
Abstract
Purpose:
To evaluate the efficacy and safety of monopolar (M-TURP) and bipolar (B-TURP) transurethral resection of the prostate in benign prostatic hypertrophy (BPH) patients.
Materials and Methods:
Eligible randomized controlled trials (RCTs) were identified from electronic databases without language restrictions. Database search, quality assessment, and data extraction were independently performed. The primary postoperative outcomes of topical M-TURP and B-TURP were maximum flow rate (Qmax) and/or International Prostate Symptom Score (IPSS). Safety was estimated by TUR syndrome; need for transfusion; clot retention; bladder neck contracture (BNC); urethral stricture (US); and catheter removal time. Efficacy and safety were investigated using the Review Manager.
Results:
Thirty-one trials met the inclusion criteria. Pooled analysis revealed significant difference in efficacy between the M-TURP and B-TURP groups. Safety analysis revealed significant improvement in the TUR syndrome with B-TURP than with M-TURP. Pooled analysis revealed that clot retention was significantly higher in M-TURP than in B-TURP. Moreover, pooled analysis revealed no significant difference between both groups in the blood transfusion frequency or late complications (urethral strictures) and bladder neck constriction.
Conclusions:
This systematic review indicates that B-TURP was significantly better in the result of Qmax and for decreasing the incidence of TUR syndrome and clot retention. No significant differences were observed in the nature of adverse events such as transfusions, retention after catheter removal, and urethral complications between both groups. Thus, B-TURP is the next generation “gold standard” for benign prostatic obstruction (BPO) because it is associated with a lower rate of clinically relevant complications such as TUR syndrome and clot retention.
Introduction
B
There are several therapeutic options to consider on the basis of the symptoms and complications of LUTS and BPO. These options include watchful waiting, pharmacological therapy, minimally invasive therapy, transurethral resection of the prostate (TURP), or open prostatectomy.
Monopolar TURP (M-TURP) is the surgical “gold standard” for BPO, primarily because of its well-documented long-term efficacy. 2 Although significant technical improvements over the past decades have decreased the adverse events associated with the procedure, concerns still remain regarding complications, such as the transurethral resection (TUR) syndrome, bleeding, and urethral strictures (US). 3,4 A prospective, large-scale, multicenter, observational study has revealed that although TURP mortality and morbidity have decreased (0.1%), morbidity still remains high (11.1%). 5
Incorporation of bipolar technology represents a significant technical improvement in TURP over recent years. Bipolar TURP (B-TURP) addresses a fundamental flaw of M-TURP because it can be performed in normal saline. The technique has revealed promising results. 6,7
A meta-analysis published in 2009 reported no clinically relevant differences in short-term efficacy between the two techniques, although B-TURP was preferred because of its more favorable safety profile (lower TUR syndrome and clot retention rates) and shorter duration of irrigation and catheterization. However, the meta-analysis also indicated a lack of well-designed, multicenter, and international randomized, controlled trials (RCTs) with long-term follow-up and cost analysis of the B-TURP technique. 8 In recent years (2009–2013), a number of new RCTs, including multicenter and international studies, have been published. 9 –22 Therefore, it is necessary to conduct a new systematic review and meta-analysis of RCTs that assesses the efficacy and safety (primary outcomes) of M-TURP and B-TURP in patients with BPO.
Material and Methods
Systematic search strategy
We searched the following databases: Medline, Embase, Science Citation Index, and the Cochrane Library. There was no restriction on the language of the publications. The following search terms were used to identify any relevant studies: “benign prostatic hyperplasia or BPH,” “BPH-related obstruction or BPO,” “monopolar-TURP and/or bipolar-TURP,” and “randomized controlled trial.” The data collected was published up to July 1, 2013.
Identification of articles
The following criteria were used for study selection: (1) RCT, (2) patients diagnosed with benign prostatic hyperplasia or BPO, (3) treatment intervention, M-TURP vs B-TURP, and (4) one of the primary outcomes must be clearly defined. Studies were excluded for the following reasons: (1) they were not RCTs, (2) primary outcomes were not mentioned, or (3) comparison was between B-TUVP and B-TURP (hybrid technique).
Outcomes
The outcomes include efficacy and safety. Efficacy was estimated by the postoperative maximum flow rate (Qmax) and/or International Prostate Symptom Score (IPSS). Safety was assessed by the postoperative occurrence of at least one of the following: (1) TUR syndrome, (2) need for transfusion, (3) clot retention, (4) bladder neck contracture (BNC), (5) US occurrence, and (6) the time of catheter removal. 8
Quality assessment of the included studies
Each step of the data extraction was independently undertaken by two reviewers and then cross-checked. Any disagreements that could not be reconciled by discussion were considered by a third person. The quality of the trials included in the study was assessed using the Jadad scale score from 0 to 5 points, with a score of 3 or above indicating high quality. 23
Data synthesis and analysis
The trial data were processed as described in the Cochrane Reviewers' handbook. 24 The statistical analyses were performed using the Review Manager 5.2 (Cochrane Collaboration, Oxford, UK). The χ 2 and I 2 tests were used to assess heterogeneity of the study data. If χ 2 heterogeneity was reported as P>0.10 and I 2 ≤50%, heterogeneity was classified as low. A fixed effect was used for the calculations in the absence of any evidence of heterogeneity; otherwise, a random effects model was applied. We reported the risk ratio (RR) for dichotomous data and weighted mean differences (WMD) for continuous data, accompanied by 95% confidence intervals (CI). A P value <0.05 was considered statistically significant.
