
Abstract
Purpose:
To investigate how prone and supine redistribution of a patient's adipose tissue affects the distance from skin to the renal collecting system.
Methods:
There were 48 patients who underwent CT intravenous urography with both supine and prone scans. The distance between skin and the posterior lower pole calix was measured in both positions. The difference was calculated using paired t tests. Subgroup analyses were conducted for patients with a body mass index (BMI) ≥28 and BMI ≥30.
Results:
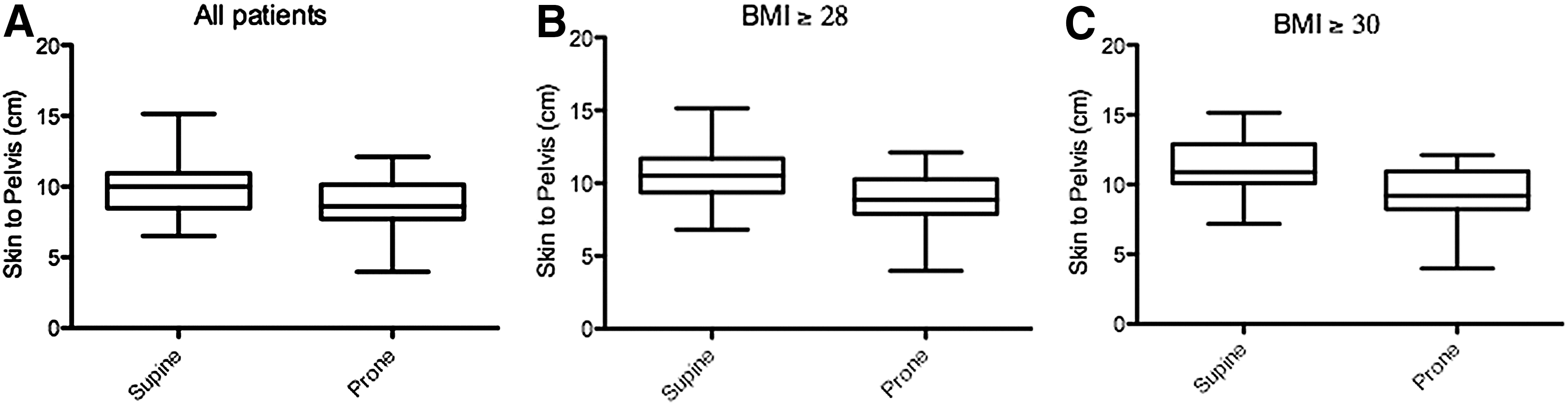
In all patients, the mean distance between skin and the posterior lower pole calix was 9.9±0.3 cm and 8.7±0.3 cm for patients supine and prone, respectively (P<0.01). Patients with a BMI≥28 had a mean distance of 10.6±0.3 cm and 8.8±0.3 cm in supine and prone positions, respectively (P<0.01), while patients with BMI≥30 had a mean distance of 11.3±0.3 cm and 9.3±0.3 cm (P<0.01). Three patients had a BMI>39 and exhibited differences in skin to the posterior lower pole calix ≥3.2 cm between supine and prone positioning. Coefficient of determination analysis for supine minus prone tract length yielded R2=0.70895.
Conclusion:
The distance between skin and the renal collecting system is decreased in the prone position when compared with the supine position. This difference increases with the patient's BMI and is further accentuated in morbidly obese patients. In these obese patients, the difference when lying prone can exceed >4 cm.
Introduction
T
Given this discrepancy, there has been a renewed effort to understand the anatomic differences between the two positions so as to investigate the stratification of patients into cohorts that could be differentially positioned. Thus, two recent studies 15,16 investigated the anatomic changes of differential positioning using imaging modalities and found that access tract length is shorter in the prone position. Specifically, Duty and colleagues 15 found that the prone position is associated with a shorter nephrostomy tract length and allows for more potential access sites. Furthermore, the study by Yazici and associates 16 found that when the subcutaneous tissue length was subtracted from the whole tract length, there was no longer a significant difference in tract length between the positions, which indicates the effect that body mass index (BMI) can have on retroperitoneal anatomy. Mazzucchi and coworkers 17 investigated obese patient outcomes in the two surgical positions but did not specifically analyze tract length. A recently proposed classification system 18 that incorporates tract length as one of five major parameters for PCNL prediction underscores the importance of this anatomy for this procedure.
In the current era of the obesity epidemic, it is common to encounter patients with a high BMI. Thus, it is important to know the distance between the renal collecting system and skin to have proper surgical planning for this cohort. When a patient's BMI nears 40, the question arises as to whether the surgical procedure is technically feasible, because some of the endoscopic instruments may not be able to reach the collecting system. To our knowledge, there are no studies that have investigated nephrostomy tract length in relation to the patient's BMI. We hypothesize that the redistribution of a patient's adipose tissue will lead to a decreased distance from skin to the collecting system when the patient is in the prone position.
