 patients per group in the study.
Patients who were 18 to 65 years old, with American Society of Anesthesiologists Grade I–II, and who were scheduled for PCNL were enrolled between January and November 2011. Exclusion criteria were refusal to participate, inability to comprehend, infection at site of block, severe chest wall deformity, coagulopathy, or hypersensitivity to local anesthetics. Patients in whom surgical complications (hydrothorax, urosepsis, excessive bleeding) developed that were likely to confound pain assessment were excluded from the analysis.
All patients were familiarized with the Ganshron LF 8 spirometer (Spirojet; Ganshron Medizin Electronic; Niederlauer, Germany); a 0–10 cm VAS, (0=no pain, 10=worst imaginable pain); and a patient controlled analgesia (PCA) device (Medima s-PCA, Warszawa, Poland) before surgery. A mean of three measurements was used to estimate the PEFR on the evening before surgery and at 6 and 24 hours postoperatively.
On the morning of surgery, patients were transferred to the anesthesia room 30 to 45 minutes before surgery. Routine monitoring (heart rate [HR], electrocardiography, oxygen saturation, and noninvasive mean blood pressure [MBP]) was started, 30 μg/kg midazolam was administered intravenously (IV), and baseline parameters noted. Thereafter, patients were randomly allocated to either the control group or the PVB group after opening opaque, sealed envelopes containing computer generated random numbers. Patients in the control group were administered general anesthesia alone whereas PVB group patients were administered the PVB block followed by general anesthesia.
Paravertebral block technique
The block was performed with patients sitting, their dorsal spine arched. After infiltrating 2% lignocaine (3–5 mL), a 16-gauge Tuohy needle (Portex, Smiths Medical International Limited, Keene, NH) was inserted 2.5 cm lateral to the spinous process of the ninth thoracic vertebra (T9), advanced perpendicularly until the T10 transverse process was encountered (usually at 3–4 cm). The needle was then withdrawn 0.5–1 cm, and walked off the upper end of the transverse process and advanced further by 1.5 cm. Thereafter, following negative aspiration for blood, cerebrospinal fluid, or air, 20 ml of 0.5% bupivacaine (Anawin, Neon Laboratories, Tarapur, India) (total dose 100 mg, not exceeding 2 mg/kg) was injected. Any coughing, difficulty in breathing, and paresthesias were noted. Thereafter, a compatible catheter was advanced 4 cm into the paravertebral space and fixed at the skin.
Anesthesia
Anesthesia was induced (propofol 2–3 mg/kg, fentanyl 2 μg/kg, vecuronium 0.1 mg/kg IV) followed by endotracheal intubation. Controlled ventilation was provided with oxygen, nitrous oxide (50:50), isoflurane (1–1.5% dial setting), 1 L/minute fresh gas flow. All patients received 1 g paracetamol IV every 6 hours.
All patients initially underwent retrograde urography (lithotomy position) and were then turned prone. Depending on the location of the renal calculus, a supra or infra 12th rib puncture was performed under fluoroscopic guidance and the tract dilated, following which a 30F Amplatz sheath and 26F rigid nephroscope were inserted. Hemodynamic parameters were noted every 5 minutes until skin puncture and thereafter every 15 minutes until the end of the procedure.
For an intraoperative increase in HR or MBP more than 20% above baseline, 0.5 μg/kg IV fentanyl was administered. At the end of the operation with the patient prone, 5 to 10 mL of water soluble radiopaque dye (Iohexol, Omnipaque 350 mg/mL, GE Healthcare Inc, Shanghai, China) was injected in the PVB catheter and dye spread visualized flouroscopically. Thereafter, patients were turned supine, the neuromuscular block reversed, and the trachea extubated.
Pain at rest and on deep breathing (movement) was assessed using the VAS score by a blinded observer immediately after transfer to the postanesthesia care unit (PACU) (0 hours) and at 1, 2, 4, 6, 12, and 24 hours postoperatively.