Results
Study characteristics
The combined search strategies identified 31 trials 9 –22,25 –40 that included 3,669 patients who met the inclusion criteria. All the studies were RCTs, and almost all were reported in English, except for one in Korean 32 and one in Chinese. 35 Two studies 27,28 enrolled the same type of patients but reported different follow-up times, whereas two other studies belonged to the same group of patients with similar follow-up time but focused on different outcomes. 17,41 Further, 16 studies 9,10,12,14,20,21,25,27 –32,34,36,40 used the plasma kinetic technology, and three studies 15,26,35 used the Vista CTR (Vista Coblation controlled tissue resection) technology. The remaining studies 11,13 –19,22,33,37 –39 used the TURis (transurethral resection in saline) technology. The characteristics of the studies are summarized in Table 1.
=Significant difference between monopolar and bipolar transurethral resection arms.
=Mean age.
IPSS=International Prostate Symptom Score; M/B=M-TURP/B-TURP; n/a=not available; PK=plasma kinetic technology; PVR=postvoid residual urine volume; Qmax=maximum flow rate; RCT=randomized, controlled trial; TURis=transurethral resection in saline; Vista CTR=Vista Coblation controlled tissue resection.
Efficacy
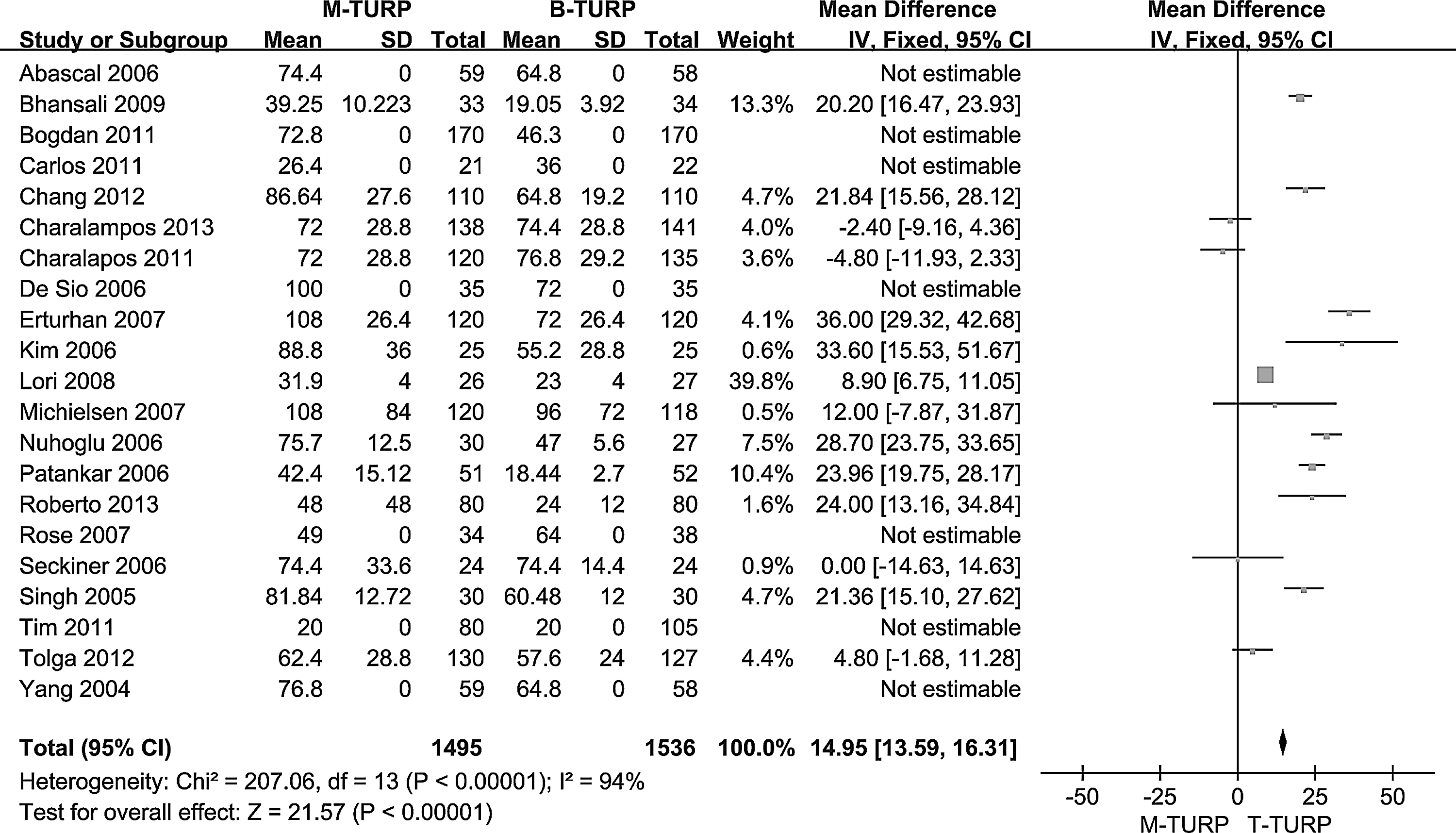
Fifteen studies 9 –11,13,14,16,19,20,27,29,30,35 –37,40 that included 2,056 patients were quantitatively analyzed for the outcome of Qmax after 12-month follow-up (23 studies from 1 to 60 months). Pooled analysis revealed that M-TURP and B-TURP technology revealed a significant difference in Qmax (Fig. 1; random effects model, mean difference, −0.36; 95% CI, −0.82 to −0.09; P=0.12). The studies by Erturhan et al. 36 revealed that this difference was not clinically relevant and may have been considerably influenced by other factors. Short-term data (6 months, 32 1 month, 39 and 6 months 40 ) and long-term data (48 months 13 and 60 months 31 ) indicated that both techniques were equally effective. Trials that could be pooled for IPSS revealed no difference at 12 months. We concluded that current evidence revealed clinically relevant differences between M-TURP and B-TURP in Qmax.
