
Abstract
Purpose:
To determine the optimum dosage and instillation time for water-soluble polyvinylpyrrolidone (PVP)-hypericin for photodynamic diagnosis of bladder cancer and to monitor its use in regard to patient safety.
Patients and Methods:
Forty patients with a cystoscopically suspected bladder neoplasm were enrolled in this prospective phase IIA study. Different combinations of PVP-hypericin dosage (225 μg and 75 μg and instillation time (120, 60, 30, 15 min) were used to evaluate the optimal conditions. After a run-in cohort of five patients to validate the test method, each group comprised seven patients. All intravesical lesions were documented, and their fluorescence characteristics were recorded. Dose finding was the primary, safety the secondary end point.
Results:
Fluorescence intensities for the first two groups (225 μg PVP-hypericin for 120 and 60 min, respectively) were not different. For group three (225 μg for 30 min), both specific fluorescence and background noise were reduced. A shorter instillation time (225 μg for 15 min) or lower dose (75 μg for 30 min) was considered insufficient for lesion identification. A dose of 225 μg PVP-hypericin instilled for 30 minutes was determined as appropriate for the detection of lesions. Of the total 93 identified lesions, 62 were detected with both white light and fluorescence, 25 were seen with blue light only, and six with white light only. It was possible to identify additionally two carcinoma in situ, eight pTa, and one pT1 lesions with PVP-hypericin and blue light. PVP-hypericin was safe and well tolerated.
Conclusion:
The optimum combination of dosage of PVP-hypericin and its instillation time was established and will be used to determine sensitivity and specificity of PVP-hypericin cystoscopy in a larger multicenter phase IIB study. The preliminary data of this study hint to a higher sensitivity of hypericin-assisted fluorescence cystoscopy.
Introduction
B
Nevertheless, HAL and 5-ALA have the limitations of significant photobleaching and a recommended instillation time of 60 and 120 minutes, respectively, which can cause problems regarding both organizational issues and patient tolerance. Moreover, specificity for the detection of bladder cancer lesions was unsatisfying so far, ranging between 41% and 67% for ALA. 11 For HAL, two studies report concerning specificity, which was 43% and 82%, respectively, and several studies, with one exception, showed consistently higher false-positive rates of HAL compared with white-light cystoscopy. 4 –8,12 –14
Hypericin is a naturally occurring substance found in St. John's wort (Hypericum perforatum). It is used for the treatment of patients with mild to moderate depression. Recent studies report, in addition, antineoplastic, antitumor, and some antiviral activities, although the confirmation of these data is incomplete and the mechanisms of these activities still remain largely unexplained. 15 Hypericin is known for its photosensitizing properties and selective accumulation in malignant bladder tissue. 16 Studies are ongoing using hypericin in the setting of photodynamic therapy, because an apoptosis-inducing effect of hypericin in cancer cells after photoactivation has been shown. 17,18
Studies conducted in bladder cancer patients 5 to 10 years ago have shown the general feasibility and safety of hypericin fluorescence cystoscopy. In addition, there seems to be a higher specificity for the detection of CIS, albeit no direct comparison between different substances has been conducted so far. Positive lesions show red fluorescence when excited by a light source in the light-blue spectral range. All past studies were performed with albumin-bound hypericin, 16,19,20 except the most recent one that used polyvinylpyrrolidone (PVP)-hypericin but without determining the optimal dose (Table 1). 21
FC=fluorescence cystoscopy; WL=white light; CIS=carcinoma in situ; NPV=negative predictive value; PPV=positive predictive value; PVP=polyvinylpyrrolidone.
PVP-hypericin has the advantage of being a well-standardized water-soluble substance without the necessity of binding to serum proteins. All these mentioned studies showed a higher detection rate for fluorescence cystoscopy than for white light cystoscopy, a good sensitivity and specificity, especially for the detection of CIS, and a lack of photobleaching, allowing an extended examination time. This makes PVP-hypericin an attractive subject of further investigations. The primary objective of this study was to establish the optimum dose and instillation time of PVP-hypericin for detection of NMIBC.
