
Abstract
Background:
There are several positions in the operation of percutaneous nephrolithotomy (PCNL), such as prone position, supine position, flank position, and modified supine position for PCNL, but the supine and prone positions are the main two choices for several years. However, there is still discrepancy on the optimal position for PCNL. Therefore, we performed this meta-analysis to evaluate safety and efficacy of the supine versus the prone position in PCNL for renal calculi.
Methods:
We searched MEDLINE, SCOPUS, and the Cochrane database libraries to look for relevant studies. All eligible controlled trials comparing supine versus prone positions for treating renal calculi were included in the meta-analysis. The main outcome of efficacy (stone-free rate, mean operative time, and hospitalization time) and safety (complication, blood transfusions) were assessed by using Review Manager 4.2 software. We calculated the estimate of effect associated with the two positions according to the heterogeneity using random-effects or fixed-effects models.
Results:
Thirteen studies (six randomized controlled trials and seven retrospective studies) with a total of 6881 patients contributed to this meta-analysis. The meta-analysis indicated/suggested that PCNL in the prone position was associated with a higher rate of stone clearance than PCNL in the supine position (odds ratio [OR]: 0.74; 95% confidence interval [CI]: 0.65, 0.84; p < 0.00001). A shorter mean operative time was observed in the supine groups (weighted mean difference [WMD]: −18.27; 95% CI: −35.77, −0.77; p = 0.04). Compared with the prone position, there was also a lower incidence of blood transfusions in the supine groups (WMD: 0.73; 95% CI: 0.56, 0.95; p = 0.02). No difference was observed between the positions with regard to the hospital stay (WMD: −0.14; 95% CI: −0.76, 0.47; p = 0.65) and complications (OR: 0.88; 95% CI: 0.76, 1.02; p = 0.10).
Conclusion:
Compared with the prone position, the PCNL in the supine position has a slightly lower rate of stone clearance, albeit shorter mean operative time, and lower incidence of blood transfusions. The meta-analysis suggests that the PCNL in the supine position is a promising alternative.
Introduction
M
PCNL has been operated in the prone position under fluoroscopic or ultrasonic guidance for decades. The prone position makes the identification of renal anatomy and the selection of the appropriate puncture point easier. It also provides a wider surface area for percutaneous access with a low risk of abdominal visceral injuries. This technique has been widely practiced by endourologists with proficiency. However, operating in the prone position has many disadvantages: Abdominal pressure decreases lung volume, thus reducing the ability for patients to tolerate prolonged surgery and requiring higher airway pressures to ensure adequate ventilation. High ventilation pressure can impair the venous return and may lead to cardiopulmonary complications, especially in obese patients and in patients with cardiopulmonary disease. 2 Furthermore, general anesthesia and ureteral catheterization are usually needed in the supine position. These necessitate position change from the supine position to the prone position after the induction of general anesthesia and retrograde ureteral catheterization. 2,3
The supine position has been developed to solve these drawbacks and to simplify the process. Compared with the prone position, the supine position in PCNL has several advantages: Cardiovascular and respiratory risks are diminished. It is easier and safer for the anesthesiologist to manage the patient and may even lessen the amount of anesthetics required. In many situations, there is no need to reposition the patient and the disinfection and the operation can be accomplished in one sequence for the surgeon who used the traditional scope in the operation of PCNL. 2,3 Furthermore, the downward slope of the PCNL access sheath allows passive egress of irrigation fluid and stone fragments by gravitational pull. This position also permits simultaneous ureteroscopic access when necessary in the management of complex stone diseases. However, disadvantages also exist with the supine position. It has limited surface area for puncture, and there is more depth between the skin and the kidney than in the prone position. These disadvantages may increase the possibility of visceral injuries and trauma to the intrarenal vessels. 4 –6 The debate over which is the better position for PCNL continues. The aim of this meta-analysis is to evaluate the safety and efficacy of the supine versus the prone position in PCNL for renal calculi.