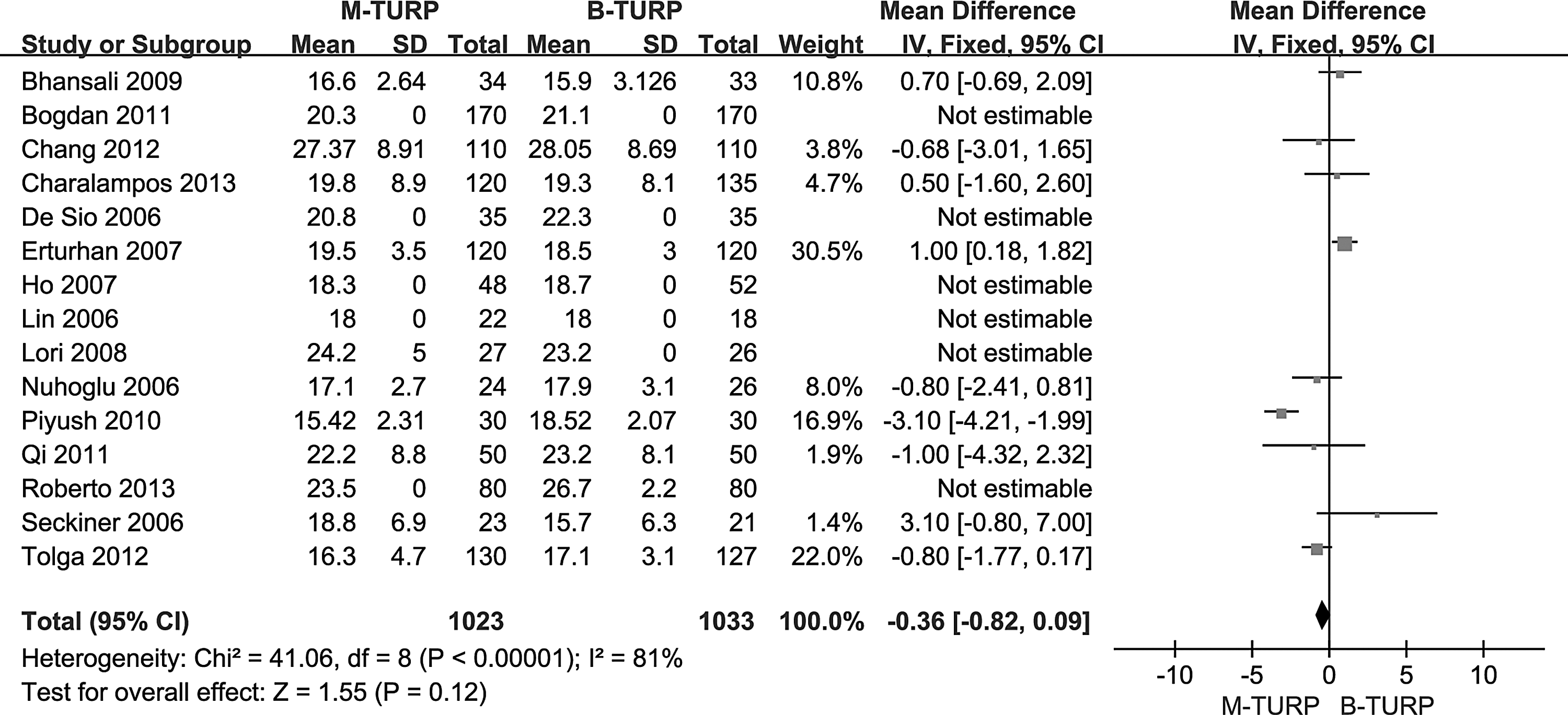
Qmax at 12-month follow-up: M-TURP vs B-TURP.