Time to VAS score of more than 3 on rest after extubation was noted as time to first analgesic requirement. For initial pain relief, boluses of fentanyl (25 μg IV) were administered until VAS score decreased to 3. After this, all patients were started on the PCA device (bolus 25 μg fentanyl, lockout interval 5 minutes, 4-hour maximum dose 400 μg). Patients in the PVB group were simultaneously administered 20 mL 0.25% bupivacaine (total dose 50 mg, not >2 mg/kg) through the paravertebral catheter.
The total PCA fentanyl consumed was noted. Patients with intractable pain despite PCA use were administered rescue analgesia (morphine100 μg/kg IV boluses every 15 minutes until the VAS score decreased to 3).
The next morning, the PCA device was disconnected; PVB group patients were readministered 20 mL of 0.25% bupivacaine (total dose 50 mg) and transferred to the ward where those with VAS score of ≥3 at rest were administered tramadol 50 mg IV to be repeated every 4 to 6 hours if needed. Thereafter, the total tramadol consumed in the next 12 hours, postoperative nausea/vomiting (PONV) during the study period, and the QoR 12 at 24 hours postoperatively were assessed and the PVB catheter removed.
Statistical analysis
Analysis was performed using STATA 9.0 (College Station, TX). Data were presented as number (%) or mean±SD/median (range). Between groups, continuous baseline parameters were compared using the Student t test, categorical variables compared using the chi square test, hemodynamic parameters over time compared using repeated measures analysis of variance. The primary outcome, VAS score at rest, was compared using the Student t test for independent samples.
The difference of mean of intra- and postoperative fentanyl requirement was compared using the Student t test. The median difference in VAS score at various time points between the groups was compared using the Wilcoxon rank sum test. The normality of VAS score at various time points was tested using Shapiro Wilk test.The difference in PEFR was compared using the Wilcoxon rank sum test. The QoR score was compared using the Student t test. P value of <0.05 was considered statistically significant.
Results
The demographic parameters, duration of anesthesia and surgery were comparable between the groups. Hydropneumothorax developed in one patient from each group because of a supracostal nephrostomy tract, and both were excluded from the study. Therefore, data of 48 patients were analyzed with 24 patients in each group (Table 1). Five patients in the control group (20.83%) and 10 (41.67%) in the PVB group had supra-12th rib punctures (P=0.23).
SD=standard deviation; ASA=American Society of Anesthesiologists.
The median time taken to perform the PVB was 10 (5–20) min, and the median time from PVB block administration to skin puncture for PCNL was 55 (15–135) min.
Blood in the catheter (PVB group) was observed in three patients, necessitating slight catheter withdrawal in two and resiting in one. No other adverse effects were observed.
Intraoperative hemodynamics (HR, MBP) were comparable between the groups. Intraoperative fentanyl requirement was greater in the control group (2.74±0.75 μg/kg, [95 % confidence interval (CI) 2.42, 3.05]) compared with the PVB group (2.07±0.26 μg/kg, [95 % CI 1.96, 2.18]), (P=0.0001).
Twenty-two patients in each group had one nephrostomy tube (28F) inserted postoperatively; two patients each in the control and PVB groups had multiple nephrostomy tubes (26F) (two tubes each except one patient in the control group had three tubes).
Fluoroscopic visualization of dye spread through the PVB catheter was performed in 16 patients. Longitudinal spread was observed in 12, 2 had both longitudinal and intercostal spread, and 2 patients had a cloud-like spread.
The VAS score at rest was lower in the PVB group compared with the control group in the postoperative period at all time points of observation. The difference was statistically significant at 0, 1, 2, and 12 hours postoperatively (Fig. 1). The VAS score on movement (deep breathing) was, however, significantly lower in the PVB group at all time points studied (Fig. 2).
