
Abstract
Introduction and Objectives:
Caliceal leak after partial nephrectomy (PN) typically resolves with conservative management. However, persistent fistulae pose a formidable challenge that may require additional therapeutic actions.
Methods:
We describe a case of a patient with a solitary kidney who suffered a persistent urine leak following PN. A novel retrograde ureteroscopic approach was taken that utilized the combined techniques of caliceal fulguration and fibrin glue injection.
Results:
Imaging demonstrated resolution of the caliceal fistula at 13 months postoperatively.
Conclusions:
Persistent urine leak after PN remains a burdensome complication that often requires creative steps to resolve. Our case presents a solution using a novel ureteroscopic technique.
Introduction
P
Several minimally invasive approaches to dealing with prolonged urine leak have been previously described. 3 –9 In the present report, we describe a novel ureteroscopic approach to prolonged urine leak after PN in a solitary kidney combining caliceal fulguration and injection of fibrin glue.
Case
A 61-year-old man with a history of chronic kidney disease (stage 3, GFR 41–52) and a solitary kidney due to prior left radical nephrectomy for renal cell carcinoma (RCC) was found, on surveillance ultrasound, to have a new 6 cm right lower pole renal mass. Subsequent magnetic resonance imaging (MRI) demonstrated a 6.4 cm heterogeneously enhancing mesophytic mass encroaching the collecting system and renal sinus fat (RENAL score=9a, Fig. 1a–c). 10
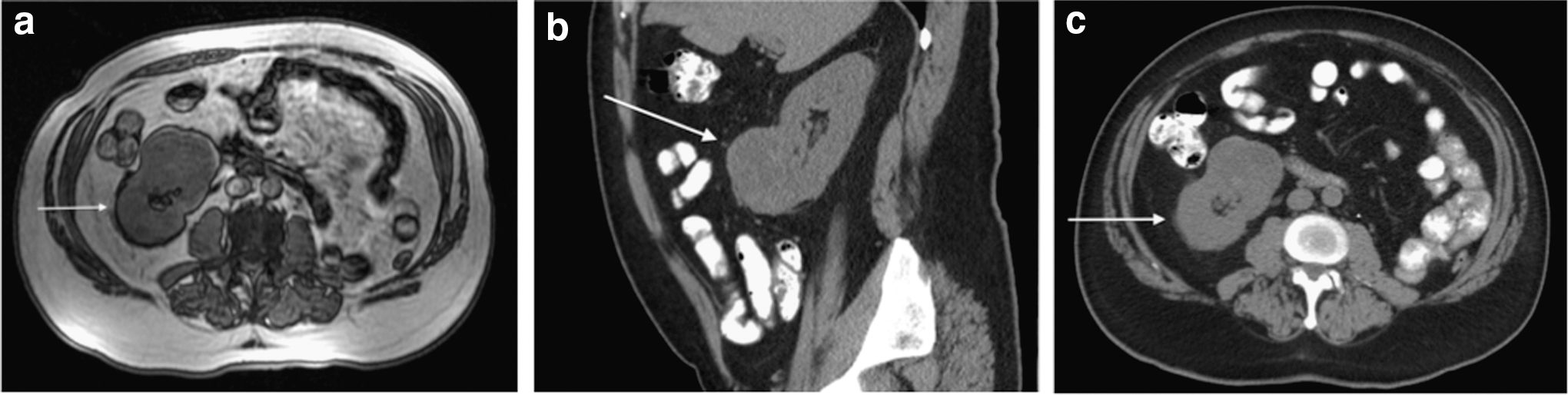
Preoperative nonenhanced magnetic resonance imaging (MRI) of the mesophytic renal mass:
The patient subsequently underwent a right retrograde pyelogram and ureteral stent placement at the time of open PN
Following hilar clamping and induction of regional hypothermia with ice slush, the tumor was resected; it was seen invading into the sinus fat and collecting system. The collecting system defects were closed with 4-0 Vicryl sutures. Floseal (©Baxter Healthcare Corporation) was placed into the resection bed. Fibrillar bolsters were placed and the renorrhaphy was completed with 1-0 Vicryl suture with the sliding clips. 11 Tisseel was drizzled over the repair followed by placement of a flap of perinephric fat. A 19F closed-suction drain was placed in the retroperitoneum. The Foley catheter was removed on postoperative day 3. Following this, the drain was removed before discharge when the output was <50 mL/24 hour. His serum creatinine peaked at 2.6 mg/dL on postoperative day 3 and returned to a baseline of 1.6 mg/dL by 6 weeks after surgery. Final pathology demonstrated a pT3a grade 2 clear cell RCC with negative margins.