Safety
Transurethral resection syndrome
Because a conductive medium is used instead of the conventional nonconductive irrigation fluid, the bipolar technology has decreased TUR syndrome incidence during recent decades. This is an important advantage because all issues relating to hypotonic/hyposmolar fluid irrigation (dilutional hyponatremia, TUR syndrome) have been eliminated. 42
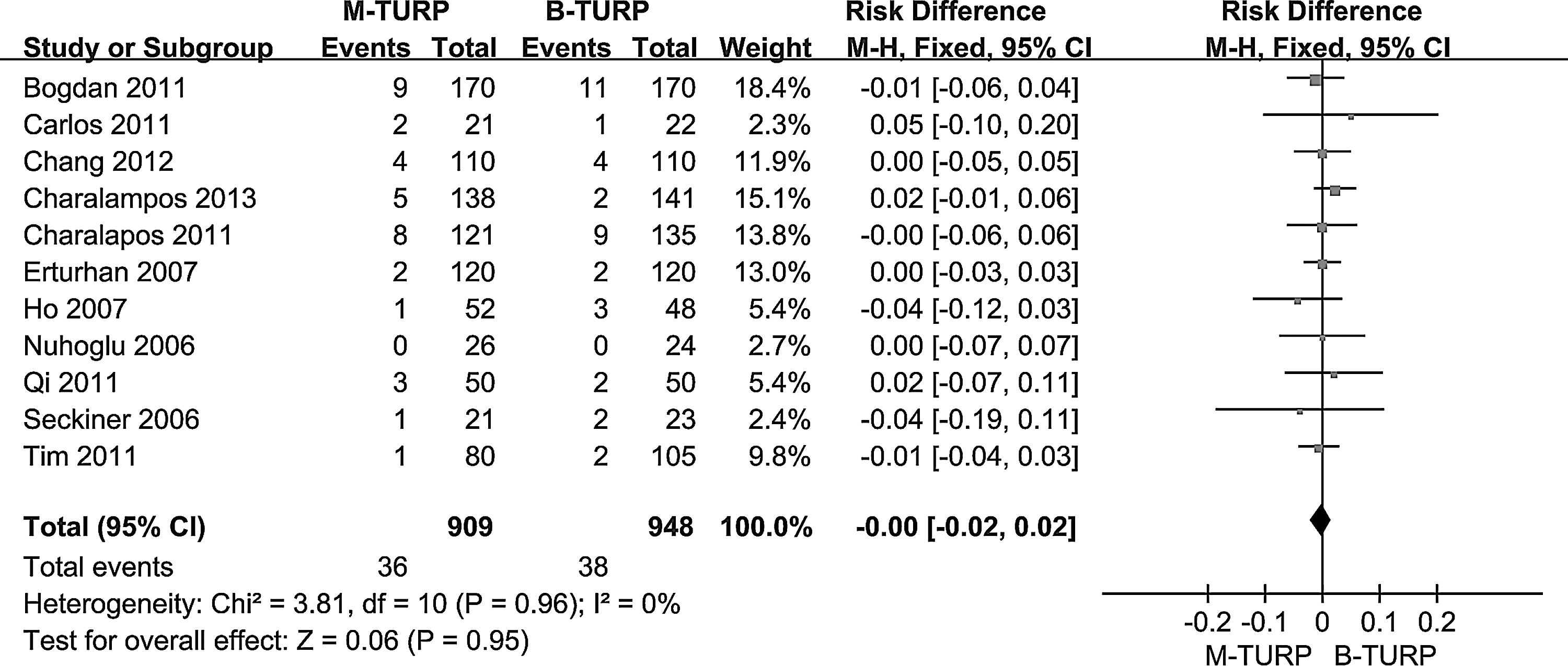
Twenty-four studies 9,10,13 –16,18,19,21,22,25 –27,29 –34,36 –40 investigated transurethral resection for TUR syndrome (Fig. 2; risk difference 0.02; 95% CI, 0.01–0.03; P=0.0004). Individual trials reported no significant difference between the two arms, whereas pooled analysis detected a significant difference (risk difference 0.02; 95% CI, 1%–3%; P=0.0004). This indicates that a smaller proportion of patients treated using B-TURP develop the TUR syndrome compared with those treated using M-TURP.B-TURP cannot prevent fluid absorption, however, and this fact should always be kept in mind.
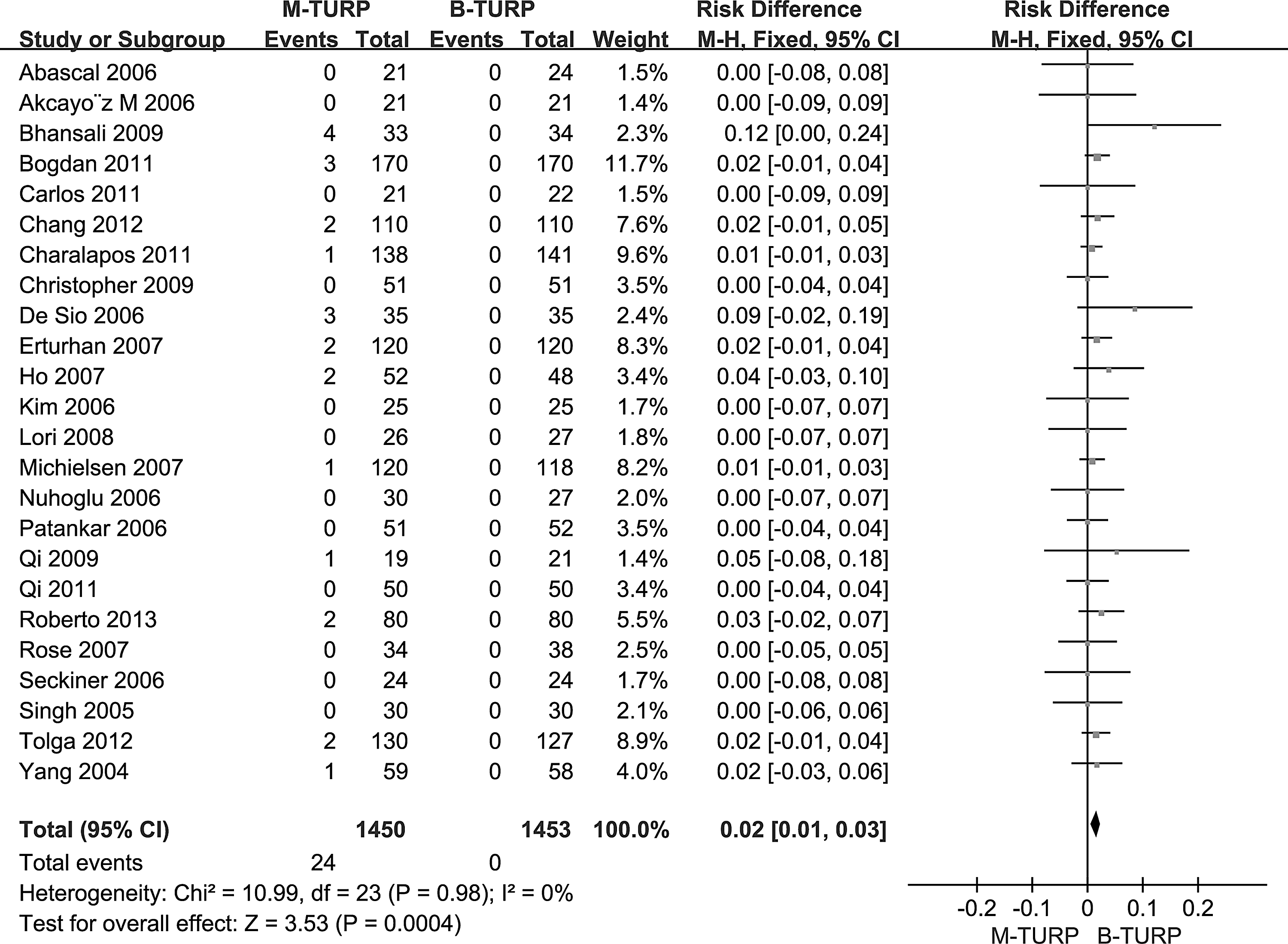
TUR syndrome: M-TURP vs B-TURP.