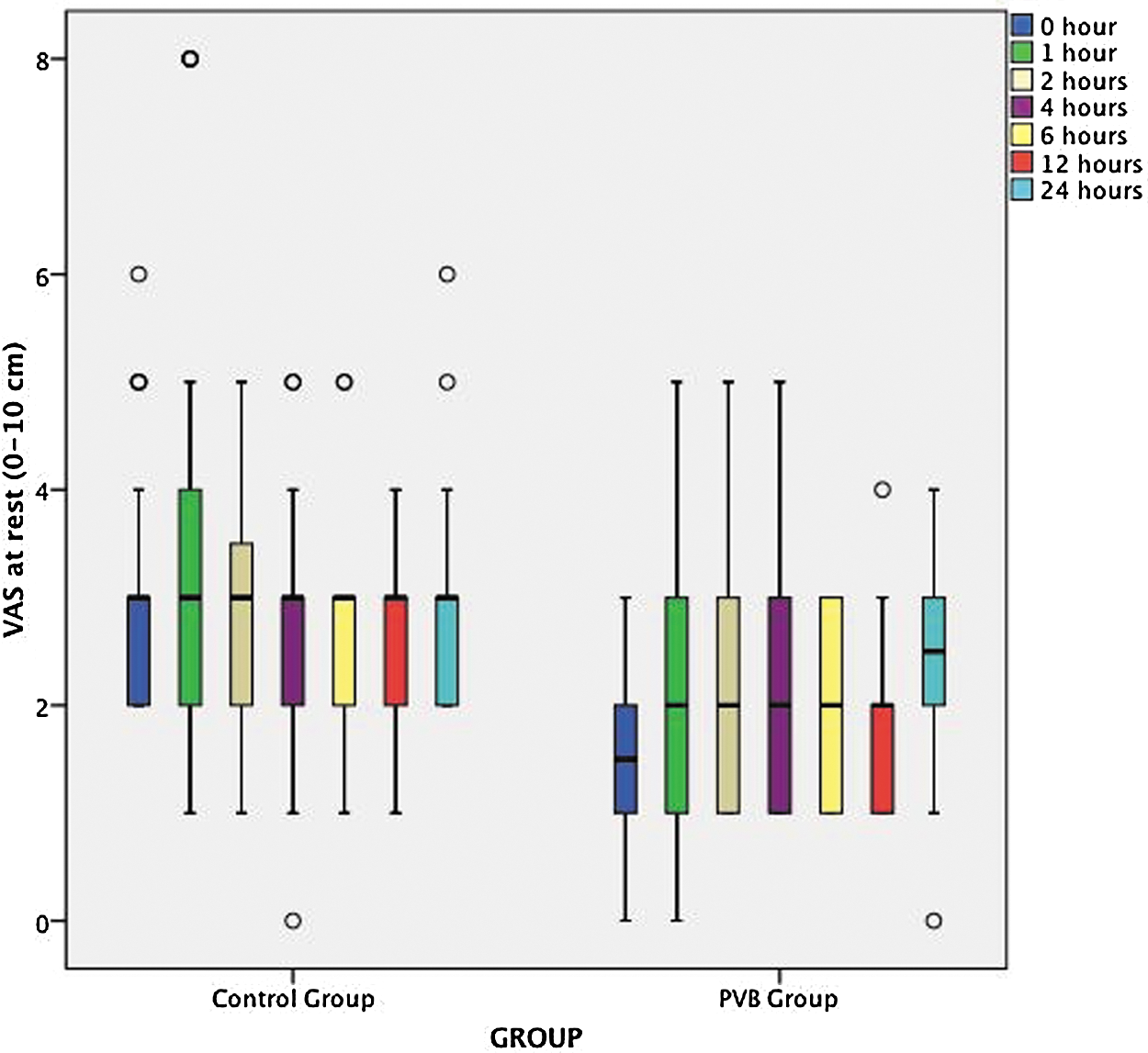
Comparison of visual analog scale (VAS) scores at rest in the postoperative period. The median, interquartile range (box), and the 5th and 95th centiles are shown. The circles represent patients lying outside the range. PVB=paravertebral.
