
Abstract
Introduction and Objectives:
Radical prostatectomy (RP) is associated with a high risk of intraoperative blood loss and subsequent blood transfusions. The shift in surgical technique from open radical prostatectomy (ORP) to robot-assisted radical prostatectomy (RARP) has resulted in lower operative blood loss, and reduced the need for transfusions. We analyzed the American College of Surgeons National Surgical Quality Improvement Project (ACS-NSQIP) database to compare real-world, contemporary trends in utilization and timing of blood transfusion following ORP and RARP.
Methods:
We identified men undergoing both RARP and ORP and then queried for patients who received a blood transfusion in the perioperative period. The outcomes of interest were need and timing of perioperative blood transfusion (PBT), which was categorized into early (postoperative day [POD] ≤1) or late (POD ≥2). Logistic regression analysis was used to identify variables associated with the need and timing for PBT.
Results:
A total of 16,144 men who underwent RP were identified from 2007 to 2012. The overall PBT rate was 3.1%. Highest rate of transfusions occurred on day of surgery for patients undergoing ORP, and first POD for patients undergoing RARP. On multivariate analysis significant predictors of blood transfusion included history of bleeding disorder (OR: 2.8, p=0.002), preoperative dyspnea (odds ratio [OR]: 1.7, p=0.03), starting hematocrit <42% (OR: 1.9, p<0.001), open approach (OR: 0.09, p<0.001), year of surgery (OR: 0.5, p<0.001), resident involvement (OR: 1.6, p=0.003), and operative time (OR: 4.4, p<0.001). The only predictor of receiving a blood transfusion on POD 2 or later was having the procedure performed through a robot-assisted approach (OR: 3.7, p<0.001).
Conclusions:
In this study we found that the rate of perioperative transfusions is lower than previously published. A clear separation in timing of transfusion exists based on the utilized surgical approach. It is prudent that surgeons performing RARP be aware of the low, but present risk of a delayed blood transfusion.
Introduction
R
One of the proven advantages of robot-assisted radical prostatectomy (RARP) over ORP has been lower operative blood loss and reduced need for blood transfusions. 3 This is thought to be secondary to the tamponade effect created by pneumoperitoneum, and magnified field of view, which may aid in control and identification of smaller venous sources of bleeding. Several large-scale studies have previously reported the differences in complications between ORP and RARP, 4 –8 and more specifically the higher rates of blood transfusion with the open approach. However, to our knowledge, this is the first study to examine the timing of transfusions (intraoperative or delayed) since the advent of RARP compared to ORP.
The American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) is a multi-institutional data source that prospectively collects data on 135 variables including intraoperative variables and 30-day postoperative mortality and morbidity outcomes for randomly assigned patients undergoing major inpatient and outpatient surgical procedures. This method of data collection has been shown to be more reliable than administrative databases that primarily rely on diagnosis and procedures codes. 9 In this study, we analyzed the ACS-NSQIP database to compare real-world, contemporary trends in utilization and timing of blood transfusion following ORP and RARP.
Materials and Methods
Data source
We utilized the American College of Surgeons National Surgical Quality Improvement Program Participant Use File (ACS-NSQIP PUF). The ACS-NSQIP PUF is a Health Insurance Portability and Accountability Act-compliant, multi-institutional data source available to researchers at institutions participating in the ACS-NSQIP. 10,11 Participating hospitals prospectively collect preoperative through 30-day postoperative data on randomly assigned patients. A trained surgical clinical reviewer at each participating hospital validates and submits the data to ACS-NSQIP. Periodic site visits are performed to continually audit the data and ensure inter-rater reliability.
Patient selection
The study cohort was populated through a query of the 2007 to 2012 ACS-NSQIP PUFs for all prostatectomy cases: RARP and ORP using primary Current Procedural Technology codes: 55866- RALP and 55840, 55842, 55845 (ORP). 12 Readmission data was available for patients undergoing surgery starting in 2011, as readmission data prior to that year were not being recorded. Patients who underwent emergency surgery (n=153), and patients who were American Society of Anesthesiology (ASA) class 5 (n=6), ventilator dependent (n=19), or had preoperative sepsis or systemic inflammatory response syndrome (n=271) at the time of surgery were also excluded to focus on elective cases.