Incidence of clot retention and blood transfusion
Intraoperative or perioperative bleeding is a major complication in TURP and can cause significant clinical symptoms such as clot retention or requirement for blood transfusion. The transfusion rates in M-TURP series have significantly decreased over time, although the incidence of clot retention ranges between 2% and 5% and still remains a concern. 3
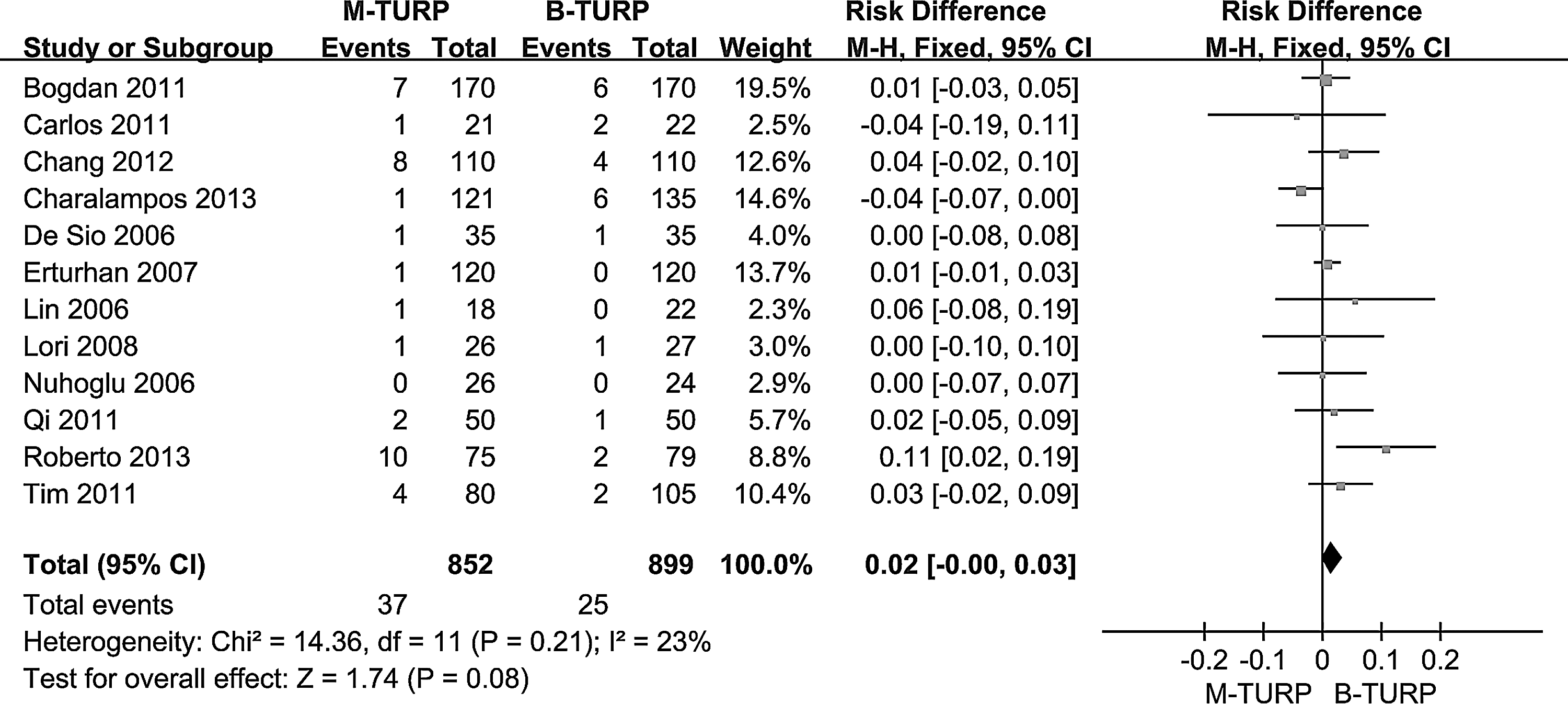
Thirteen studies 10,12 –14,16,19,27,31,35 –37,39,40 evaluated the incidence of clot retention, and 22 studies 9,10,13 –20,22,25 –27,29,31,33,34,36,37,39,40 evaluated the cases requiring blood transfusion. Pooled analysis (Fig. 3) revealed that the incidence of clot retention was significantly higher in M-TURP than in B-TURP (risk difference 0.04; 95% CI, 0.02–0.06; P<0.0001). In addition, pooled analysis (Fig. 4) verified that there was no significant difference between M-TURP and B-TURP regarding the frequency of blood transfusions (risk difference 0.02; 95% CI, 0.01–0.04; P=0.0005).