Methods
We performed a single-institution retrospective chart review of all patients who presented with hematuria to the Upstate Urology Clinic and underwent CT intravenous urography CT IVU) in 2010. During 2010, it was common practice for the Upstate University Hospital's radiology department to perform CT IVU with patients in both the supine and prone position per a separate protocol. As such, there was no specific indication for prone and supine imaging. Of these patients presenting to the Clinic, 48 were identified who received a CT IVU with both supine and prone position images. The scans obtained were noncontrast, nephrogenic, and delayed excretory phase (IVU). The supine measurement was taken in the noncontrast phase, whereas the prone measurement was taken from the IVU phase.
As illustrated in Figure 1, the distance between skin and the lower pole calix was measured using axial images, following the methodology of previous studies. 19 Nephrostomy tract length was measured from epidermal edge to the medial area of the lower calix bilaterally. Tract lengths for both kidneys (96 data points) were measured and then averaged yielding 48 total data points. The difference in mean tract length for both body positions was calculated. Statistical analysis, using GraphPad Prism® software, of paired t tests was conducted for supine versus prone tract length. Further subgroup analyses were conducted for patients with BMI≥28 and BMI≥30.
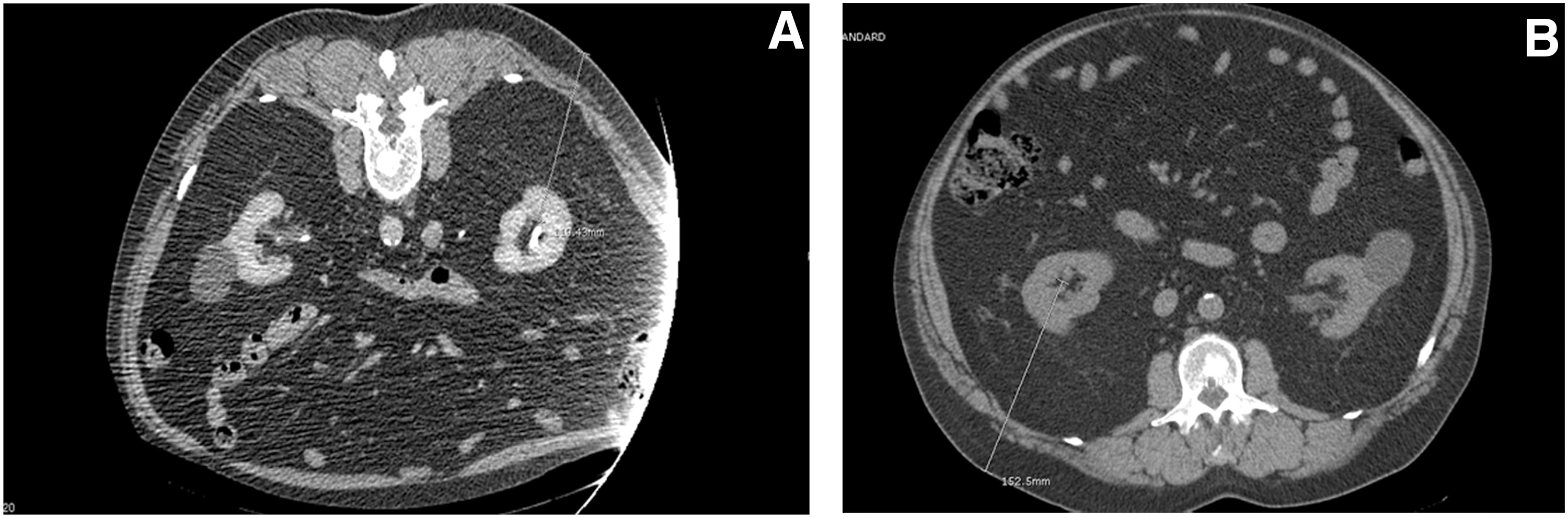
Sample measurement of a patient with body mass index=40 in both prone (
Results
Patient demographics
Forty-eight patients were included in this study: 37 male and 11 female. Mean BMI was 27.6 kg/m2 with a range of 16.5 to 40.0 for all patients. Of the total cohort, 16/48 (30%) met Centers for Disease Control and Prevention criteria for obesity (BMI≥30 mg kg/m2). In men, mean BMI was 28.1, and in women, mean BMI was 26.1. No other renal pathology was noted on CT scans that would have caused anatomic confounding of our data.