Patients and Methods
Patients
A total of 40 patients with cystoscopically suspected bladder cancer, either primary or recurrent, were included in this prospective trial between September 2009 and October 2010 (Table 2). Main exclusion criteria were a history of bacillus Calmette-Guérin instillation therapy in the last 6 months, a transurethral resection in the last 3 months, macroscopic hematuria, or hints of a urinary tract infection. The study protocol was approved by the local ethics committee, and the study was registered in EudraCT. The study was conducted in accordance with the International Conference on Harmonization guidelines for Good Clinical Practice and the Declaration of Helsinki. All patients signed written informed consent before study entry.
CIS=carcinoma in situ.
Imaging system
Because of the similar emission spectra of PVP-hypericin and protoporphyrin IX (PpIX), cystoscopic equipment developed for the use of 5-ALA fluorescence cystoscopy could be used. In this study, the photodynamic diagnostic system of Richard Wolf GmbH, Knittlingen, Germany, was applied. For the calculation of the relative intensities between the blue (excitation), red (fluorescence), and green (autofluorescence) channel, raw sensor data were used without any transformation. A high red-to-green ratio (r/g) together with a high red-to-blue ratio (r/b) is considered high quality. These objective ratios together with the impression of the investigator (MS) were considered suitable to determine the lower limits of the instillation time and dose.
To prove the independence of the r/g and r/b intensity ratios against variations of distance and imaging parameters, a piece of Spectralon® was used. Constant ratios from 5 to 50 mm distance of the endoscope to the model surface using frame integration and electronic light control were found. To test the dependence of the ratios against variations of fluorophor concentration, an epoxy resin model with optical properties similar to bladder tissue was mixed adding scattering and absorbing particles in an appropriate amount and ratio. With this model with a flat pit in its center containing fluorescent solution of hypericin, the dependence of fluorescence to autofluorescence (r/g) ratio and fluorescence to excitation intensity (r/b) ratio was found to be constant with respect to distance and linear with respect to relevant fluorophor concentrations.
To validate the test method based on the phantom, the modified imaging system was tested on a first group of five patients.
Study design
The 40 patients were arranged into six groups. The fluorescence data of the first five patients (group 0) were used to validate the test method as mentioned above. After that, each group consisted of seven patients. The first dose, 225 μg PVP-hypericin, was chosen based on a previous study using a dose of 250 μg hypericin bound to PVP to detect malignant lesions. 20 Therefore, the parameters for the first group were 225 μg PVP-hypericin instilled for 120 minutes (group 1). In the following patient groups, the instillation time was gradually reduced (groups 2 to 4). Searching for the optimal combination of dose and instillation time, investigation of a second, lower dose combined with an instillation time ≤60 minutes seemed reasonable. A dose reduction to more than half of the initial dose (225 μg) was pursued; for that reason, the second PVP-hypericin dose selected was 75 μg. After completion of each group, the Drug Safety Monitoring Board decided about the following dose and time, adhering to the predefined decision tree (Fig. 1).