Patient and hospital characteristics
Demographics including age, race, gender, body mass index, ASA physical status, smoking status, chronic steroid use, functional status, nutritional status as assessed by preoperative serum albumin, preoperative weight loss, presence of metastatic disease, Charlson comorbidity index, baseline comorbidities, operative time, and resident involvement were examined. 13
Outcome analysis
The primary outcome of interest was requiring perioperative blood transfusion (PBT), which was categorized into early (postoperative day [POD] ≤1) or late (POD ≥2). Variables were analyzed with Student's t-test for continuous variables and chi-square test categorical variables. Variables were introduced into the multivariate logistic regression model if n≥10 and p<0.2. This regression yielded an independent odds ratio (OR), 95% confidence interval, and p-value for each potential predictor. All analyses were conducted with SAS, version 9.3 (SAS Institute, Cary, NC). All statistical tests were two-sided with statistical significance determined at the p<0.05 level.
Results
A total of 16,144 men who underwent RP were identified from 2007 to 2012 of which 12,746 (79.0%) underwent RARP and 3398 (21.0%) underwent ORP. Table 1 depicts the patient demographics broken down by occurrence of transfusion and timing of transfusion. Overall 503 (3.1%) of all patients received a blood transfusion. When stratified by surgical approach, the number of patients requiring blood transfusion was 342 (10.1%) in the open surgery group and 161 (1.3%) in the RARP group (p<0.001). When PBT was stratified by POD, the highest rate of transfusion occurred on day of surgery for patients undergoing ORP, and on POD 1 for those undergoing RARP (Fig. 1). Men who received a blood transfusion were more likely to have ASA class ≥3 (38.6% vs. 31.1%, p<0.001), have a history of bleeding disorder (2.6% vs. 0.9%, p<0.001), preoperative dyspnea (4.4% vs. 2.8%, p=0.036), lower starting hematocrit (41.6% vs. 44.2%, p<0.001), and longer operative time (212 minutes vs. 195 minutes, p<0.001).
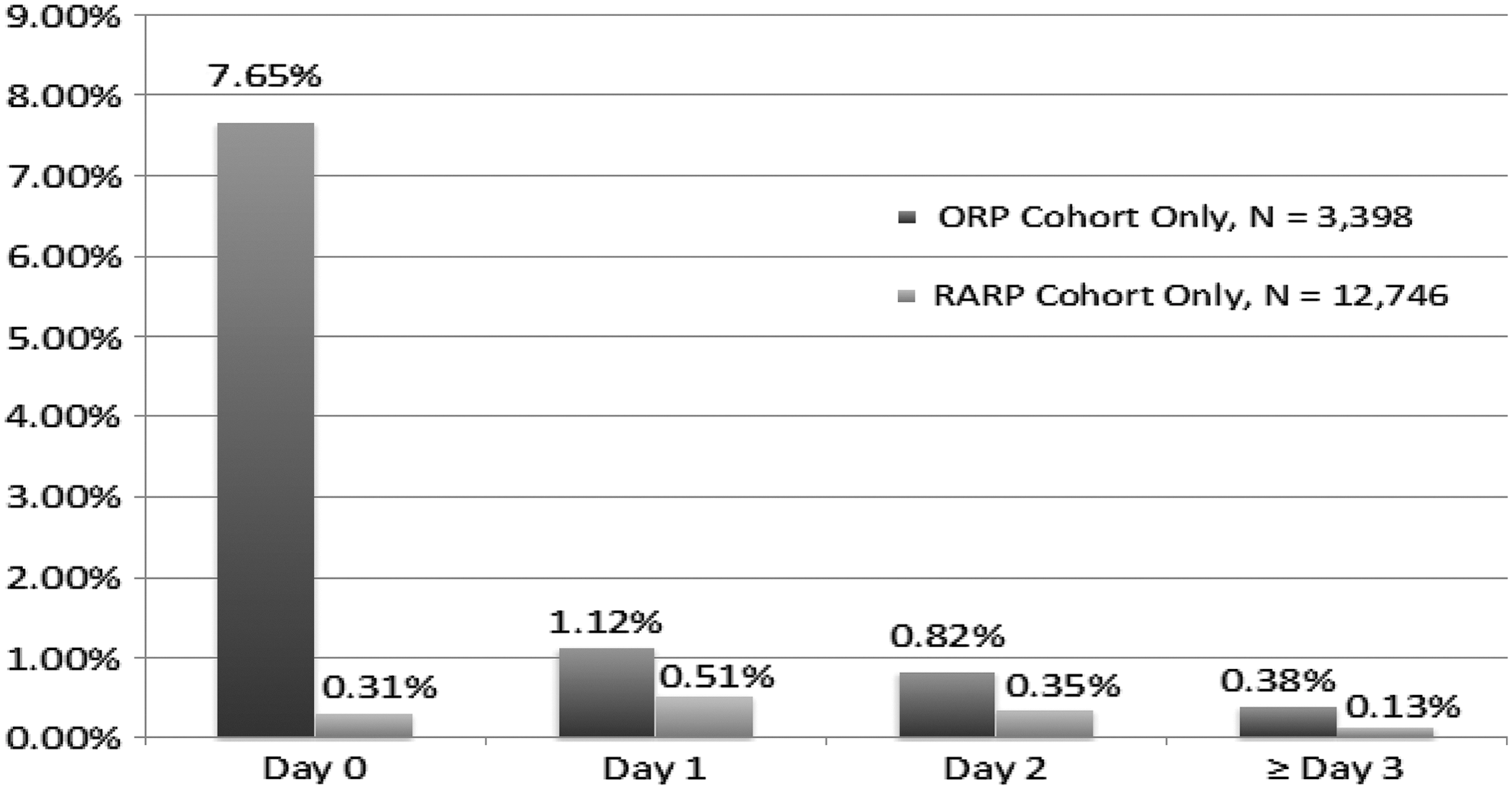
Perioperative transfusion rates.
ASA=American Society of Anesthesiology; HD=hospital day; ORP=open radical prostatectomy; RARP=robot-assisted radical prostatectomy.