Materials and Methods
Search strategy and eligibility and exclusion criteria
All eligible studies were retrieved from MEDLINE, SCOPUS, and the Cochrane database libraries. The following search terms were employed without any limitation: “Supine position,” “Prone position,” and “Percutaneous nephrolithotomy or PCNL.” We also manually screened the reference lists of the related studies and relevant review articles. The following trials were considered eligible for inclusion in this study: (1) patients with renal or upper ureteral stones, (2) patients were treated with PCNL in supine or prone position, (3) outcomes, including the efficacy (stone-free rate, mean operative time, and hospitalization time) and safety (complications, blood transfusions) of the PCNL, and (4) randomized controlled trials (RCTs) involving comparative studies and case series studies. Exclusion criteria were: (1) renal abnormalities (such as whole horseshoe kidney and ectopic kidney), (2) pediatric patients, (3) unclear position for the PCNL, and (4) provision of insufficient data. The details of the systematic search and selection strategy are shown in Figure 1.
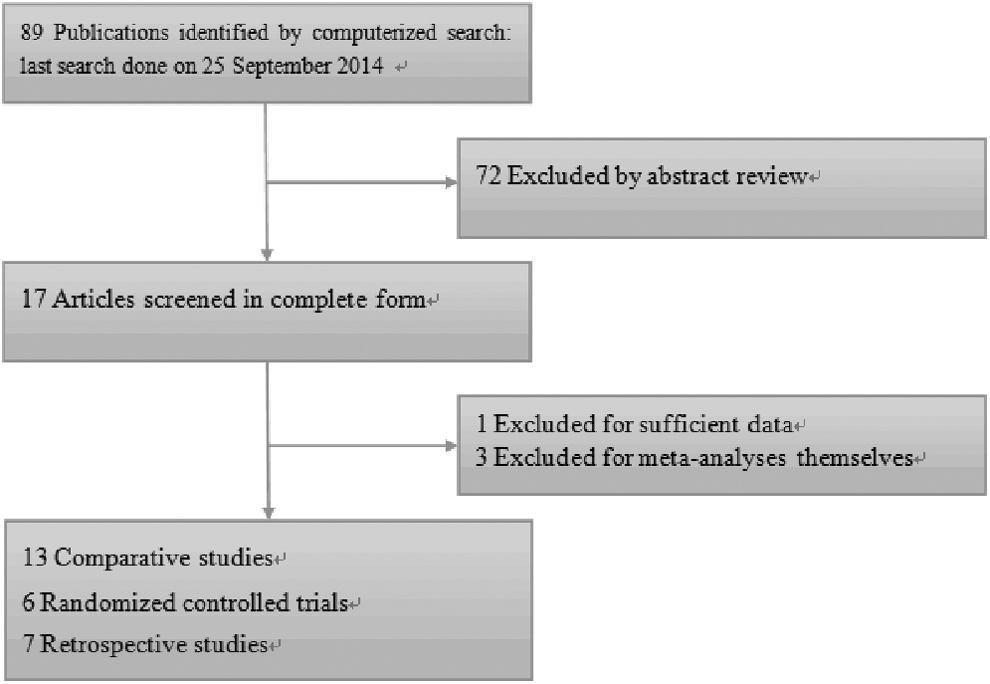
Computerized search and selection strategy.
Data extraction and quality assessment
Data pertaining to the following variables were independently extracted for each study by two authors using a standardized data extraction form: authors, year of publication, source journal, sample size, the patients' characteristics, stone-free rate (the stone-free rate was defined as either no residual stone or a clinically insignificant residual stone fragment of <4 mm in diameter and that is non-obstructive and non-infected), the mean operative time (operative time was defined as the time from the ureteral catheterization to the placement of the nephrostomy tube), complication rates, blood transfusions, and hospital stay. In duplicate studies, only the most recent data were included. The primary endpoint in the studies was the stone-free rate. The secondary endpoint was complications that included fever, urinary leakage, adjacent organ injuries (mainly colonic and pleural injury), mean operative time, and length of hospital stay. The star scoring system 7 was used to evaluate methodological quality of the included studies, which was based on the criteria related to the study design, comparability of the patient groups, and the outcome assessment to assess the literature quality. The total score was 9 stars, and the quality of each study was graded as lower (0–5 stars) or higher (6–9 stars).