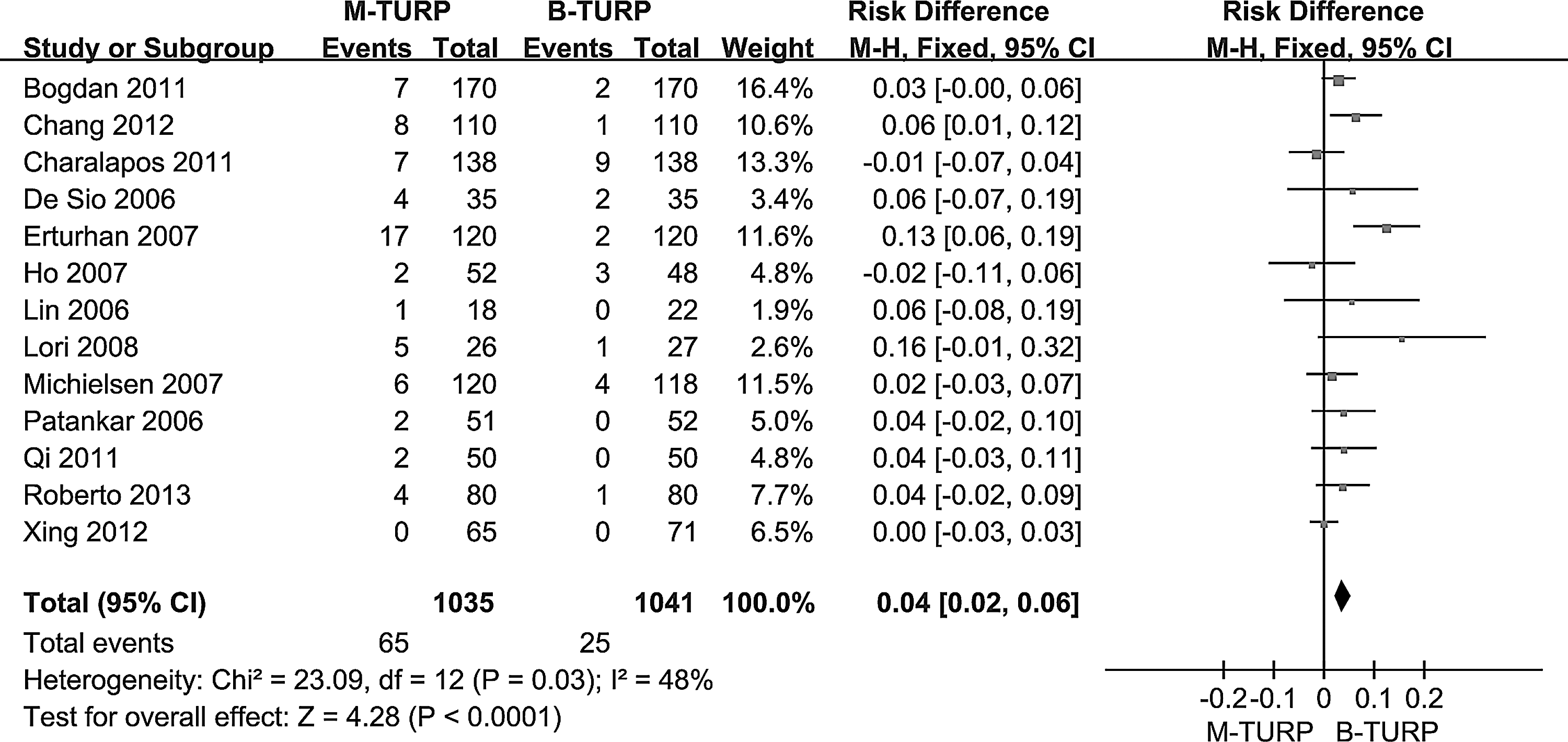
Incidence of clot retention: M-TURP vs B-TURP.
