
Abstract
Introduction:
The factors that contribute to continence following robot-assisted radical prostatectomy (RARP) are currently being investigated. The purpose of this study is to determine the relationship of the bladder neck location on postoperative cystogram to subsequent continence rates following RARP.
Patients and Methods:
A retrospective review of 611 consecutive RARP patients identified 215 patients with a postoperative cystogram. A ratio was created by measuring the distance from the superior edge of the pubic symphysis to the bladder neck and dividing it by the total pubic symphysis height, termed the bladder neck to pubic symphysis (BNPS) ratio. Odds ratios with 95% confidence intervals (CI) were calculated for the relationship between incontinence and BNPS tertile categories.
Results:
At 3-month follow-up, continent patients had a mean BNPS ratio of 0.39 (95% CI 0.35, 0.43), while incontinent patients had a mean BNPS ratio of 0.49 (95% CI 0.42, 0.56; p=0.01). At 12 months, the mean BNPS ratio was 0.40 (95% CI 0.37, 0.44) for continent patients, whereas incontinent patients had a mean BNPS ratio of 0.60 (95% CI 0.43, 0.77; p=0.001). When analyzed as tertile groups, the corresponding incontinence rates at 12 months were 2.8%, 2.8%, and 19.4% for the lowest, middle, and highest BNPS tertiles, respectively.
Conclusions:
Postprostatectomy bladder neck location defined by the BNPS ratio on cystogram correlates with continence rates and may predict patients at risk for prolonged incontinence. Efforts designed to preserve support of the bladder neck and sphincteric complex in relation to the pubic symphysis may improve both early and late continence.
Introduction
I
Patients and Methods
After the institutional review board approval, a retrospective review was performed on 611 consecutive robot-assisted radical prostatectomy (RARP) patients. All surgeries were performed by one of the two surgeons in a single academic institution between March 2005 and December 2011. Information regarding preoperative demographics and postoperative outcomes was collected. In addition, specific information regarding the location of the bladder neck on postoperative cystogram and continence status based on pad usage was determined. Continence was assessed by a physician interview at follow-up clinic appointments. Continence was divided into two categories: early continence (<3 months) and late continence (>12 months). In the analysis of urinary continence, patients were stratified by pad usage into those patients wearing no pad or only a safety pad (classified as continent) and those wearing >1 pad per day (classified as incontinent). Patients who received treatment for incontinence such as slings or artificial urinary sphincters before 12 months post-RARP were considered incontinent at 12 months. RARP was performed with a transperitoneal approach using a standard four-armed robotic configuration with two additional assistant ports. A cystogram was performed at the discretion of the surgeon 7–21 days postoperatively.
Standardized cystogram protocols consisted of instilling 250 mL of half-strength Omnipaque contrast (GE Healthcare, Inc., Cork, Ireland) into the bladder by gravity, followed by clamping of the Foley catheter. With the catheter under no tension, plain cystogram films were obtained in the anterior–posterior view and saved on the IMPAX radiograph viewing system (Agfa Healthcare IMPAX, Ridgefield Park, NJ). Interpretation of cystograms was performed by a single urologist blinded to continence status to eliminate interobserver variability. Bladder neck location, defined by the lowest extension of the tapering contrast, was evaluated in relation to the superior aspect of the pubic symphysis. The distances were recorded as negative values when the bladder neck was cephalad to the pubic symphysis and positive values for bladder neck extending caudad to the superior aspect of the pubic symphysis. To control for potential differences in magnification provided by the cystogram, the bladder neck–pubic symphysis distances were divided by the total pubic symphysis height to obtain a corrected ratio, called the bladder neck to pubic symphysis (BNPS) ratio (Fig. 1). A higher, more positive BNPS ratio indicates an overall lower anatomical bladder neck position on the postoperative cystogram.