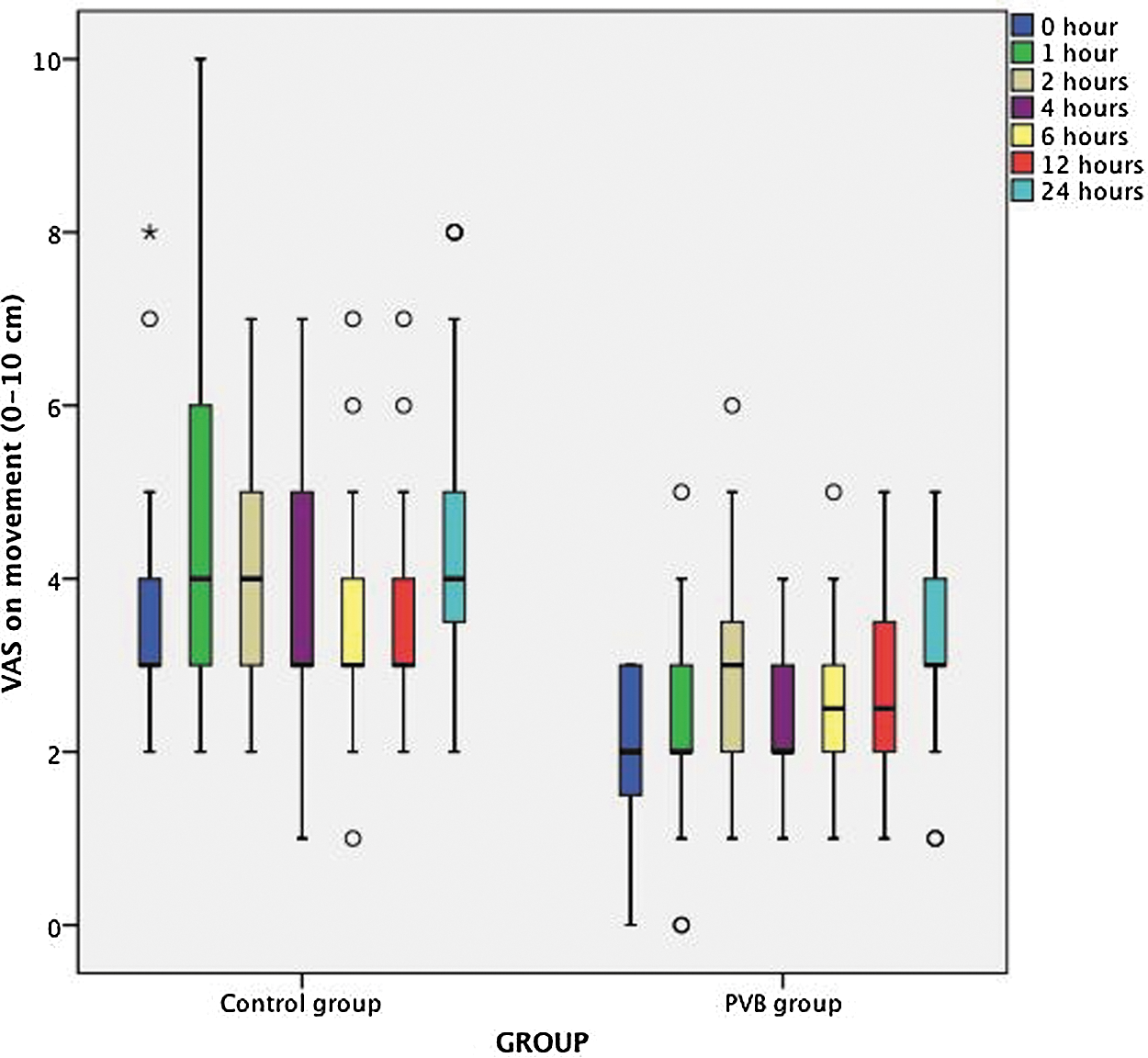
Comparison of visual analog scale (VAS) scores at movement (deep breathing) in the postoperative period. The median, interquartile range (box), and the 5th and 95th centiles are shown. The circles and asterisk represent patients lying outside the range. PVB=paravertebral.