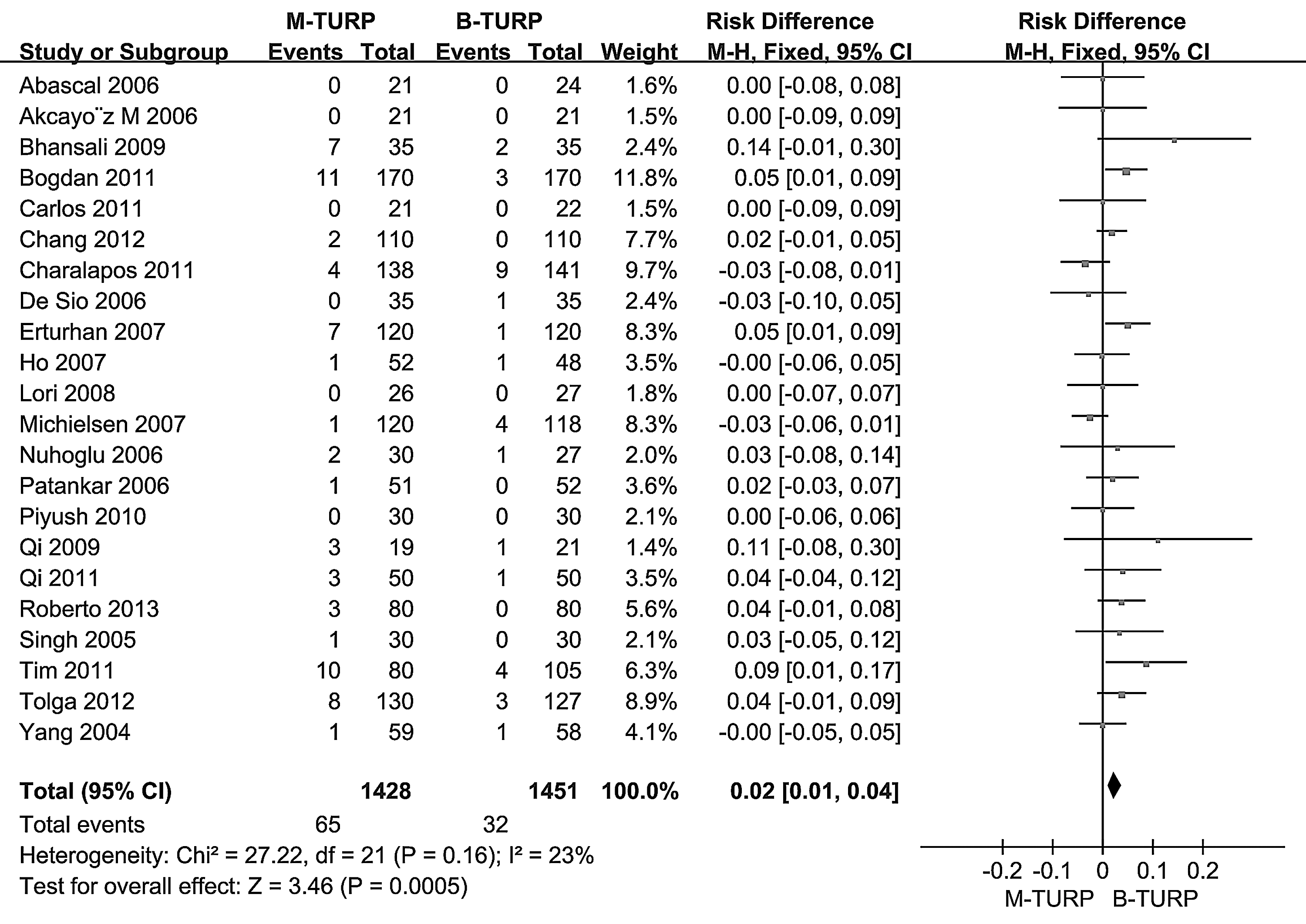
Blood transfusion: M-TURP vs B-TURP.
Catheterization time
A meta-analysis could not be performed because of extreme heterogeneity (I 2 : 94%; see Fig. 5. Twenty-one studies 9 –11,13 –18,25 –27,29 –33,36,38 –40 analyzed catheterization time. The different protocols caused heterogeneity for catheter removal.
Catheterization time: M-TURP vs B-TURP.
Late Complications
Urethral stricture (US) and bladder neck constriction (BNC) were the major late complications of TURP. Pooled analysis (Figs. 6 and 7) revealed no significant difference in the late complications between M-TURP and B-TURP. However, B-TURP occasionally presented a higher incidence of US and BNC compared with M-TURP in individual RCTs (US, 22, 33; BNC, 28). The risk factors for B-TURP included a larger resectoscope diameter, higher ablative energy, and longer procedure time.
Urethral strictures: M-TURP vs B-TURP.
Bladder neck constriction: M-TURP vs B-TURP.
Bias analyses
To analyze possible publication bias, we used funnel plots to evaluate the comparisons of outcomes. The funnel plot for TUR syndrome shown in Figure 8 has no obvious asymmetry.
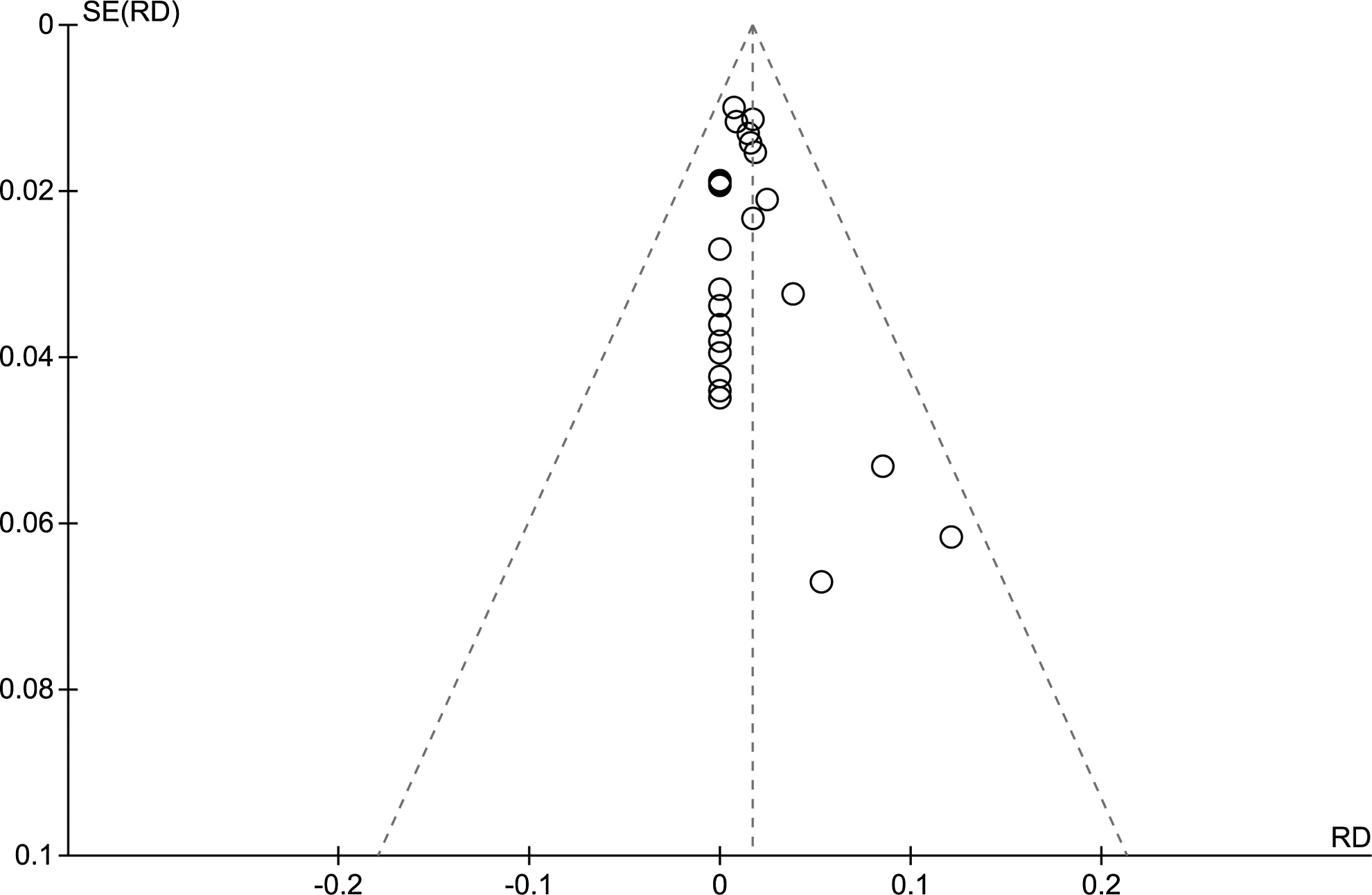
Funnel plot on the incidence of TUR syndrome.
Discussion
Over the past few decades, the traditional M-TURP has remained the gold standard surgical treatment for BPO. In recent years, however, bipolar technology, in which the positive and negative poles are on the same axis and isolated from each other by a ceramic connecting piece, has developed. 43 The absence of a return current has improved hemostasis during resection and minimized blood loss. 44 The hemostatic capability of B-TURP may be better than M-TURP because the mean coagulation depth in B-TURP is greater than the maximum microvessel diameter. 45 Bipolar technology can coagulate small venous bleeding and provides a clearer view compared with M-TURP during surgery, thereby resulting in a decrease in operation time as well as in the incidence of early complications. M-TURP is performed using glycine or mannitol irrigating solutions that may cause TUR syndrome, which is one of the most important complications of this surgery. In contrast, B-TURP uses normal saline during resection, which protects against TUR syndrome.
Pooled analysis for TUR syndrome has revealed that B-TURP was associated with significant improvement compared with M-TURP, with 24 patients developing TUR syndrome with M-TURP and none with B-TURP. These outcomes were due to the decreased serum sodium (Na+) levels. Therefore, B-TURP has a major advantage because it decreases the risk of TUR syndrome and is safer for patients, as the surgery is better controlled. Additionally, the training time for the resident is decreased with this procedure.