Example measurement images are shown in Figure 1. Table 1 summarizes supine versus prone mean nephrostomy tract length for 48 patients with additional stratification by BMI. In all patients, the mean distance between skin and renal pelvis was 9.9±0.3 cm and 8.7±0.3 cm for patients supine and prone, respectively (P<0.01). Patients with a BMI≥28 had a mean distance of 10.6±0.3 cm and 8.8±0.3 cm in supine and prone positions, respectively (P<0.01). Furthermore, patients with BMI≥30 had a mean distance of 11.3±0.3 cm and 9.3±0.3 cm, in supine and prone positions, respectively (P<0.01). Three patients had a BMI>39 and exhibited differences in skin to renal pelvis≥3.2 cm between supine and prone positioning. These data are graphically represented in Figure 2, with the additional subanalysis of patients by BMI stratification.
Mean nephrostomy tract length in supine vs prone position. Differential nephrostomy tract length in the (
CI=confidence interval.
Figure 3 demonstrates a coefficient of determination analysis for supine minus prone nephrostomy tract length as a function of BMI. The coefficient of determination is the portion of the total variation in the nephrostomy tract length that is explained by variation in BMI. Analysis yields an R2=0.70895

Coefficient of determination analysis for effect of percutaneous nephrolithotomy position on nephrostomy tract length.
Discussion
There has been much investigation into patient outcomes and anatomic changes associated with differential positioning of patients undergoing PCNL. The purpose of our study was to investigate nephrostomy tract length changes in supine and prone positions and to analyze the effect of BMI on tract length alteration. Our hypothesis was that the prone position will cause a redistribution of a patient's adipose tissue and will lead to a decreased tract distance from skin to the collecting system. As seen in Table 1 and Figure 2, we found that nephrostomy tract length was significantly shorter in the prone position versus the supine (8.7 cm vs 9.9 cm, P<0.01), and this difference was further accentuated by subgroup analysis of the obese cohort (11.3 cm vs 9.3 cm, P<0.01). Three patients had BMI>39 and exhibited differences in skin to renal pelvis ≥3.2 cm between supine and prone positioning. Furthermore, regression analysis determined that most of the variation in tract length is explained by variation in BMI (R2=0.70895). As a result, the larger a patient's BMI, the greater the effect on the difference in nephrostomy tract length between supine and prone positioning.
The length of the nephrostomy tract is important for three main reasons. First, having a longer tract means there is less maneuverability for the surgeon, which in turn makes the procedure more difficult and can decrease the stone-free rate. Second, there may be more surgical complications such as bowel injury or bleeding from trauma to the kidney because of torquing on the renal parenchyma given larger patient body habitus. Finally, such technical difficulties can lead to increased necessity of expensive and hard to obtain equipment for the surgeon.
There are numerous studies that support our findings. Duty and colleagues 15 found that in 20 patients who underwent prone and supine CT, the prone nephrostomy tract length was on average shorter (2.6 cm for right and 1.8 cm for left). Of note, the average BMI in this cohort was 29.5. In addition, Yazici and associates 16 investigated anatomic changes in prone and supine positioning on CT of 30 patients. Their analysis yielded a mean access tract length for the lower, middle, and upper calices that was significantly shorter in the prone position. An interesting aspect of their data is that when subcutaneous tissue was subtracted from the whole tract length, there was no longer a difference between the positions. They concluded that the difference in tract length was solely reliant on subcutaneous tissues. There was no information of the mean BMI for this cohort. In contrast, Mazzucchi and coworkers 17 in 2012 found that outcomes for 42 patients who underwent prone and supine PCNL were similar, with the additional benefit of having a shorter operative time and hospital stay with supine positioning. This study, however, only analyzed patient outcomes and did not address anatomy. A more recent study by Kamphuis and coworkers 20 found longer operative time and lower stone-free rate for supine PCNL. Our study is beneficial in that we demonstrate a decrease in tract length in the prone position as a function of BMI. Thus, the traditional prone PCNL may be easier and more feasible in obese patients without the need for a more difficult and complex surgical approach as in supine PCNL.
Our study has a number of limitations. We do not have outcome data such as stone-free rates, complication rates, or mean operative times because these patients were not presenting with stone complaints and did not necessarily have any procedures. This study is also limited given its retrospective nature and the relatively small sample size. Other factors were not analyzed, such as access angle or degree of kidney displacement. Our study, however, is the first to our knowledge that investigates the anatomic changes in access length while specifically questioning the role of BMI. Given the difficulties in performing PNCL in obese patients, we propose that the distance gained by prone positioning is significant enough to make a surgical procedure that was originally considered not technically possible to be feasible. When the urologist is conducting presurgical planning, it may be beneficial to order a CT scan performed with the patient in the prone position, particularly in obese patients.
Conclusion
The distance between the renal pelvis and skin decreases in the prone position when compared with supine. This difference increases with the patient's BMI and is further accentuated in morbidly obese patients. A preoperative CT scan in the prone position should be considered before PCNL in morbidly obese persons because this may alter surgical management.
Footnotes
Author Disclosure Statement
No competing financial interests exist.