
Abstract
Purpose:
To evaluate the safety and efficacy of retrograde placement of single-J stent guided by a flexible cystoscope for management of ureteroenteral anastomotic stricture in patients after radical cystectomy and Bricker urinary diversion.
Patients and Methods:
Between January 2008 and June 2012, 11 patients with ureteroenteral anastomotic stricture after open radical cystectomy and Bricker urinary diversion were enrolled in this study. All patients were treated with retrograde placement of single-J stent guided by a flexible cystoscope. A 7F single-J stent was placed for 6 weeks.
Results:
Of the 11 patients, seven strictures occurred on the left side, two on the right side, and two on both sides. The retrograde procedure was successfully performed in 10 cases, and the remaining 1 was successful on the right side but failed on the left side. Upper urinary tract infection was well controlled in all three patients with fever. After a follow-up of 12 to 66 months, eight patients had long-term symptom relief, one patient had open surgery to remove the stricture and re-implant the ureter, and one patient died because of tumor recurrence. The only failed case was that of a left side percutaneous nephrostomy, but the patient was lost to follow-up.
Conclusions:
Retrograde placement of a single-J ureteral stent guided by a flexible cystoscope is safe and effective for ureteroenteral anastomotic stricture in patients with Bricker urinary diversion, and it brings fewer complications. The procedure is minimally invasive and could avoid immediate surgery for most patients.
Introduction
B
Ileal conduit (Bricker procedure) is the most common form of ureteroenteral anastomosis and has become the gold standard in urinary diversion since the1950s. 8 Ureteroenteral anastomotic stricture after the Bricker procedure is very common, however, 7,9 and another procedure is often needed to preserve renal function and prevent other complications such as severe upper urinary tract infection. Many procedures including open surgery and anterograde ureteroscopy after percutaneous nephrolithotomy have been reported. These procedures are challenging and not widely applied for their limitations. 8
In this study, we performed retrograde placement of single-J stent guided by a flexible cystoscope for management of ureteroenteral anastomotic stricture in patients after radical cystectomy and Bricker urinary diversion. We evaluated the efficacy and safety of this procedure to see if it can be a noninvasive alternative to manage ureteroenteral anastomotic stricture.
Patients and Methods
This retrospective study was approved by the Institutional Review Board of Shanghai Changhai Hospital. We reviewed medical files for patients with bladder cancer who underwent open radical cystectomy between January 2008 and June 2012. End-to-side ureteroenteral anastomosis was established, and interrupted sutures were performed. After a patient came to the clinic, ultrasonography was first prescribed. Then, intravenous urography, CT or MRI was performed to identify the location and length of the stricture. Computed tomography urography (CTU) with contrast medium was performed when renal function of the patient was normal; magnetic resonance urography (MRU) was performed when the creatinine level was high. A loopagram was performed, and reflux was excluded. Urine culture and drug sensitivity tests were performed before operations.
Prophylactic antibiotics were administered according to results of urine culture and drug sensitivity tests. When there was fever, quinolone was used before the urine culture and sensitivity test. After surgery, the patients received intravenous antibiotics until results of the complete blood cell count and temperature was normal. Then, ciprofloxacin was given orally for 3 days. Anesthesia and sedation were combined for these patients. In this study, when cardiopulmonary function was normal, general anesthesia was applied; when cardiopulmonary function was compromised, spinal anesthesia was performed.
Retrograde placement of the single-J stent guided by a flexible cystoscope was then performed. The flexible cystoscope (16.2F, Olympus, Tokyo, Japan) was first inserted into the ileal conduit. The assistant should then gently pinch the stoma nipple to control the outflow rate so as to achieve a moderate conduit filling and a clear vision. Zebra guidewire (Cook, Bloomington, IN) was inserted into the strictured ureter through the anatomosis and fixed beyond the site of obstruction. Then, 5F, 6F, 7F, and 8F ureteral stents (Shagong, Zhangjiagang, Jiangsu, China) were used successively to dilate the ureteral stricture with the guidance of the guidewire. For two patients who could afford the expense of balloon dilation (Cook, Bloomington, IN), this procedure was applied with a pressure of 12 to 14 atmospheres for 5 minutes. Finally, a 7F single-J stent was placed and left in place for 6 weeks for all patients.