Furthermore, the incidence of clot retention was significantly higher in M-TURP than in B-TURP, resulting in B-TURP requiring less postoperative intervention and a higher degree of patient satisfaction. Hospitalization time and duration of catheterization, however, were similar with both technologies. Despite the advantage of B-TURP with regard to coagulation and incidence of clot retention, the transfusion rates in the two technologies were almost the same.
BPH primarily affects aging males. In elderly patients, the incidence of patients with previous medical history, including diabetes mellitus and cardiac pacemaker implantation history, is higher than usual. The use of normal saline decreased the risk of hyperglycemia in patients with diabetes, whereas the absence of a return current through the body in the bipolar technology has fewer effects in patients with a cardiac pacemaker.
In summary, this systematic review contains the largest patient group and the longest follow-up comparison between the two surgical procedures M-TURP and B-TURP. The findings confirm that B-TURP is more effective in the treatment of BPH. This review also confirms that B-TURP remarkably increases Qmax due to the shorter operation time, better surgeons' comfort as a result of lower complication rates, better coagulation, and better surgical exposure. B-TURP also decreases the incidence of TUR syndrome and the risk of clot retention, and the bipolar technology is safer for patients with diabetes mellitus and cardiac pacemakers. In addition, B-TURP decreased the training time for students and promotes patient satisfaction. When these factors of safety, satisfaction, and training time are taken into account, it is apparent that B-TURP should replace M-TURP as a treatment option for BPH.
Conclusions
This systematic review reveals that there are clinically relevant differences with regard to safety and efficacy between M-TURP and B-TURP in Qmax. B-TURP is associated with decreased incidence of TUR syndrome and decreased risk of clot retention compared with M-TURP. The bipolar technique is safer for patients with diabetes mellitus and cardiac pacemakers, requires shorter training time for the students, and promotes higher patient satisfaction. In addition, because of comparable complication rates regarding TUR syndrome, the B-TURP is a cheaper and less invasive method for surgical management of BPH. We consider that B-TURP is the next generation “gold standard” for BPO.
Footnotes
Acknowledgments
This study was supported by the National Natural Science Foundation of China (Grant Nos. 30901484, 81270841) and the Pillar Program from Science and Technology Department of Sichuan Province (Grant No. 2013SZ0034).
Disclosure Statement
No competing financial interests exist.