Statistical analysis
The weighted mean differences (WMDs) were used for continuous outcomes, and odds ratios (ORs) were used for the dichotomous outcomes. The summary risk estimates were calculated using random-effects or fixed-effects models, as appropriate, based on heterogeneity levels. 8 Heterogeneity among studies was assessed using the I 2 statistic, which measured quantitative inconsistency in heterogeneity levels across studies. Studies with I 2 values from 25% to 50% exhibited low heterogeneity, 50% to 75% showed moderate heterogeneity, and studies with results >75% exhibited high heterogeneity. An I 2 value >50% and pheterogeneity >0.10 indicated significant heterogeneity. All statistical analyses were conducted using Review Manager version 4.2 software (Cochrane Collaboration, Copenhagen, Denmark).
Results
Characteristics of included studies
Following the search strategy and inclusion criteria, the initial search identified 89 citations, of which 13 studies 9 –21 (6 RCTs 9,10,12,16,18,21 and 7 retrospective studies 11,13 –15,17,19,20 ) were included in this meta-analysis with a total of 5881 patients (1703 in the supine group and 5178 in the prone group). The main characteristics of the 13 studies are shown in Table 1. Table 2 shows the quality assessment of individual studies that have a score of >6 points, with the exception of Shoma et al., 20 whose score was 5 points.
BMI = body mass index; NA = not available; RCT = randomized controlled trial; RNT = retrospective nonrandomized trial.
Selection for treatment: 1 = inclusion criteria reported; 2 = generalizability of patients undergoing surgery in supine position to population undergoing surgery for kidney calculi; 3 = generalizability of patients undergoing surgery in prone position to population undergoing surgery for kidney calculi. Comparability between groups (if yes to all, 2 stars; if one of these characteristics was not reported, 1 star; if the two groups differed, no stars): 4 = age, sex, and body mass index; 5 = stone location, stone burden, and site of puncture. Outcome assessment: 6 = more than 5 outcomes of interested clearly recorded (1 star); 7 = adequacy of follow-up (1 star if follow-up is 0.90%).
Stone-free rate
All 13 studies 9 –21 included data on stone-free rate. We used the fixed-effects model to combine these data, because heterogeneity was not evident (p = 0.46). The stone-free rate was 77.7% (4025/5178) in the prone position versus 74.3% (1266/1703) in the supine position. In the overall data, the stone-free rate was higher in the prone position than in the supine position (OR: 0.74; 95% confidence interval [CI]: 0.65, 0.84; p < 0.00001, Fig. 2).