At the 2 week follow-up, he noted a 15lb weight gain and leakage from the drain site. A noncontrast computed tomography (CT) of the abdomen and pelvis demonstrated a 7.7×3.3 cm crescentic lower pole pararenal fluid collection consistent with urinoma (Fig. 2a). The ureteral stent was seen in good position. A Foley was replaced and a percutaneous 8F pigtail drain was placed into the urinoma (creatinine>25 mg/dL). A repeat CT scan 3 weeks later demonstrated radiographic resolution of the urinoma, but the drain output remained persistently high at 90 to 150 mL daily. Despite advancing the drain and discontinuing drain suction, ∼100 mL of daily drainage continued for the next month. A percutaneous nephrostomy tube was not attempted due to concern for possible complication, given the lack of collecting system dilation in a solitary kidney. The patient was subsequently taken to the operating room for endoscopic management. Flexible right ureteropyeloscopy was performed through a 13F access sheath. Upon interrogation of the lower pole anterior calix, a 5 mm defect was observed through which the retroperitoneal drain pigtail could be seen. A 1.9F nitinol stone retrieval basket (©Boston Scientific) was deployed into the calix in the open position and 40W of coagulation current was applied to the exposed metal portion within the window of the basket handle to completely fulgurate the calix under direct ureteroscopic vision (Fig. 3). Fibrin glue was then injected under direct vision into the fulgurated calix. A 7F×26 cm ureteral stent was then placed in the renal pelvis and the retroperitoneal drain was pulled back 3 cm away from the kidney. A Foley catheter was left in place for 10 days. On subsequent outpatient follow-up at 3 weeks postoperatively, the drain output decreased to zero and was removed. An MRI demonstrated resolution of the perinephric fluid collection (Fig. 2b).