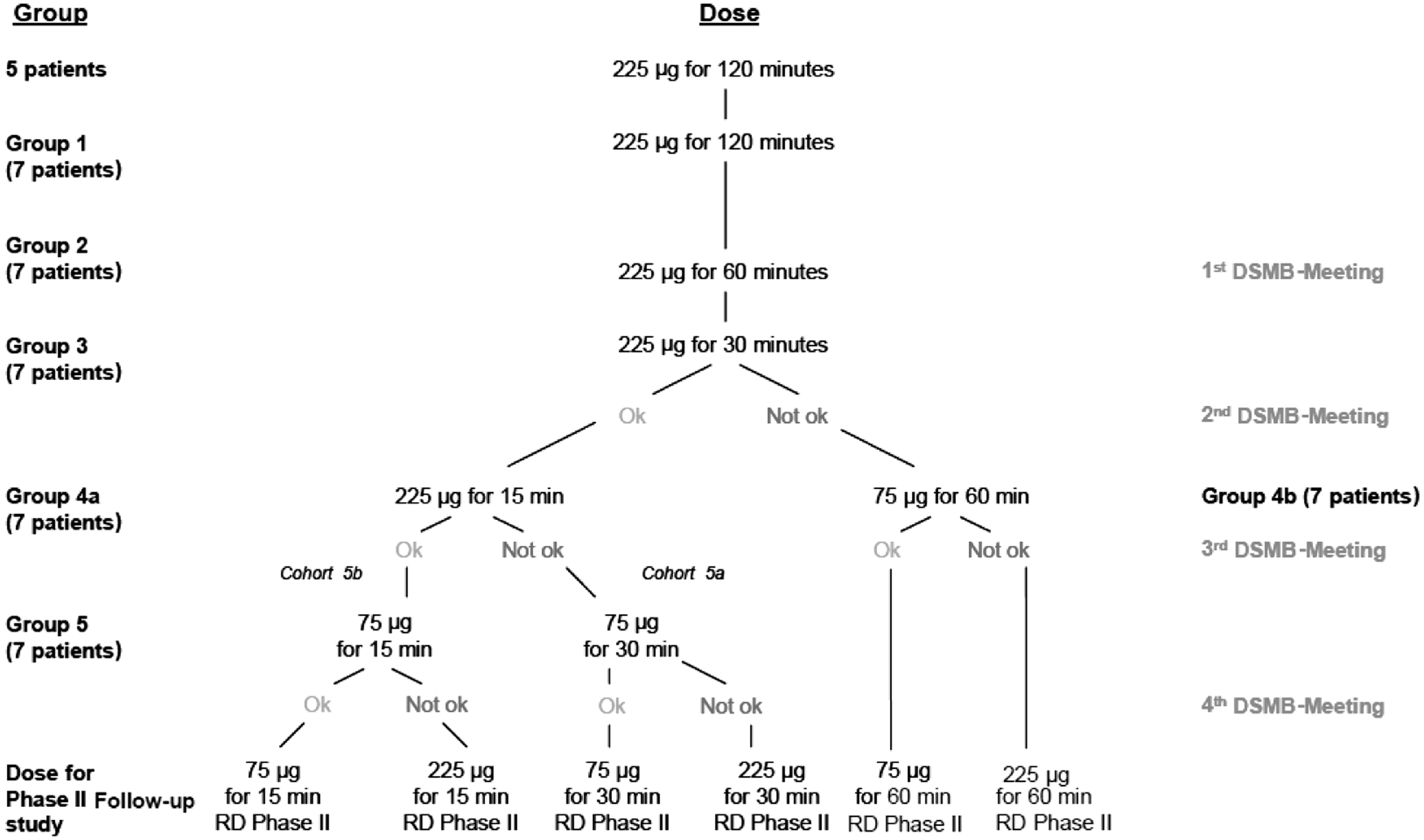
Decision tree for the dose-finding process. DSMB=Drug Safety Monitoring Board; RD=recommended dose.
Drug reconstitution
PVP-hypericin solution for intravesical administration was prepared by reconstitution of the PVP-hypericin powder (75 μg or 225 μg hypericin) with 50 mL sterile water for injection. The solution was freshly prepared before each administration.
Surgical procedures
All procedures were performed by a single experienced urologic surgeon (MS). Before transurethral resection of bladder tumor (TURBT), PVP-hypericin was instilled via a transurethral catheter. After the predefined instillation time, the bladder was emptied and the catheter removed. The surgical procedure started shortly thereafter. A thorough white-light cystoscopy was performed, and all found lesions were documented on a standardized bladder sheet. Thereafter, the light source was switched to the fluorescence mode. Raw data and preprocessed data images were taken and lesions documented as done in the white-light mode.
Follow-up
All patients were followed according to the Guidelines of the European Association of Urology. 10 Either white-light cystoscopy after 3 months or a re-TURBT after 6 to 8 weeks was performed in the study institution to document midterm safety. The study ended with the last patient finishing the follow-up examination.
Study objectives
The primary end point of the study was the evaluation of the most appropriate concentration (75 μg or 225 μg) and instillation time (120, 60, 30, 15 min) of PVP-hypericin based on fluorescence data and the surgeon's ability to detect the intravesical lesions. Safety was the secondary end point. Adverse events (AEs) were coded according to the Medical Dictionary of Regulatory Activities (MedDRA) using MedDRA Version 13.1.