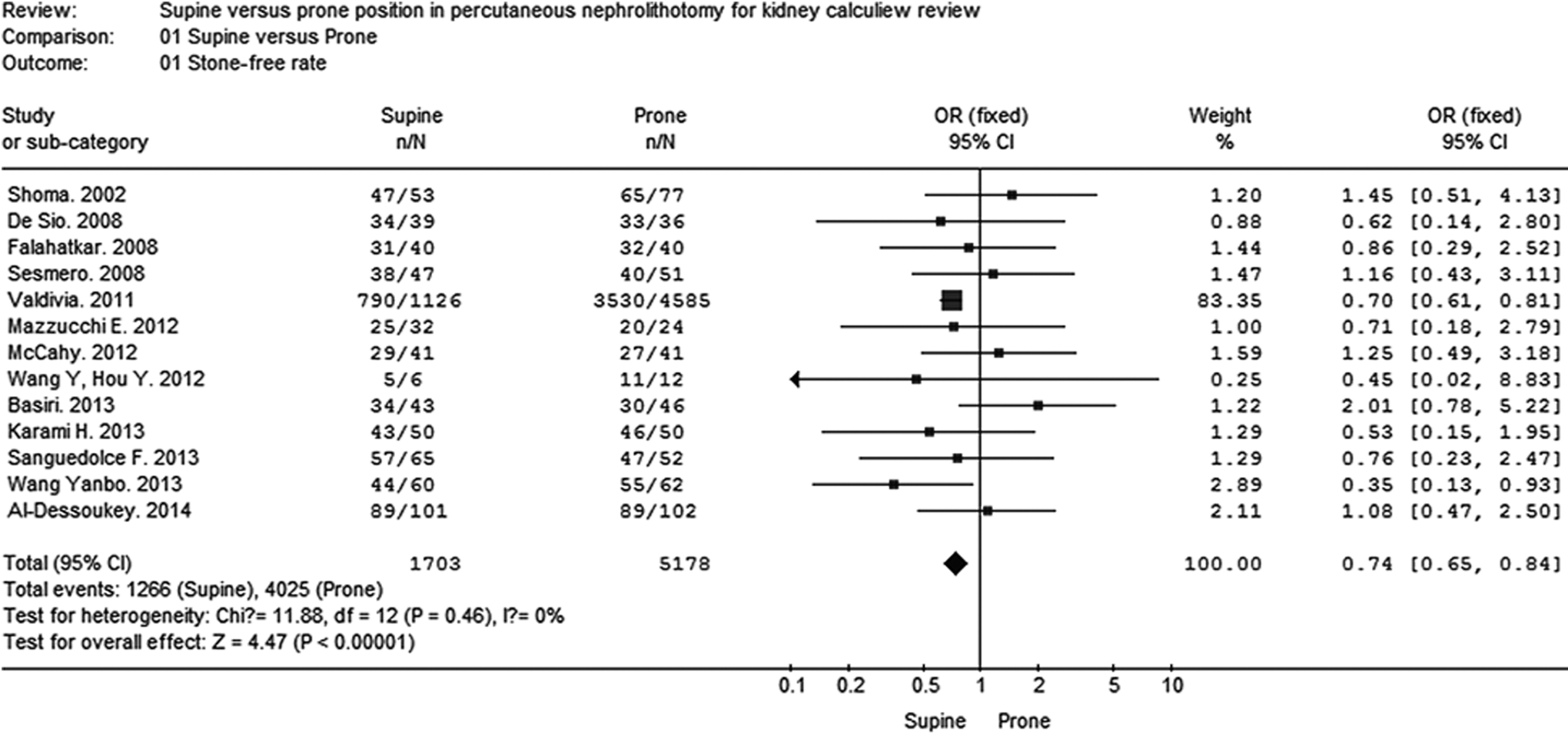
Forest plot showing stone-free rate between supine and prone positions.
Mean operative time
Six studies, 9,11,16 –19 including 6274 patients, reported the mean operative time for PCNL in two positions. We used the random-effects model to combine the data due to notable heterogeneity (p < 0.00001). Compared with the prone position in PCNL, operative time in the supine position was less (WMD: −18.27; 95% CI: −35.77, −0.77; p = 0.04, Fig. 3).