The median time to first analgesic requirement after extubation was 30 (0–180) min in the control group and 120 (30–570) min in the PVB group. (P=0.0000)
Retrospectively, the median time from the administration of the PVB block to first analgesic requirement in the PVB group was 275 (180–610) min.
The average duration of stay in the PACU was comparable in the control (15.76 [±2.17] hours) and block group (14.69 [±2.00] hours) (P=0.079).
Postoperative PCA fentanyl consumption was significantly more in the control group (525 μg [150–1275]) than in the PVB group (175 μg [25–475]) (P=0.0000). Within the PVB group, PCA fentanyl consumption in patients with (150 μg [25–450]) or without (225 μg [25–450]) fluoroscopic confirmation of dye spread was comparable (P=0.482).
Three patients in the control group and none in the PVB group needed rescue morphine analgesia. Control group patients received more tramadol boluses (1.95±0.80) than the PVB group patients in the ward (1.04±0.53) (P=0.0000).
The majority of patients in both groups were free from PONV; one patient in each group needed ondansetron.
A fall in the PEFR was observed in both groups at 6 hours and 24 hours postoperatively. The difference between groups was not statistically significant (Fig. 3).
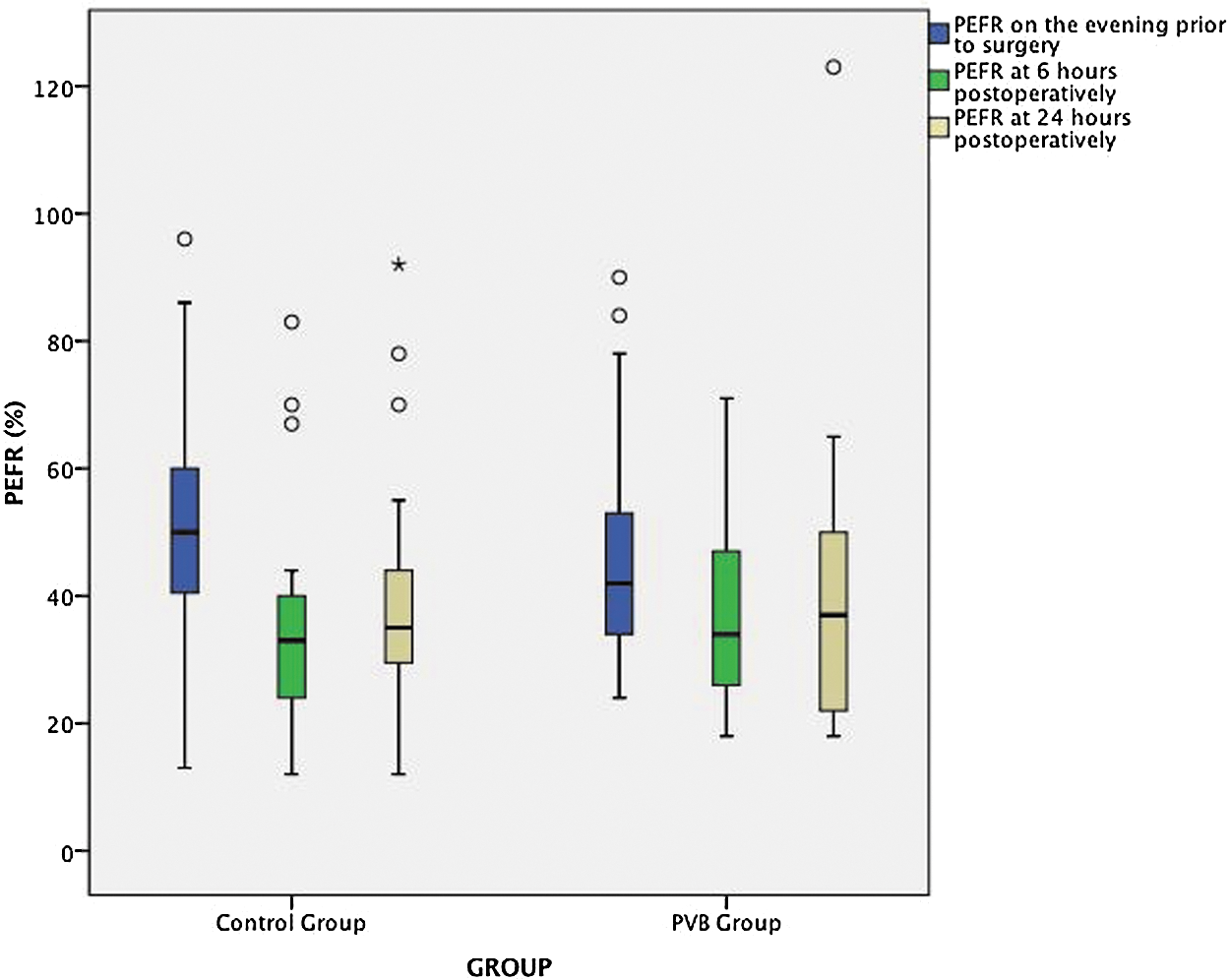
Comparison of pulmonary expiratory flow rates (PEFR) between the two groups. The median, interquartile range (box), and the 5th and 95th centiles are shown. The circles and asterisk represent patients lying outside the range. PVB=paravertebral.
The QoR score was higher in the PVB group (15.36±2.29) compared with the control group (13.46±2.13) (P=0.0039).
Discussion
The primary aim of the study was to assess the efficacy of PVB block for providing analgesia at rest in adults undergoing PCNL under general anaesthesia. The VAS scores at rest were significantly lower in the PVB group compared with the control group for the first 2 hours postoperatively (Fig. 1). The difference thereafter was not significant until 12 hours postoperatively. This could be because by 2 hours postoperatively, the effect of the initial PVB bolus had worn off and the control group patients had started receiving PCA fentanyl. The significantly higher consumption of PCA fentanyl by the control group during the PACU stay could have masked the difference in VAS scores until 12 hours postoperatively.