On multivariate analysis (Table 2) significant predictors of blood transfusion were history of bleeding disorder (OR: 2.8, p=0.002), preoperative dyspnea (OR: 1.7, p=0.03), starting hematocrit<42% (OR: 1.9, p<0.001), open approach (OR: 0.09 p<0.001), year of surgery prior to 2011 (OR: 0.5, p<0.001), resident involvement (OR: 1.6, p=0.003), operative time >90 minutes (OR: 4.4, p<0.001), and any postoperative complication (OR: 2.2, p<0.001). Among the subgroup of patients undergoing RARP, predictors of any transfusion were history of bleeding disorder, lower preoperative hematocrit, and year of surgery 2009 or earlier (Table 3). Resident involvement and operative time were not predictive of PBT for the RARP group. Within the group undergoing ORP (Table 4), predictors of PBT included preoperative hematocrit<42 (OR: 2.1), resident involvement in the case (OR: 1.9), and operative time greater than 90 minutes. When examining the timing of PBT, predictors of early transfusion (POD 0 or 1) included, history of bleeding disorder, preoperative dyspnea, preoperative hematocrit <42%, year of surgery before 2010, resident involvement, open surgical approach, and longer operative times (Table 5). The only predictor of receiving a blood transfusion on POD 2 or later was having the procedure performed through a minimally invasive surgical approach (OR: 3.7, p<0.001).
CI=confidence interval; HCT=hematocrit; OR=odds ratio.
POD=postoperative day.
Discussion
The risk of perioperative transfusion exists for all patients undergoing RP. The morbidity associated with blood transfusions has been well documented. 2 In our study, the rate of blood transfusion was 7.8 times higher for patients undergoing ORP than those treated with RARP. The findings of our study are in accordance with other recently published studies reporting significantly lower rates of transfusion in patients undergoing RARP. 3,5 –8,12,14 Recently published meta-analysis of outcomes after open, laparoscopic, and robot-assisted prostatectomy has shown a 7.6-fold higher rate of blood transfusions in ORP compared with RARP. 6 Using Nationwide Inpatient Sample, Trinh et al. 8 found that compared with open surgery, RARP was associated with lower rates of blood transfusions, shorter length of stay, and lower overall complication rate. In a propensity score matched cohort that adjusted for inherent biases associated with multivariable analysis, blood transfusion rates were 7.7% and 2.4% for open and robotic approaches, respectively.