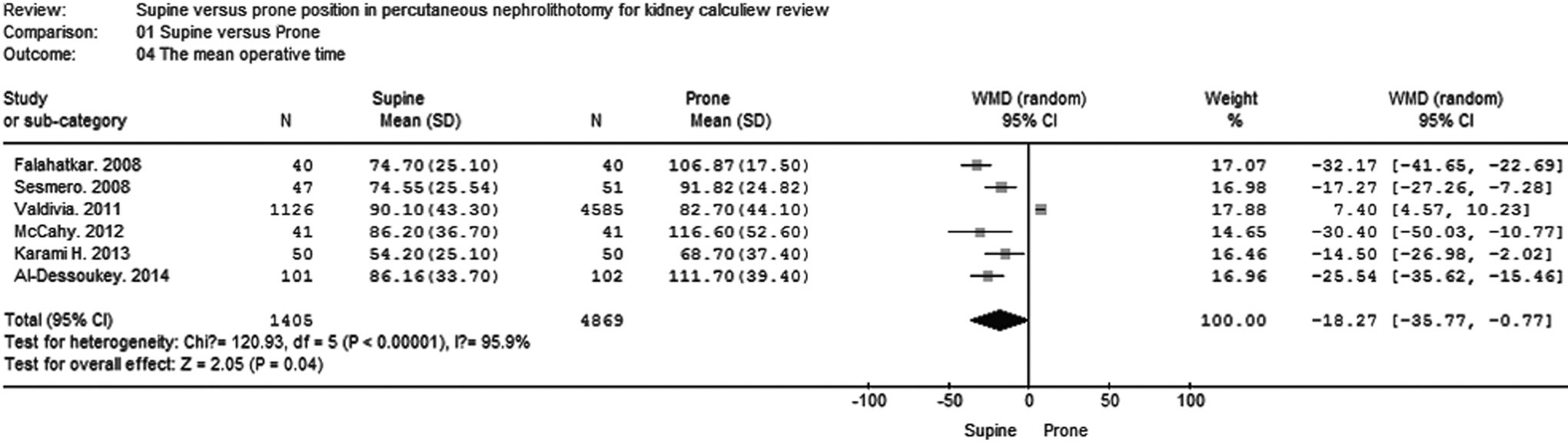
Forest plot showing the operative time between supine and prone positions.
Length of hospitalization
Six studies, 9,11,16 –19 including 6264 patients, reported the length of hospital stay for PCNL in two positions. The random-effects model was used to combine the data owing to notable heterogeneity (p < 0.00001). In the combined data, this model showed no significant difference between the supine position and the prone position with regard to hospitalization time (WMD: −0.14; 95% CI: −0.76, 0.47; p = 0.65, Fig. 4).
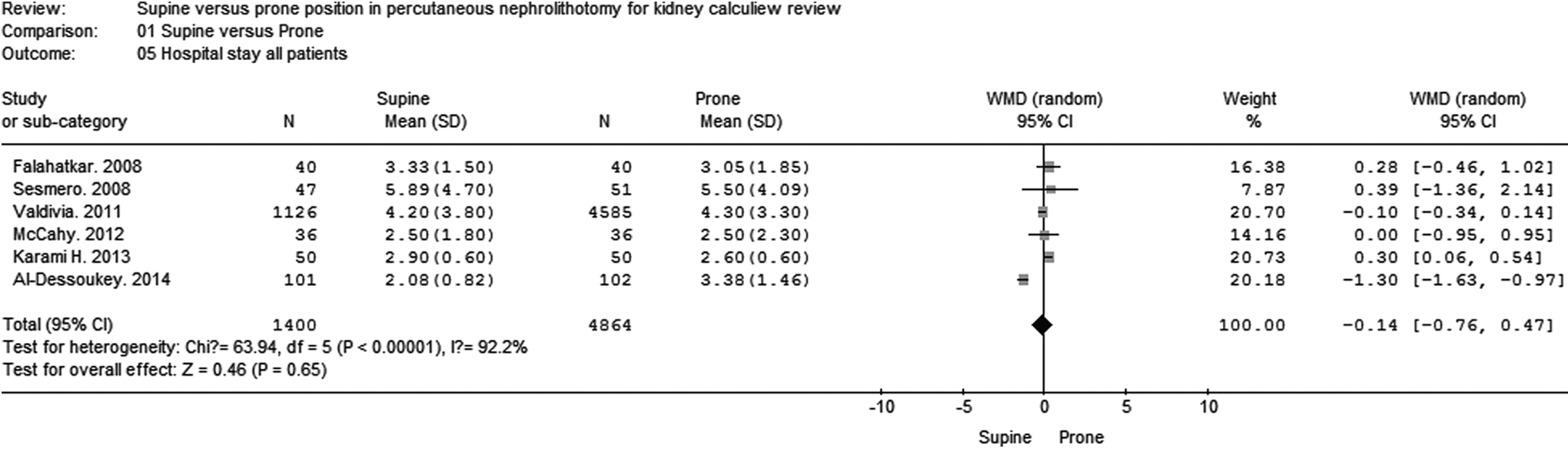
Forest plot showing hospital stay between supine and prone positions.