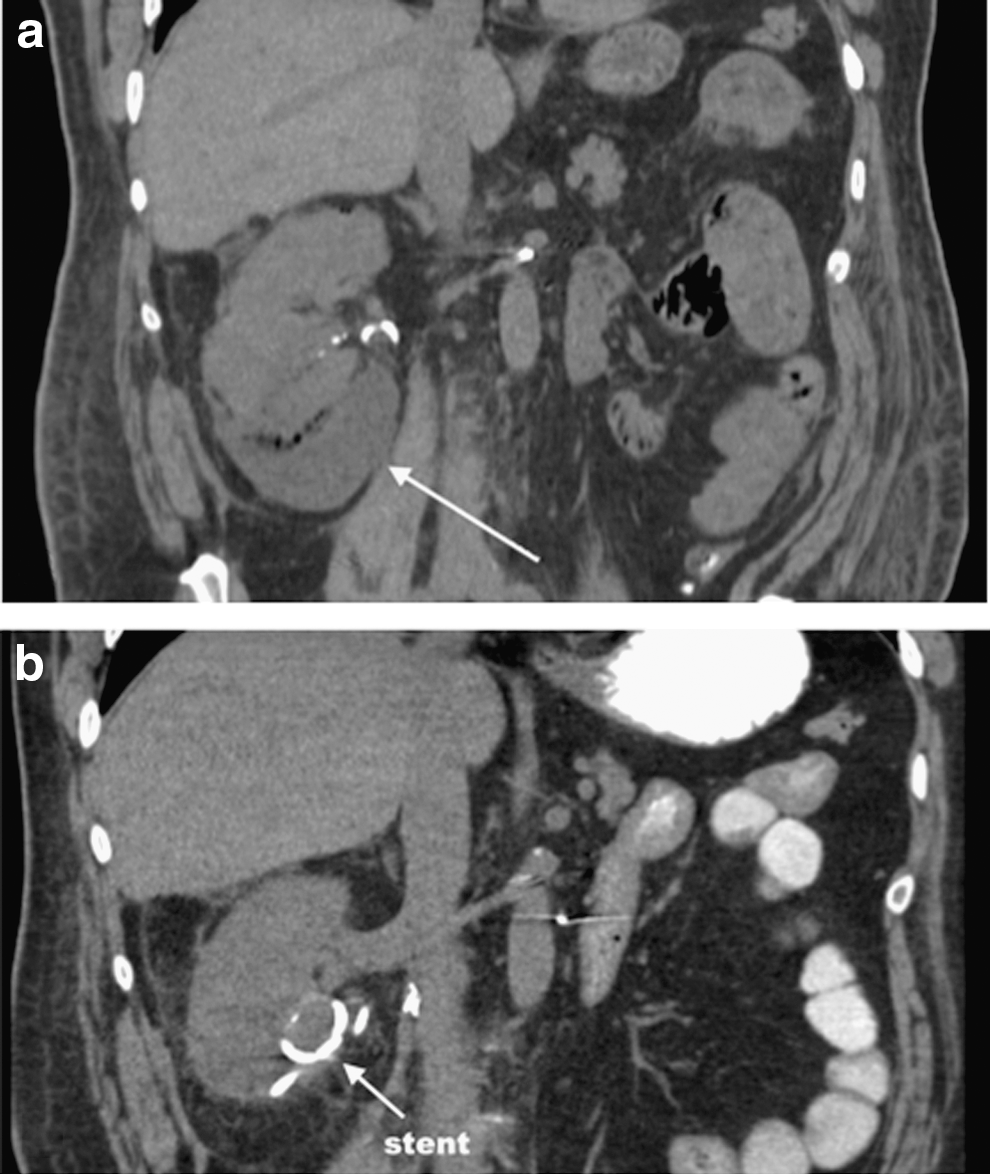
Nonenhanced MRI T2-weighted images:
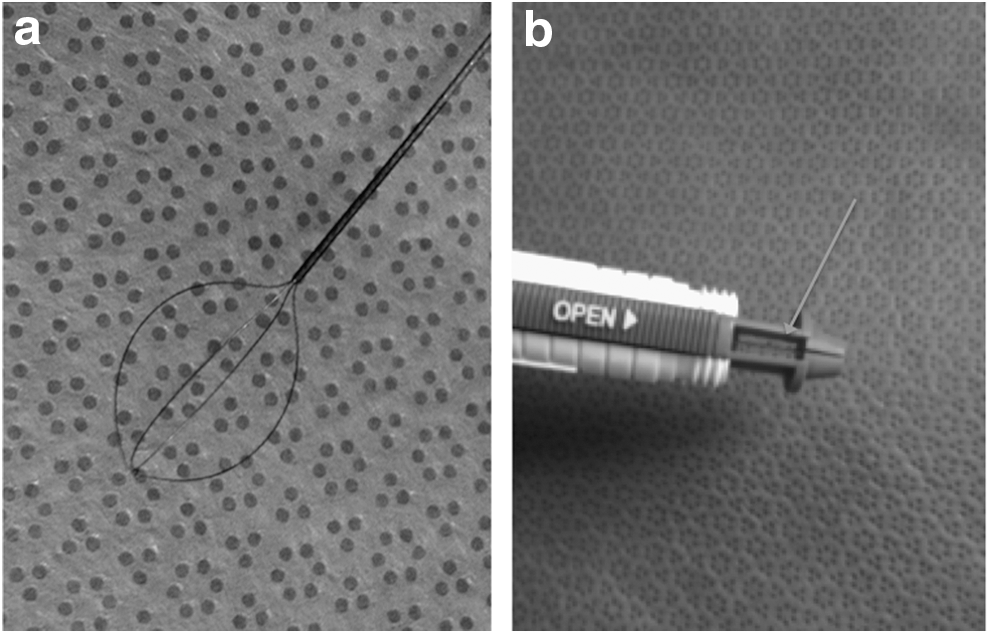
Boston Scientific 1.9F zero tip nitinol stone retrieval basket:
Discussion
PN has become the standard of care for the surgical management of most small- to intermediate-sized renal masses. 12,13 One of the potential technical problems when utilizing this more complex reconstructive approach, however, is urine leak. A higher RENAL nephrometry score has been associated with an increased risk of urine leak. Bruner et al. 14 noted after PN a 35% increased risk of leak for each unit increase in the RENAL score. This complication typically resolves with conservative management. These measures include maintaining a low-pressure system with a Foley catheter, facilitating antegrade urine flow into the bladder with a ureteral stent(s), diverting urine with a nephrostomy tube, and often placement of a percutaneous drain. 2 A drain inadvertently placed too close to the repair may perpetuate the fistula, especially if the drain is on suction. Withdrawal of the tip of the drain away from the leak site or taking the drain off suction may alleviate this problem. In this particular case, we believe that the most likely factor associated with persistent leak was the large tumor size with major collecting system entry and repair; this is the most commonly associated variable in most reports. 2,15 While it is common to prophylactically place a ureteral stent for more complex PNs, we are not familiar with any strong evidence to support this routine practice. In the present case (involving a solitary kidney), a stent was placed at the time of surgery, which did not prevent this complication from occurring.