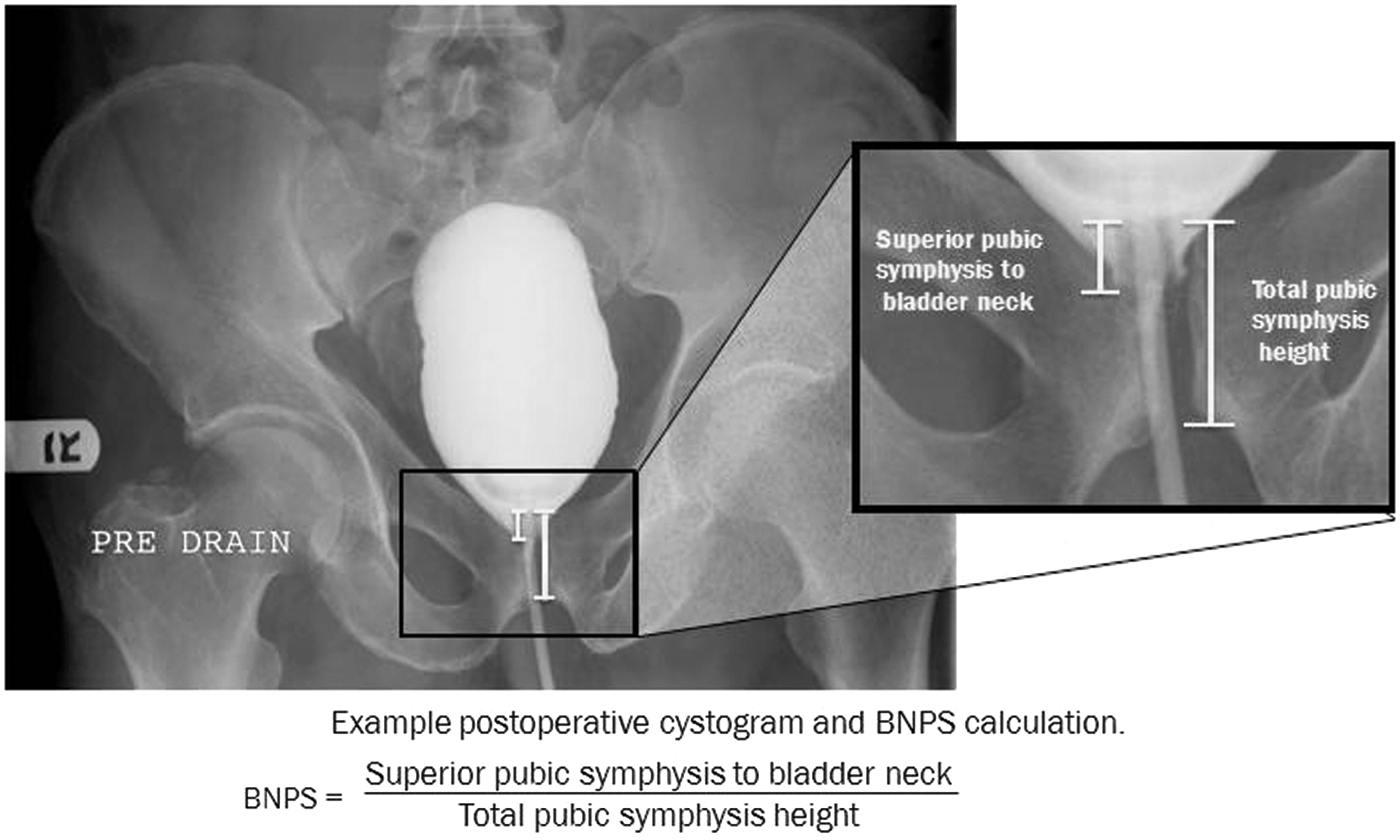
Example postoperative cystogram and bladder neck to pubic symphysis (BNPS) calculation.
All data were analyzed with SAS v9.2 (SAS Institute, Inc., Cary, NC). BNPS ratios were calculated for each patient. A Student's t-test was performed to analyze mean scores for BNPS ratios between continent and incontinent patients, separately at 3 and 12 months postsurgery. An alpha level of 0.05 was used to determine statistical significance. Logistic regression analysis was used to generate the odds ratios with 95% confidence intervals (CI) calculated for the relationship between incontinence and BNPS categories.
Results
Of the 611 RARP patients, 215 with postoperative cystogram as well as 3- and 12-month postoperative incontinence data were used for analysis. Overall, at 3 months, 152 patients (70.7%) were continent and 63 patients (29.3%) were incontinent. At 12 months, 197 patients (91.6%) were continent and 18 patients (8.4%) were incontinent. Preoperative characteristics of continent and incontinent patients were similar at both 3 months (Table 1) and 12 months (Table 2) post-RARP.
ASA=American Society of Anesthesiologists; BMI=body–mass index; BNPS=bladder neck to pubic symphysis; PSA=prostate-specific antigen.
At 3-month follow-up, continent patients had a mean BNPS ratio of 0.39 (95% CI 0.35, 0.43), while incontinent patients had a mean BNPS ratio of 0.49 (95% CI 0.42, 0.56; p=0.01). At 12 months, the mean BNPS ratio was 0.40 (95% CI 0.37, 0.44) for continent patients, whereas incontinent patients had a mean BNPS ratio of 0.60 (95% CI 0.43, 0.77; p=0.001). Forty-five out of the 63 patients (71.4%) who were incontinent at 3 months gained continence at 12 months. The mean BNPS ratio for those who became continent at 12 months was 0.44 compared to 0.60 for those who remained incontinent (p=0.038).