Similar results were observed by Ak and associates 10; patients in whom a one-time, multiple-level PVB block at thoracic T10–T12 levels was administered at the end of surgery had significantly lower VAS scores at rest for the first 2 hours postoperatively. Time to first analgesic requirement was also significantly longer in the block group (94.2±24.1 min) compared with the control group (48.3±17.4 min) similar to our study—120 (30–570) minutes PVB group and 30 (0–180) minutes control group. Unlike Ak and associates, 10 however, a single-level PVB block was performed before induction and a PVB catheter inserted in the present study.
The median time from the administration of the PVB block to the first analgesic requirement was 275 (180–610) minutes in our study, demonstrating that the analgesic effect of a bolus of local anesthetic has a limited duration.
This was also observed by Akin and associates, 10 where analgesia lasted for 8 hours after a single postoperative bolus of lumbar PVB local anaesthetic in elderly patients (>65 years) undergoing open urologic surgery. 13
Elbealy and colleagues 9 provided surgical anesthesia for PCNL by inserting a lumbar PVB (L1–2 level) catheter and administering titrated doses of 0.5% bupivacaine up to a maximum of 35 mL. The catheter was removed after the procedure, and PCA morphine started. Patients in the PVB group were found to have lower VAS scores and morphine requirement in 24 hours postoperatively compared with patients administered epidural or general anesthesia. In our study, general anesthesia was administered to all patients because they needed to be positioned prone and the PVB block was used for providing analgesia alone. The PVB catheter enabled us to readminister local anesthetic resulting in decreased postoperative analgesic (PCA fentanyl, morphine rescue, tramadol) requirement and lower VAS scores in the block group during the study period.