Complication rate
Data on postoperative complications, including fever, 9,10,12,13,15 –18,20 urinary leakage, 9,15,18 –21 organs injury, 9,16,17 pleural effusion, 9,14,15,17 bleeding, 10,20,21 renal colic, 10,21 urinoma, 14 arteriovenous fistula, 14,19 septicaemia, 14,19 and hyponatremia, 15 were collected and analyzed. Due to lower heterogeneity (p = 0.33), the fixed-effects model was used to pool the data. The complication rate was 20.5% (1058/5161) in the prone position versus 18.1% (307/1696) in the supine position. Pooled data showed similar overall complication rates in both supine and prone groups (OR: 0.88; 95% CI: 0.76, 1.02; p = 0.10, Fig. 5), and specifically in urinary leakage (OR: 1.06; 95% CI: 0.64, 2.44; p = 0.89, Fig. 6) and pleural effusion (OR: 0.76; 95% CI: 0.46, 1.25; p = 0.28, Fig. 7). However, the rates for fever were significantly lower in the supine group than in the prone group (OR: 0.64; 95% CI: 0.51, 0.79; p < 0.0001, Fig. 8).
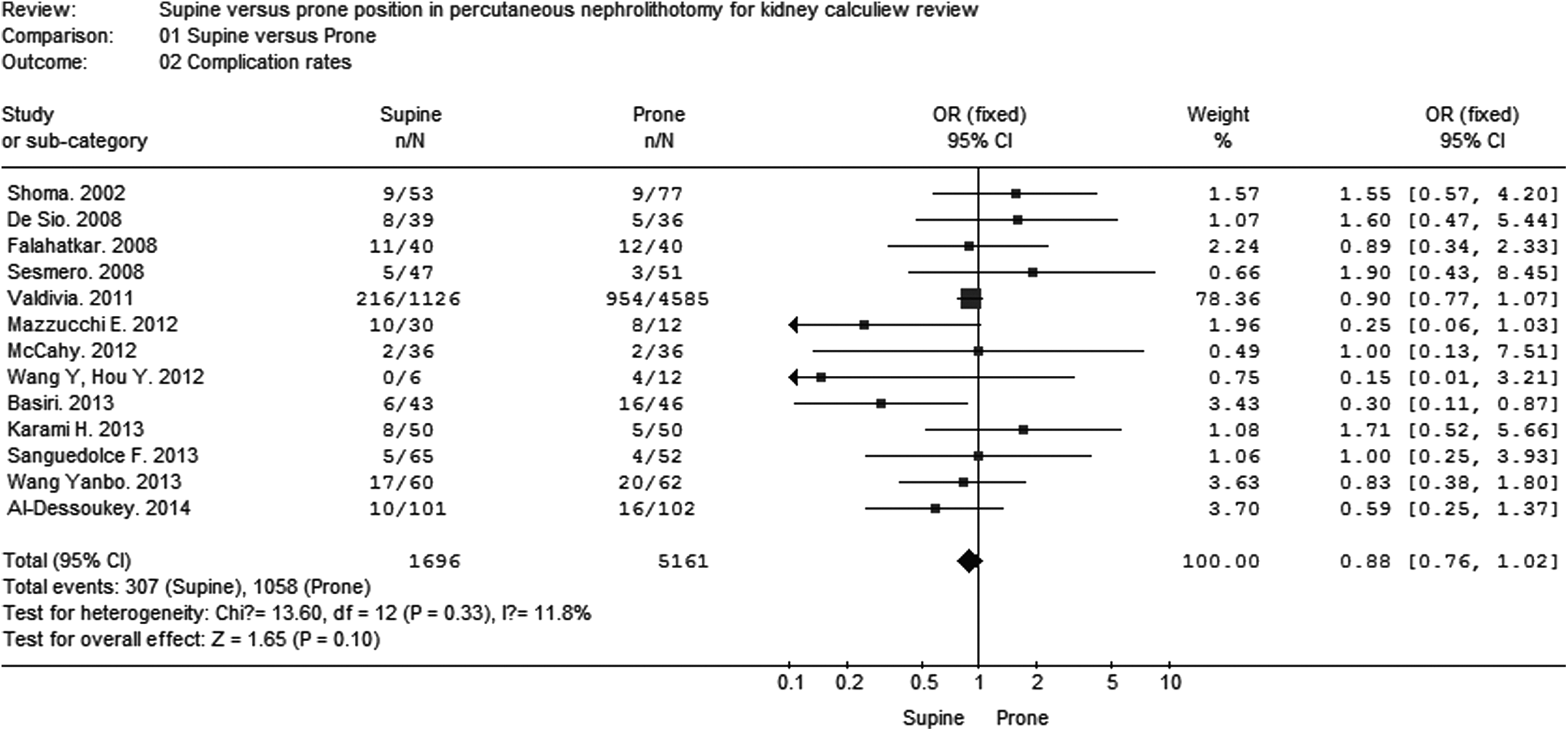
Forest plot showing complication rate between supine and prone positions.
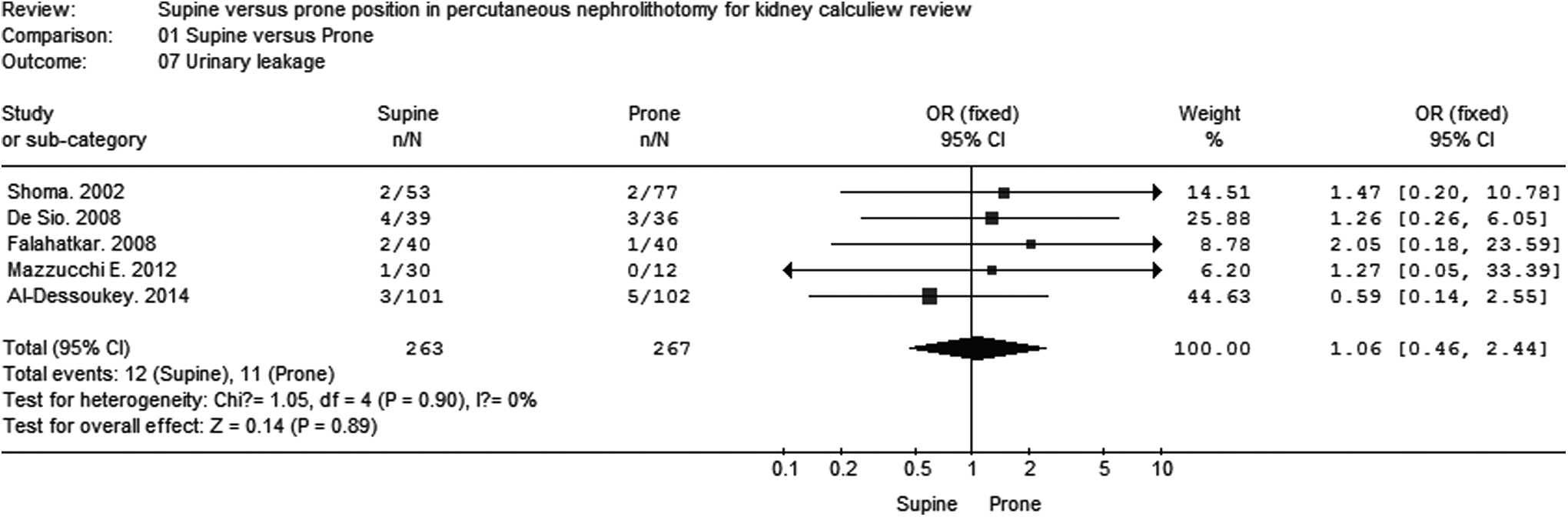
Forest plot showing urinary leakage between supine and prone positions.