Biopsies were performed if an abnormal mass could be observed. Antibiotics were administered after the procedure. Blood loss was estimated by both the surgeon and anesthesiologist. Pain was assessed 1, 3, 6, 12, 18, and 24 hours after the operation. Operative time, bleeding volume, maximum visual analogue scale (VAS) scores at different time points and hospital stay were documented and analyzed. Patients were followed every 3 months in the first 2 years with urine analysis and ultrasonography, and then they were followed once every 6 months. Intravenous urography was performed once a year. When periodic replacement of the stent was needed, it was performed every 3 months in the clinic under cystoscopy guidance.
Results
Between January 2008 and June 2012, 138 patients with bladder cancer underwent open radical cystectomy and Bricker urinary diversion by a single urologist. Among them, 11 (8%) patients with 13 strictures had a diagnosis of ureteroenteral anastomotic stricture after the operation (Table 1). The incidence rate of the stricture was 7.97%. Neither adjuvant nor neoadjuvant systemic chemotherapy was performed in these patients. They came to the hospital with a complaint of flank pain (eight patients) or flank pain with fever (three patients) after a median of 6 months (range 3–10 months) postoperatively. The median age of the patients was 61 years (range 41–76 years). Nine patients were men, and two were women. Of the 11 cases, 7 were left sided, 2 were right sided, and 2 were on both sides.
The mean VAS pain score before the procedure was 3.9±1.0. The average operative time was 23.9±3.6 minutes. The average hospital stay was 30.0±8.5 hours. The mean maximum VAS pain score was 2.3±0.9. The mean VAS score was decreased significantly (P=0.008). No postoperative analgesic was administrated. Intraoperative bleeding was less than 10 mL. In 10 patients, retrograde placement of a single-J stent was successful, and flank pain was relieved. In 1 of the 10 patients, a cauliflower-like neoplasm was observed close to the right ureteroenteral anastomosis (Fig. 1). Pathologic results after biopsy indicated recurrent bladder cancer. Percutaneous nephrostomy was finally performed because the tumor progressed quickly and wrapped the right iliac vessels. The patient died 8 months after percutaneous nephrostomy.
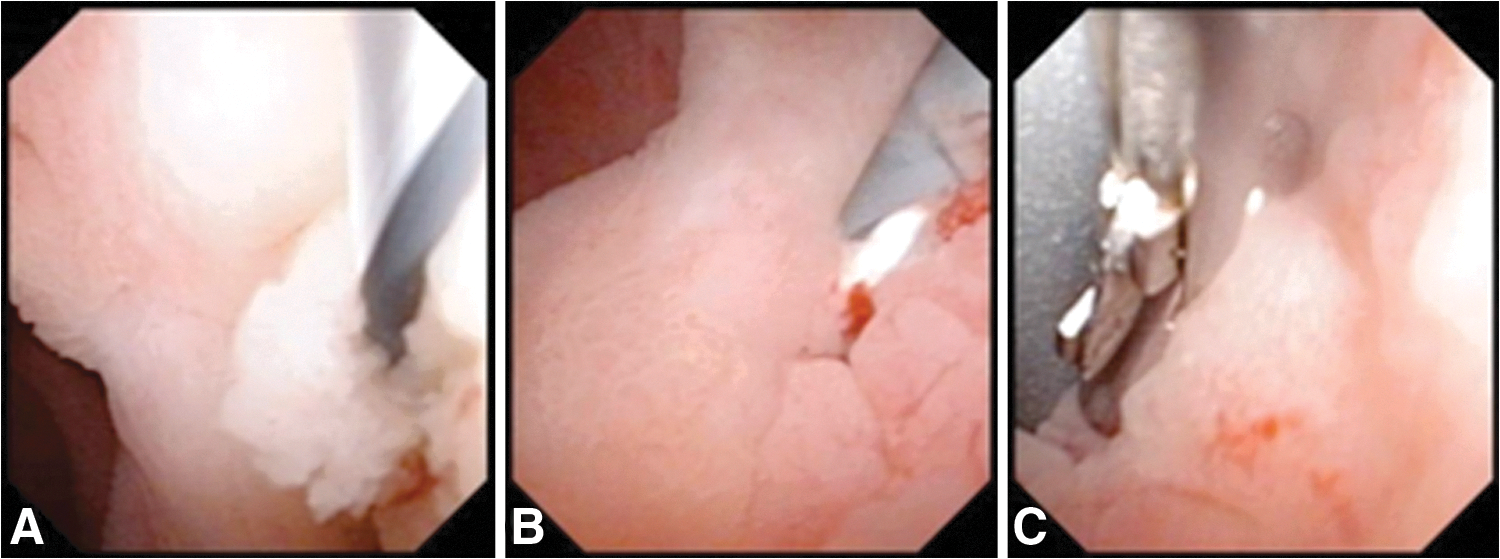
Bladder cancer recurrence near the right ureteroenteral anastomosis. (
Among the other nine patients who were followed for 12 to 66 months, five patients were symptom free, and upper urinary tract dilatation disappeared 6 weeks after the procedure (Figs. 2, 3); symptoms and hydronephrosis did not recur after removing the single-J stent during follow-up. Two patients presented upper urinary tract dilatation 4 weeks after stent removal. The single-J stent was replaced every 3 months, and the dilatation finally vanished after 6 months. Another patient got a regular single-J stent replacement every 3 months. For the last patient, resection of the stricture and ureteral reimplantation were performed as an open procedure because he refused periodic replacement of the single-J stent.