Study by Pierorazio et al. 7 examined a group of 18,049 men who had undergone open or minimally invasive prostate surgery at Johns Hopkins from 1991 to 2011 and found that the rate of anemia requiring blood transfusion was 9 (0.13%) and bleeding requiring re-exploration only occurred in six (0.08%) patients. Surprisingly, in this study, the rate of transfusion was slightly higher for the group undergoing minimally invasive surgery. This finding may reflect increased surgical expertise of the surgeons performing ORP, who performed, on average, 1400 more operations than those performing robotic procedures.
The effect of the surgical experience on perioperative outcomes including estimated blood loss and operative time has been well described. In a study examining perioperative outcomes during the first 700 RARP cases, by Zorn et al. 15 found that compared to the first 300 cases, there was significant reduction in operative times, operative blood loss, and positive surgical margin rate. Similarly, in a study examining 27,348 RARP performed by 744 surgeons using an administrative inpatient and outpatient database (Premier Research Perspective Database), surgeons further along their learning curve showed significant improvements in surgery time, hospital stay, conversion rates, and complication rates. 15,16 We found that the year of operation was a significant predictor of requiring a blood transfusion within the RARP group only; with patients undergoing surgery in 2009 or earlier having a significantly higher risk of needing transfusion compared to later years. This finding is likely reflective of increasing surgical experience and expertise among robotic surgeons resulting in improved perioperative outcomes.
With continued adoption of robotic technology, the progression along the curve of robotic surgery skill set may start to occur increasingly earlier in a surgical trainee's career, without negative repercussions on patient outcomes. A study by Schroeck et al. demonstrated that in a structured teaching program, trainee participation in as much as a third of a case did not impact estimated blood loss or positive surgical margin rate. 17 Our data show further support for this finding, with no association seen between perioperative transfusions and resident involvement in RARP cases.
To our knowledge, this is the first study in which the temporal relationship of PBT has been reported. We found that for men undergoing radical prostate surgery, the majority of PBT on day of surgery occur with open procedures, and on POD 1 or later with robotic procedures. In fact, the only risk factor for receiving a transfusion on second POD or later was having undergone a robot-assisted procedure. While RARP has been shown to have several advantages over ORP including lower operative blood loss, decreased perioperative pain, and shorter hospital stay, physicians must be cognizant of the rare, but increased risk of delayed bleeding.
Several important limitations and strengths of this study should be noted. Data was acquired through a large nationally representative quality improvement database and therefore the results may not be generalizable. As with all retrospective studies, a number of patient and physician preferences that we are unable to measure may have influenced surgical decision making leading to selection bias. Furthermore, analysis of the data cannot identify perioperative use of medications that increase the risk of bleeding complications.
Conclusions
The current rate of perioperative transfusions is lower than previously published, but is highly dependent on the surgical approach utilized. A clear separation in timing of transfusion exists based on the utilized surgical approach. It is important for surgeons performing RARP to have knowledge of the low, but increased risk of a delayed blood transfusion. Trainee involvement in RARP cases does not alter the risk of requiring a PBT.
Disclaimer
American College of Surgeons National Surgical Quality Improvement Program and the hospitals participating in the ACS-NSQIP are the source of the data used herein; they have not verified and are not responsible for the statistical validity of the data analysis or the conclusions derived by the authors.
Ethical Approval
De-identified patient information is freely available to all institutional members who comply with the ACS-NSQIP Data Use Agreement. The Data Use Agreement implements the protections afforded by the Health Insurance Portability and Accountability Act of 1996 and the ACS-NSQIP Hospital Participation Agreement.
Footnotes
Disclosure Statement
No competing financial interests exist.