One method of closure of urinary leaks involves plugging the tract with glue. This has been accomplished through retrograde and antegrade approaches with several different substances. French and Marcovich 6 described retrograde ureteroscopic injection of fibrin glue for closure of a persistent urine leak after PN. A similar type of polymerizing adhesive (n-butyl-2-cyanoacrylate) has also been used percutaneously. 4 Aslan et al. demonstrated the effective closure of a caliceal fistula after PN with percutaneous injection of this substance through a 0.95-mm microcatheter using a 3.3-mm introducer sheath.
Urinary fistulae can also be occluded by ablating the lining of the tract resulting in contraction and scarring down of the fistulous tract. 8 Meeks et al. employed a percutaneous antegrade ureteroscopic approach to ablate a leaky lower pole calix after PN with a holmium laser. The holmium:YAG laser delivers energy at a wavelength of 2100 nm to coagulate tissue at a depth of 0.4 mm. 16 The end result may cause contraction and welding of the tissue. 17
In the present case, we combined variations of the aforementioned concepts into a novel purely retrograde ureteroscopic technique. We utilized a ureteral access sheath from below and ureteroscopically visualized the lower pole caliceal defect. A 200-μm holmium laser fiber could not be delivered into the lower pole calix due to deflection limitations. However, we were able to effectively deploy a 1.9F nitinol stone basket into this area and transmit electrocautery to then fulgurate the calix using monopolar current. This technique allowed distribution of thermal energy over a wide surface area (Fig. 3a). Unlike the holmium laser, monopolar electrocautery is cheap, universally accessible, and more efficient. The particular characteristics of the stone basket should be carefully considered to ensure the efficacy and safety for this off-label use. Several readily available stone baskets are compatible with this technique. In the present case, we elected to use a nitinol basket from Boston Scientific that is insulated with the exception of the distal basket portion and the proximal cable seated in the handle, thereby protecting the ureteroscope and ureter from collateral thermal damage (Fig. 3b). After fulguration of the tract, we then injected fibrin glue sealant to mechanically occlude the defect. Follow-up imaging revealed resolution of the urine leak at over 13 months postoperatively.
There are inherent limitations to a case report. While the present case demonstrates resolution of a persistent leak with our novel intervention, there are obviously multiple variables at play in such a complex case. It is difficult to ascertain which aspect of our intervention was the most efficacious. Indeed, it is even possible that the urine leak could have resolved on its own with more time. However, the majority of fistulae would be expected to spontaneously seal after several months of conservative management. It should also be noted that as mentioned above, alternative thermal ablation strategies might have been equally effective, such as holmium laser or the 2F Greenwald electrode.
Urine leak after PN is a vexing problem that is occasionally refractory to conservative countermeasures. We demonstrated an effective resolution of this complication with a retrograde ureteroscopic approach employing a novel technique of caliceal fulguration and injection of fibrin glue.
Footnotes
Disclosure Statement
No competing financial interests exist.