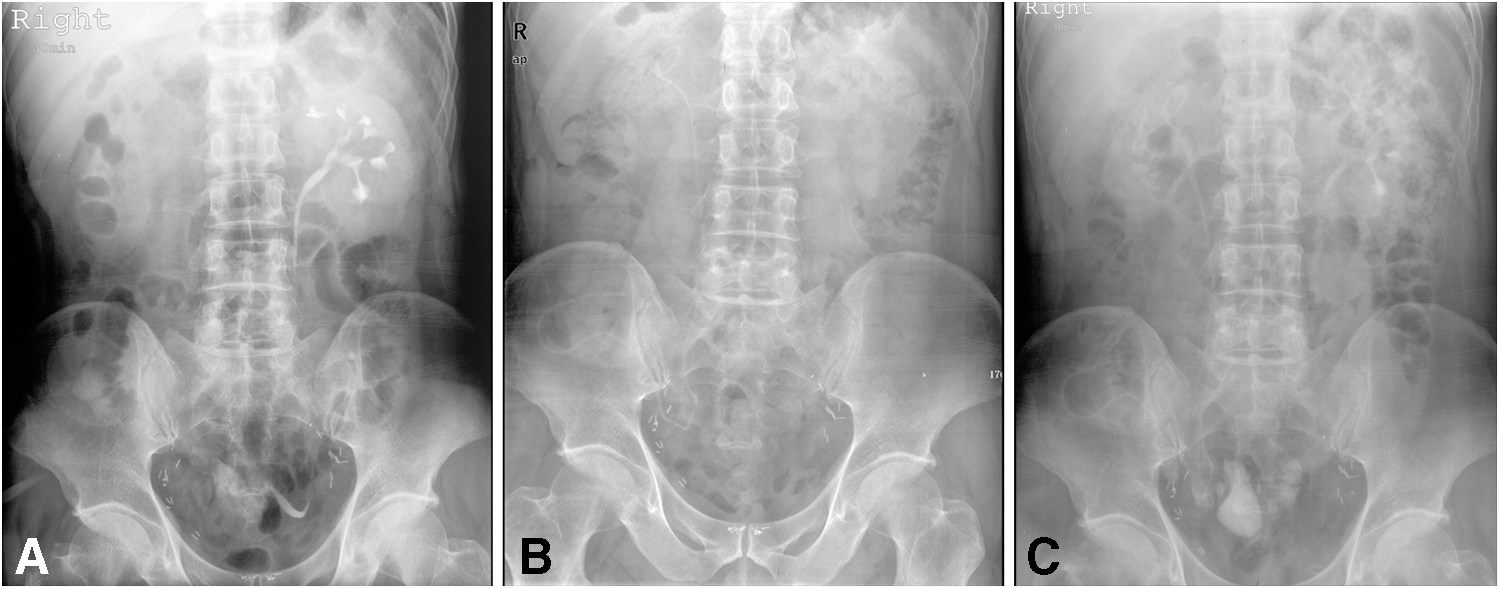
Efficacy of retrograde placement of a single-J stent (kidneys, ureters, and bladder [KUB] radiography+intravenous urography [IVU]). (
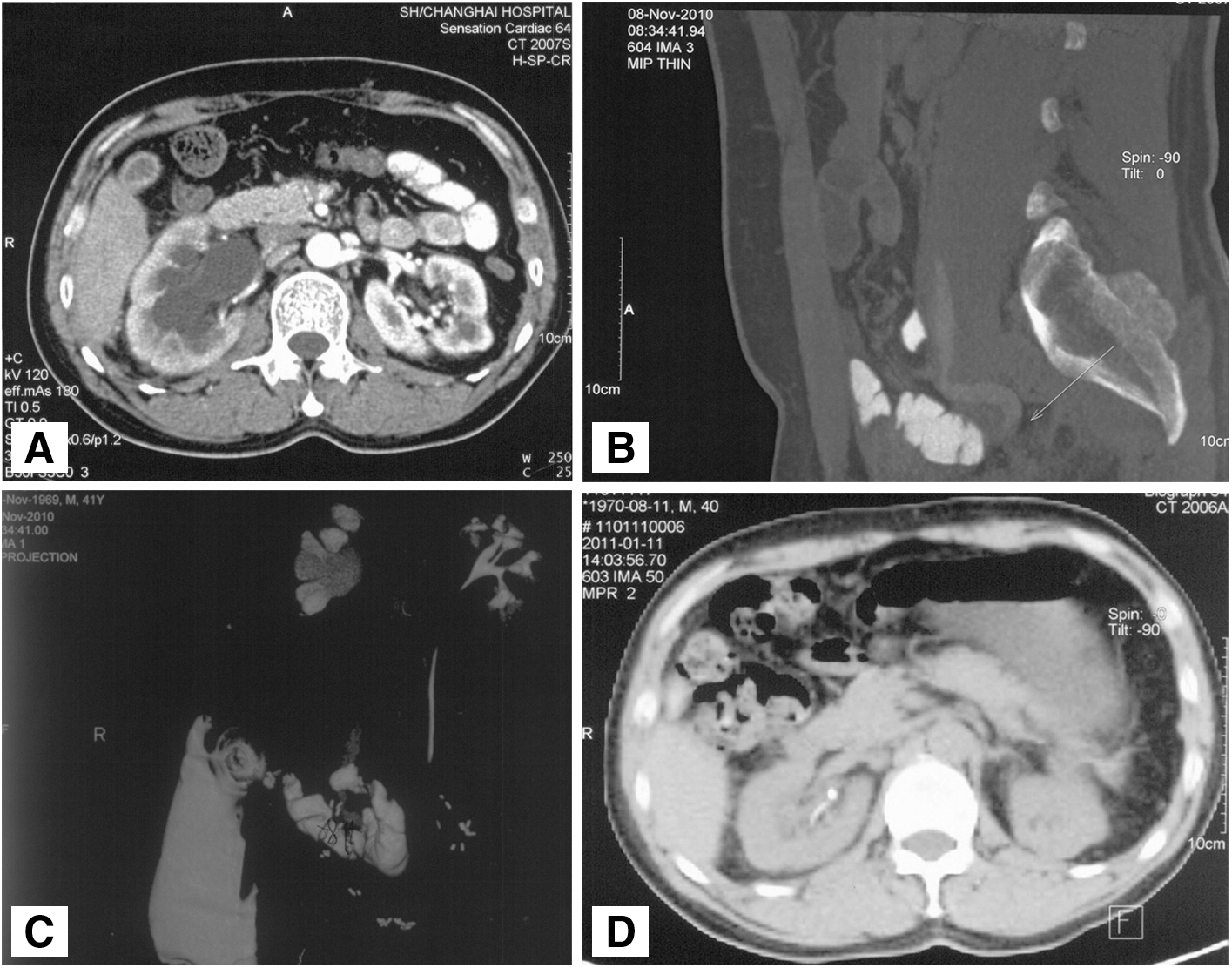
Efficacy of retrograde placement of a single-J stent (computed tomography urography [CTU]+magnetic resonance urography [MRU]). (
Balloon dilation was performed in two patients. Both patients were symptom free 6 weeks after the procedure (Supplementary Figs. 1, 2; Supplementary Data are available online at
Discussion
The Bricker procedure is one of the most common ways of urinary diversion after cystectomy. Sufficient blood supply is the key to prevent ureteroenteral anastomotic stricture. Ischemia or necrosis of the distal ureter happens, however, because lower ureters are greatly mobilized during the surgical procedure, leading to ureteroenteral anastomotic stricture. 7,9 –11 Studies have shown that the incidence rate of ureteroenteral anastomotic stricture 2 years after Bricker diversion could be as high as 14%. 7 If not managed properly, it may easily cause upper urinary tract infection, urolithiasis, renal insufficiency, and more. 12 –14 Therefore, appropriate management is of great importance.
There are currently several ways to manage ureteroenteral anastomotic stricture after radical cystectomy and Bricker diversion, including open surgery, anterograde ureteroscopy, and rigid cystoscopy. 15,16 Although the stricture could be resected through an open procedure, frequent adhesions are inevitable, and anatomic landmarks are illegible because of the previous cystectomy. Moreover, open surgical procedures could bring about additional trauma.