Unlike these studies 9,10,13 that only assessed pain at rest, we also assessed VAS scores on deep breathing (movement). This was significantly less in the PVB group at all time points studied. This is especially important, because nephrostomy tubes, especially with supracostal punctures, can causer considerable pain on deep breathing. 2 The use of small diameter nephrostomy tubes or their avoidance can minimize pain. 4 A recent meta-analysis, however, demonstrated that further multicentric randomized trials are needed before this becomes established practice, especially with supracostal punctures. 6
To objectively measure the patient's ability to breathe deeply in the postoperative period, we measured PEFR. Despite the significantly lower pain on deep breathing in the block group, no significant difference in PEFR values was observed between the two groups in the present study. In contrast, Ugras and coworkers 14 found that postoperative infiltration of 30 mL local anesthetic (0.2% ropivacaine) in the skin, nephrostomy tract, and renal puncture site in adults undergoing PCNL resulted in longer time to first analgesic requirement, lower VAS (6 h) score, and higher PEFR values at 2 and 6 hours postoperatively. The PEFR values, however, became comparable by 24 hours, and all patients had a single subcostal access, unlike our study where a significant number of patients underwent supracostal (21%–42%), and at times multiple punctures.
No complications other than blood in the catheter were observed in three PVB group patients in this study. Similar incidence of vascular puncture has been reported by others (8.3%, 6.8 %). 15,16
Luyet and colleagues 17 reported a 30% incidence of catheter misplacement after anatomic landmark guided PVB catheter insertion necessitating flouroscopic confirmation of dye spread through the catheters. Dye visualization could not be done in the initial eight patients because the dye was unavailable. Naja and associates 18 reported that drug spread covering more dermatomes occurs when longitudinal dye spread is observed on flouroscopy. This was observed in the majority of our patients (14/16). No evidence of misplaced catheters was observed in the small group studied nor were higher pain scores suggestive of catheter misplacement observed in the eight patients in whom the dye study could not be performed.
QoR was assessed by using a validated score consisting of nine variables, each graded (0, 1, 2), to a maximum score of 18—a higher score signifying better quality of recovery. 12 Patients in the PVB group had a higher QoR score (15.36±2.29) than those in the control group (13.46±2.13) P=0.0039, further highlighting the effectiveness of repeated PVB block.
A limitation of this study was that PVB group patients had catheters whereas the control group patients did not. Insertion of PVB catheters in the control group and administration of saline was considered unethical because it would have exposed these patients to an invasive procedure without expectation of any benefit. The fact that control group patients are often exposed to harm for the sole purpose of blinding has been highlighted in a review by McGuirk and coworkers. 19 The PVB catheters were taped to the back and not easily apparent in this study. To decrease bias in pain assessment, however, objective measurement of the PCA fentanyl consumption was considered in addition to VAS scores.
Conclusion
A preincisional, ipsilateral PVB block with catheter provided good perioperative analgesia together with an improved QoR and minimal adverse effects in adults undergoing PCNL under general anesthesia. Although the technique was associated with decreased pain on deep breathing, a significant difference in PEFR was not observed between the groups.
Footnotes
Acknowledgments
We would like to thank Dr. Kalaivani, MSc Biostatistics, Department of Biostatistics AIIMS, New Delhi, for helping us with the statistical analysis of our paper.
This report was previously presented, in part, at the 15th WFSA World Congress of Anaesthesiologists in 2012, and was published as an abstract in British Journal Anaesthesia.
Disclosure Statement
No competing financial interests exist.