When sorted by BNPS, the ratios of the patients in the lowest tertile (highest bladder neck positions) ranged from −0.41 to 0.32, the middle tertile from 0.32 to 0.52, and the highest tertile from 0.52 to 1.14 (Table 3). The corresponding incontinence rates at 3 months were 19.7%, 27.8%, and 40.3% for the patients in the lowest, middle, and highest tertile of BNPS ratios. The odds ratio for having incontinence at 3 months was 2.75 (1.30, 5.82) (p=0.008) for the patients with the highest BNPS ratios. At 12 months, the incontinence rates were 2.8%, 2.8%, and 19.4% for the lowest, middle, and highest BNPS tertiles, respectively. The patients with the highest tertile of BNPS ratios were 8.33 times more likely to have persistent incontinence at 12 months (p=0.006).
Lowest BNPS tertile used as reference to calculate ORs.
Bold type indicates statistically significant values.
OR=odds ratio.
Discussion
RARP has quickly become the most common surgical management for prostate cancer. 6 A potential side effect is urinary incontinence, which occurs following radical prostatectomy in 5–20% of patients. 2 Moreover, ∼4.8% may have significant incontinence that could negatively impact quality of life. 7
Significant progress has been made into understanding, preventing, and treating postprostatectomy incontinence. Stress urinary incontinence is the most prevalent type of postprostatectomy incontinence and is thought to be related most commonly to intrinsic sphincter deficiency. 2,4 Other contributing mechanisms for continence may include structural and anatomic support of the sphincter, 8,9 bladder compliance, 4 and detrusor stability. 2,4 The levator ani muscles, pubourethral ligaments, puboprostatic ligaments, and fibrous raphe form the pelvic floor, which suspends and supports the bladder, prostate, and urethra. Compromised anatomic support may lead to the bladder neck descent and change in the vesicourethral angle. This may result in an alteration in force transmission during periods of stress, ultimately impairing normal continence. 5
The correlation between pelvic floor support and urinary incontinence has been previously studied where fluoroscopic imaging was utilized to evaluate bladder neck descent at rest and with straining. 10 Some classifications of incontinence types are generally representative of lower bladder neck and urethra in relation to the symphysis pubis, and thereby a greater degree of stress urinary incontinence. 11 The fact that anatomic support of the bladder neck and sphincteric complex are associated with continence in women suggested that similar loss of urethral and bladder neck support could also play a role in male postprostatectomy incontinence.
Our series is designed to evaluate the relationship between continence and anatomic support using postoperative cystography and determine whether there is a relationship between having a high proximal urethra and bladder neck and subsequent continence status at 3 and 12 months following RARP. The BNPS ratio can also be used to predict patients who may have prolonged and higher degrees of incontinence. These patients may be placed on a more aggressive bladder rehabilitation program at the time of catheter removal. In addition, this information can be used to help manage the expectations of the patient.
There are several limitations to this study. It is a retrospective study with inherent limitations such as selection bias. Since these surgeries were performed by two surgeons in a single center, additional studies will be required to see whether this metric predicts continence by surgeons in other centers. In addition, the absence of a preoperative cystogram does not account for changes in bladder neck position that may arise from the prostatectomy. Future studies may evaluate how the anatomic position of the bladder neck and urethra change from baseline following radical prostatectomy. While the BNPS ratio is helpful in counseling the individual surgical patient, this study does not determine the etiologies for this incontinence. Whether the elevated BNPS ratio is simply due to technical factors at the time of surgery versus specific preoperative parameters is not clear and requires further evaluation. The next step would be to identify factors leading to an increase in BNPS ratio intraoperatively to allow prevention of postprostatectomy incontinence. Another limitation is that the angle of the X-ray beam to the pubic symphysis at the time of cystogram may alter the position of the bladder neck. However, the use of the BNPS ratio was created specifically to minimize the influence of differences in angulations during the cystogram. Although the correlation between anatomic support and ultimate short- and long-term continence is intriguing, these findings must be confirmed in future studies.
Conclusions
Postprostatectomy bladder neck location defined by the BNPS ratio on postoperative cystogram correlated with continence at <3 and >12 months. Cystograms could potentially be used in the future to identify individuals who may suffer from prolonged incontinence and thus tailor management and patient expectations. This study suggests that efforts designed to support the bladder neck in a fixed, anatomic retropubic location may ultimately improve the return of continence in patients undergoing radical prostatectomy.
Footnotes
Disclosure Statement
No competing financial interests exist.