Anterograde ureteroscopy and placement of a single-J stent seems to be another option, but it necessitates a tract established by percutaneous nephrolithotomy, which is invasive. In addition, it may be accompanied by pertinent complications such as renal vascular injury. Bleeding may also occur during and after the procedure. 17 Some physicians have tried to use a rigid cystoscope to find the stricture. Because an ileal conduit differs from the normal urinary bladder in morphology and anatomic location, it might be difficult for a rigid cystoscope to find the stricture, however. Liatsikos and associates 18 used self-expandable metal stents for ureteroileal anastomotic strictures; however, this necessitates nephrostomy.
Endourologic treatment is promising to manage ureteroenteral anastomotic strictures. Schöndorf and colleagues 19 compared endourologic and open surgical procedures. They found the success rate of endourologic intervention was acceptable for ureteroileal strictures 1 cm or less. In this study, retrograde placement of a single-J stent guided by a flexible cystoscope for management of ureteroenteral anastomotic stricture was evaluated, and similar efficacy with more safety could be found when comparing with other treatments. 20,21 Advantages and essential points for this procedure are summarized.
There are several advantages to managing ureteroenteral anastomotic stricture with flexible cystoscope endoscopy. (1) The procedure is minimally invasive, relatively safe, and could be repeated. (2) There is no need to change position when treating bilateral diseases. (3) Retrograde cystoscopic inspection could be achieved through the conduit. Abnormalities that could not be easily discovered by CT or MRI could be found under direct vision. (4) Stricture could be preliminarily evaluated in the endoscopic vision and re-evaluated according to the grossly feculent urine flow rate when the guidewire passes through the stricture.
There are some tips that we should pay attention to while doing this procedure. (1) It is important to keep moderate conduit filling to ensure a good inspection vision. The conduit cavity is relatively small, however, and the irrigation fluid could outflow easily through the conduit outlet. According to our initial experience, the assistant could gently pinch the stoma nipple to control the outflow rate so as to achieve a moderate filling and a clear vision. (2) The conduit might be distorted beneath the abdominal wall. False passage and even perforation may happen if the cystoscope is inserted forcibly without a clear vision. Therefore, irrigation pressure and flow rate should be increased to ensure a smooth insertion under this circumstance.
(3) The dead end of the conduit should be taken as an anatomic landmark. Withdraw the flexible cystoscope from the dead end, then right and left ureteroenteral anastomoses could be observed successively to avoid confusion. (4) Morphologic change of the mucosa is an important mark to identify anastomosis. Microvilli and other structures of ileum glandular epithelium in the conduit will be gradually undermined after surgery, the epithelium will undergo urothelial metaplasia and eventually have coverage and protective functions similar to urothelium. 22 Urothelial metaplasia is most obvious around the anastomosis, so there is a marked contrast of the epithelium between the anastomosis and around, which is beneficial to find the anastomosis.
(5) If stricture recurred after removal of the stent, the placement of the stent could be prolonged to 3 months. Regular follow-ups and replacement of the stent are suggested. (6) Balloon dilation to expand the tract is highly recommended if patients could afford the expense. (7) The surgeon who performed the radical cystectomy may be the ideal one to solve this complication, because it may be easier for him or her to find the ureteroenteral anastomosis.
The efficacy of retrograde placement of a single-J stent guided by a flexible cystoscope for management of ureteroenteral anastomotic stricture in patients after radical cystectomy and Bricker urinary diversion is related to several factors. In our study, symptom free after the procedure were achieved in five patients who came to clinic immediately once flank pain occurred, indicating early intervention may be helpful. The intraoperative protection of nutrient arteries of ureters is important. In two cases, the procedure was not effective enough, and excessive mobilization of the ureter was found in these two cases when we reviewed the surgical records of cystectomy.
There were some limitations in this study. First, this was a single-center study, and the sample size was not large enough. Second, because of the small amount of patients with ureteroenteral anastomotic stricture, it was difficult to identify the population who are more likely to be successful with this procedure. Third, it is possible that only selected cases of stricture are amenable to this approach; passive dilation with stent upsizing over time does not work for every patient. It is nice for the patients who have been successfully dilated for a long time, however.
Conclusion
Retrograde placement of a single-J stent guided by a flexible cystoscope for management of ureteroenteral anastomotic stricture in patients after radical cystectomy and Bricker urinary diversion is minimally invasive, relatively safe, and effective according to our initial clinical practice. Long term, large-scale studies should be warranted to further evaluate this procedure.
Footnotes
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.