Results
Patient population
The majority of the study population was male (33 of 40, 82.5%). All patients were of Caucasian origin, except one who was Arabic. The mean age for the whole group was 66.8 years (31–90). All 40 patients in whom PVP-hypericin was instilled were included in the Safety Analysis dataset. In regard to the Full Analysis dataset, the first five patients of the run-in phase were excluded. Moreover, one patient had no detectable lesions, so he was also excluded from the FA set, which finally included 34 patients. There were no relevant violations so that for the per-protocol analysis, none of the patients needed to be excluded.
225 μg PVP-hypericin for 30 minutes: Optimal dose and instillation time for detection of NMIBC
The measured fluorescence intensities and the statistical evaluation of the digitally analyzed images did not show any differences between group 1 (225 μg PVP-hypericin for 120 min) and group 2 (225 μg PVP-hypericin for 60 min). The fluorescence intensity of the tissue was very strong, resulting in saturation of the fluorescence signal in numerous image pixels. The specific coloring was reduced with 225 μg PVP-hypericin instilled for 60 minutes (group 2) and 30 minutes (group 3) with an associated decrease of the background noise. There was no statistical difference in the r/g relationship (data not shown). The color capacity after an instillation time of 30 minutes with 75 μg (group 5) and 15 minutes with 225 μg (group 4) was considered to be insufficient for identification of the lesions. The calculated red-to-green- and red-to-blue ratios for each group are depicted in Figure 2. The lower ratios obtained for groups 4 and 5 indicate that the fluorescence intensity obtained with 75 μg PVP-hypericin for 30 minutes or 225 μg for 15 minutes was insufficient.
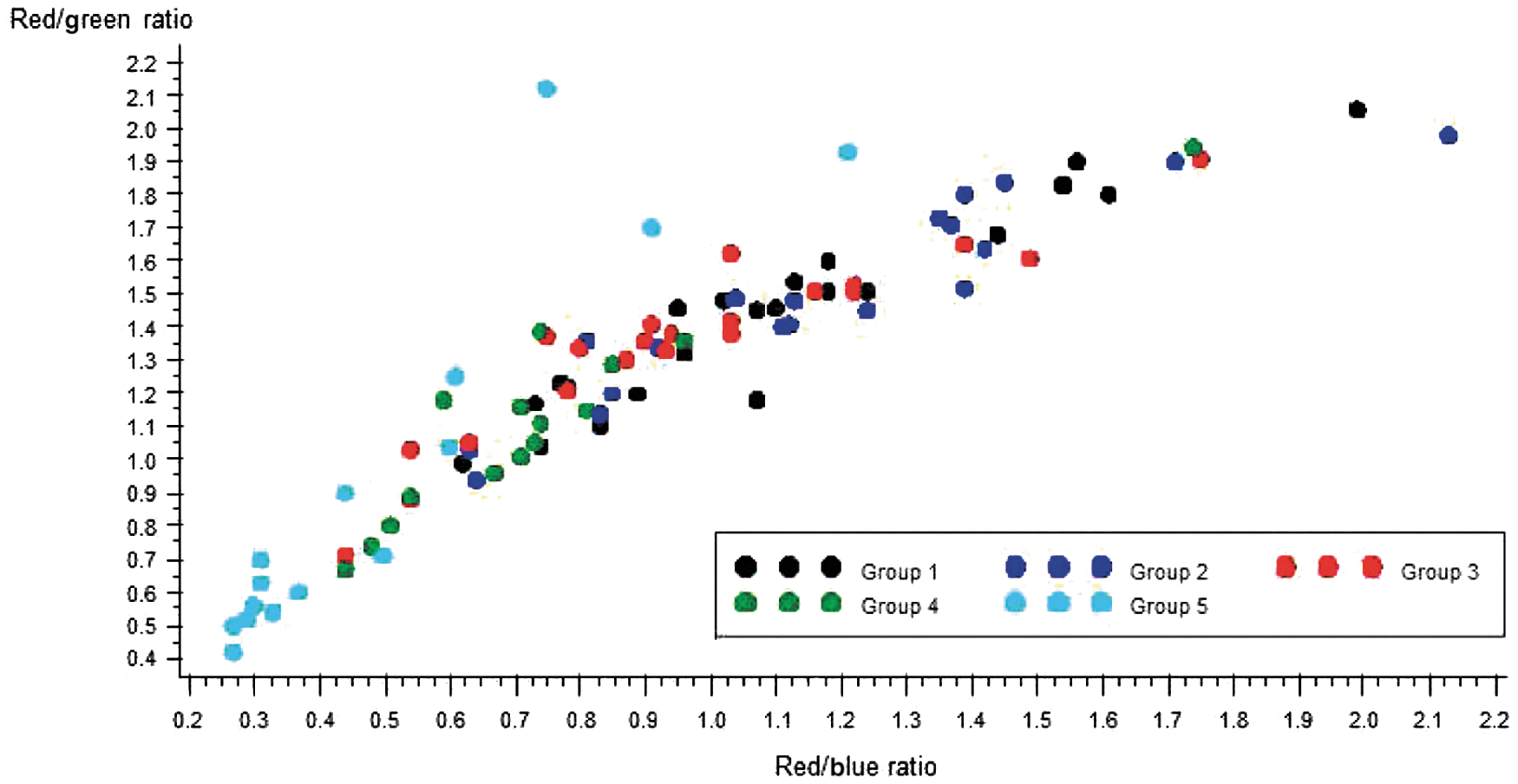
Scatter plot of red/green ratio by red/blue ratio for all lesions detected in each group. Lower ratios for groups 4 and 5 can be seen clearly.
Representative cystoscopic images for each group both in white and in blue light are depicted in Figure 3.
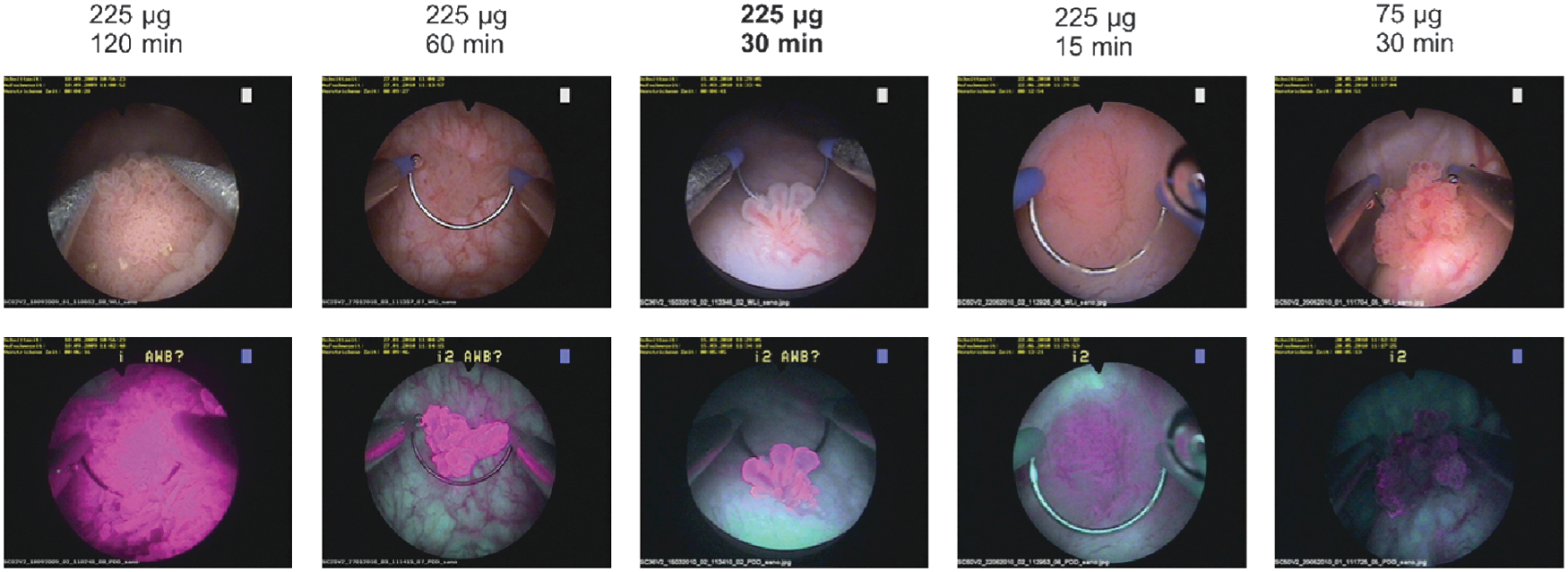
Appearance of a pTa, low grade tumor under white light and PVP-hypericin fluorescence cystoscopy. Different dosages and instillation times of PVP-hypericin are indicated. Variables in group 3 (225 μg, 30 min) are considered as most appropriate.
Additional malignant lesions could be detected with PVP-hypericin
In the 40 study patients, 93 intravesical lesions were detected, 62 both with white light and blue light, 25 with blue light only, and 6 with white light only. Of the 25 lesions additionally detected with blue light, 14 were benign and 11 malignant. Two extra CIS lesions were detected with PVP-hypericin and blue light—one in group 2 and one in group 3. Eight extra pTa lesions were seen with PVP-hypericin and blue light—three lesions in group 1, two in group 2, and three in group 3—as well as one extra pT1 lesion in group 2. Summarized, it was possible to identify additional two CIS, eight pTa, and one pT1 lesions with PVP-hypericin and blue light compared with white light in groups 1 to 3 (Table 2 and Fig. 4).
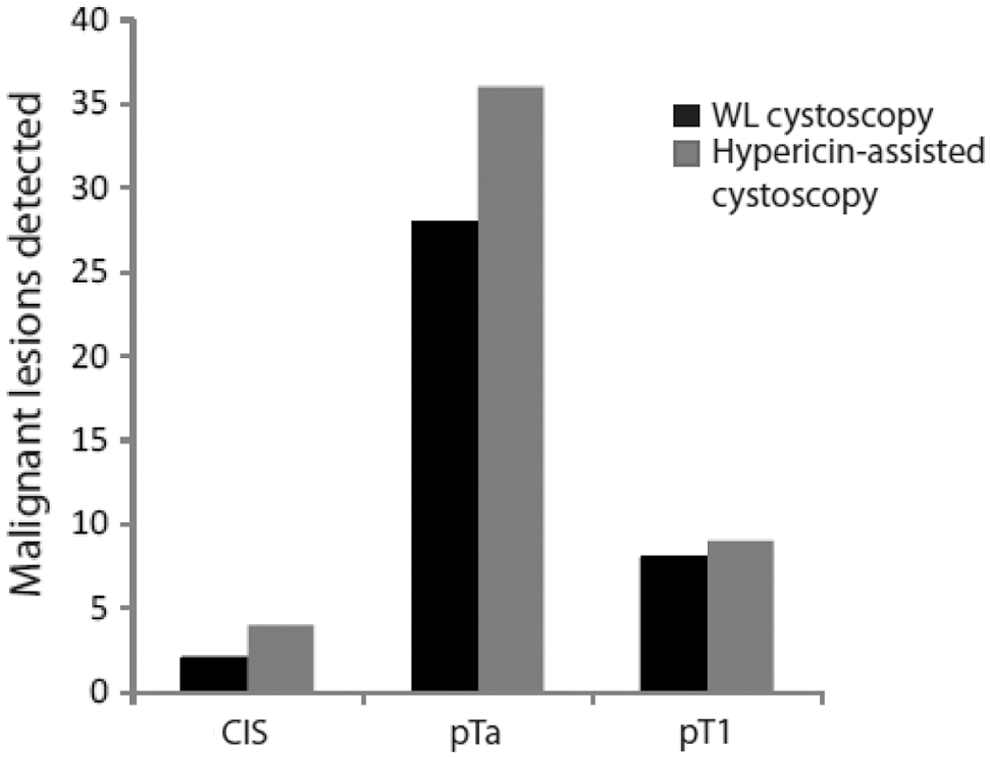
Number of detected lesions per histologic subtype in patient groups 1 to 3 with either white-light (WL) cystoscopy (black columns) or blue-light cystoscopy after PVP-hypericin instillation (grey columns). CIS=carcinoma in situ.
No extra lesions were detected in groups 4 and 5 with PVP-hypericin and blue light. One lesion in group 4, which was seen with white light only, was classified as pTa; all other lesions seen with white light only were benign. With the recommended dose and time for further clinical development (225 μg, 30 min), no malignant lesions were missed in the blue light mode. Overall, 53 of 87 (61%) lesions detected in the fluorescence mode were malignant.
Seven patients underwent follow-up fluorescence cystoscopy after 6 weeks with none of them showing residual tumor. Of the other patients, 12 had their first routine follow-up cystoscopy after 3 months in our institution.
PVP-hypericin was safe and well tolerated
A total of 29 AEs were registered during the study period with 21 of the 40 (52.5%) patients experiencing at least one AE. Of the AEs, 23 were considered unrelated to the study drug and 6 unlikely related. The most frequently reported AEs were postprocedural hemorrhage in four patients and bladder perforation in three patients. All bladder perforations and three of the four hemorrhagic episodes were considered as serious adverse events (SAEs); the remaining hemorrhage happened shortly after the primary resection and was not considered an important medical event. All bleeding episodes were treated with transurethral coagulation. Totally, eight SAEs were reported in seven patients (Table 3). All patients recovered from the SAE without sequelae. No patient discontinued the study early because of an AE. All AEs were of mild or moderate intensity; the AEs were not dose-dependent, and all were considered either unlikely or not related to the study medication. No clinically relevant trend was observed in the clinical laboratory results or vital signs.
Discussion
In this phase IIA trial, the optimum conditions for the intravesical instillation of PVP-hypericin were determined as 225 μg for 30 minutes. This decision was based on objective fluorescence raw data and the ability of the surgeon to identify intravesical lesions correctly. The raw data have shown high ratios in specific fluorescence/autofluorescence intensity and specific fluorescence/excitation intensity for groups 1 to 3 and low for groups 4 and 5.
There was an additional detection of malignant lesions in groups 1 to 3 but not in groups 4 and 5. The only false-negative finding for fluorescence cystoscopy was a pTa tumor in group 4. Sensitivity was not an objective of the present study. Nevertheless, 48 of 49 (98%) malignant lesions in groups 1 to 3 were detected by blue light cystoscopy and PVP-hypericin. Specificity cannot be addressed because no random biopsies were taken.
The instillation of PVP-hypericin was safe and well tolerated. This is shown by the fact that all AEs were of mild or moderate degree and were considered unrelated or unlikely related to the study drug. No patient needed to terminate the study earlier because of an AE. The most frequent AEs were postoperative hemorrhage with a need for intravesical coagulation and a small bladder perforation, both of which are clearly related to the surgical procedure itself.
Allergic reactions/hypersensitivity has been reported after oral and intravenous administration of St John's wort. Infrequent allergic skin reactions including rash, itching, and pruritus were reported in 0.5% to 2.0% of patients in clinical trials. 15,22 Conventional therapy with St. John's wort extract for depression does normally not cause phototoxic side effects. 23 Until now, no allergic reactions after intravesical instillation of hypericin have been reported. 16,20,21
Remarkably, hypericin fluorescence showed no photobleaching during the resection time. Although investigation of photobleaching of hypericin was not a primary objective in reported clinical studies so far, no photobleaching during illumination, endoscopy, or resection was reported in one study 21 and fluorescence up to 16 hours after instillation was reported by two others. 16,19 In this regard, PVP-hypericin differs substantially from HAL, the substance used today. Moreover, in this study, a shorter instillation time for PVP-hypericin (60 min vs 30 min) was determined as completely sufficient.
Sensitivity and false-positive rate of PVP-hypericin fluorescence cystoscopy will be addressed in a multicentric phase IIB study.
Footnotes
Acknowledgment
We explicitly express our thanks to the Richard Wolf GmbH for technical support of the study.
Disclosure Statement
The study was sponsored by Sanochemia Pharmazeutika AG (Vienna, Austria), of which one of the authors (Christina Abrahamsberg) is an employee.