Forest plot showing pleural effusion between supine and prone positions.
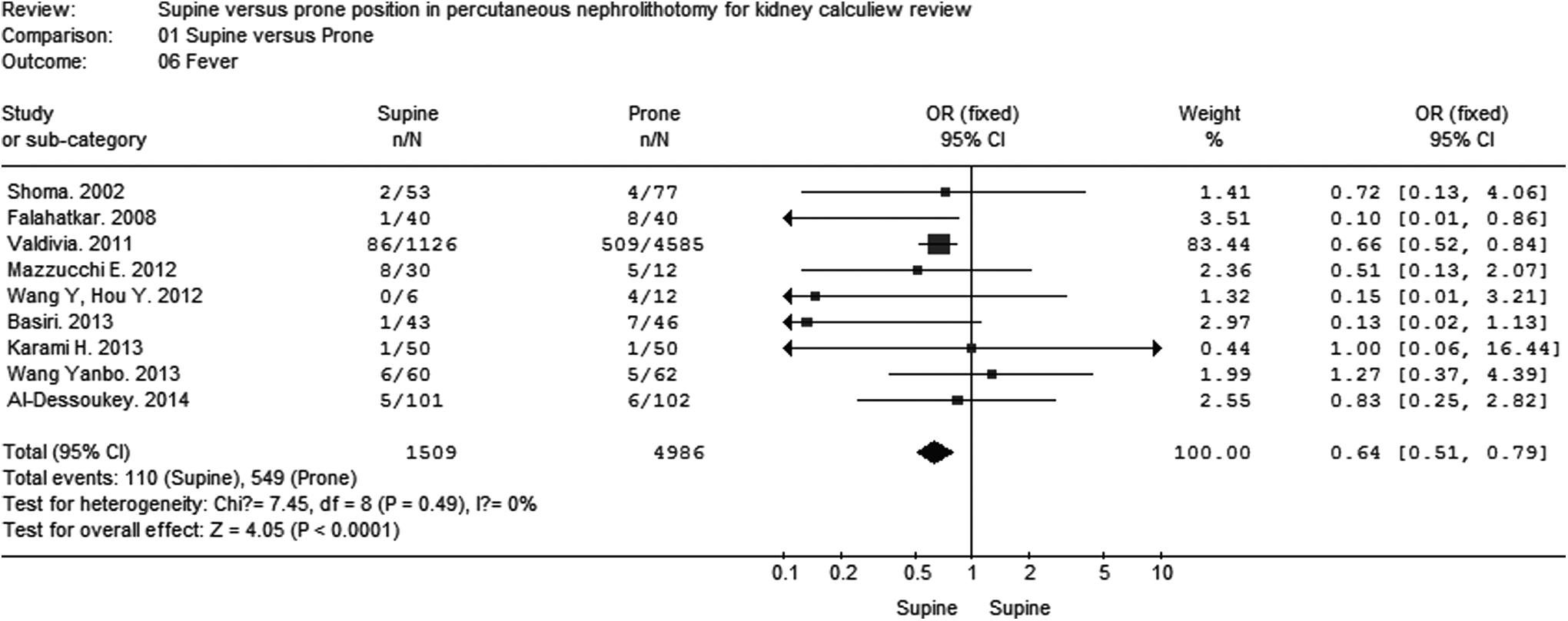
Forest plot showing fever between supine and prone positions.
Blood transfusions
Nine studies, 9,11,12,14 –20 including 6512 patients, reported the blood transfusion rate for PCNL in both positions. Owing to lower heterogeneity (p = 0.09), we used the fixed-effects model to combine the data. Meta-analysis demonstrated lower blood transfusions in the supine position than in the prone position (WMD: 0.73; 95% CI: 0.56, 0.95; p = 0.02, Fig. 9).
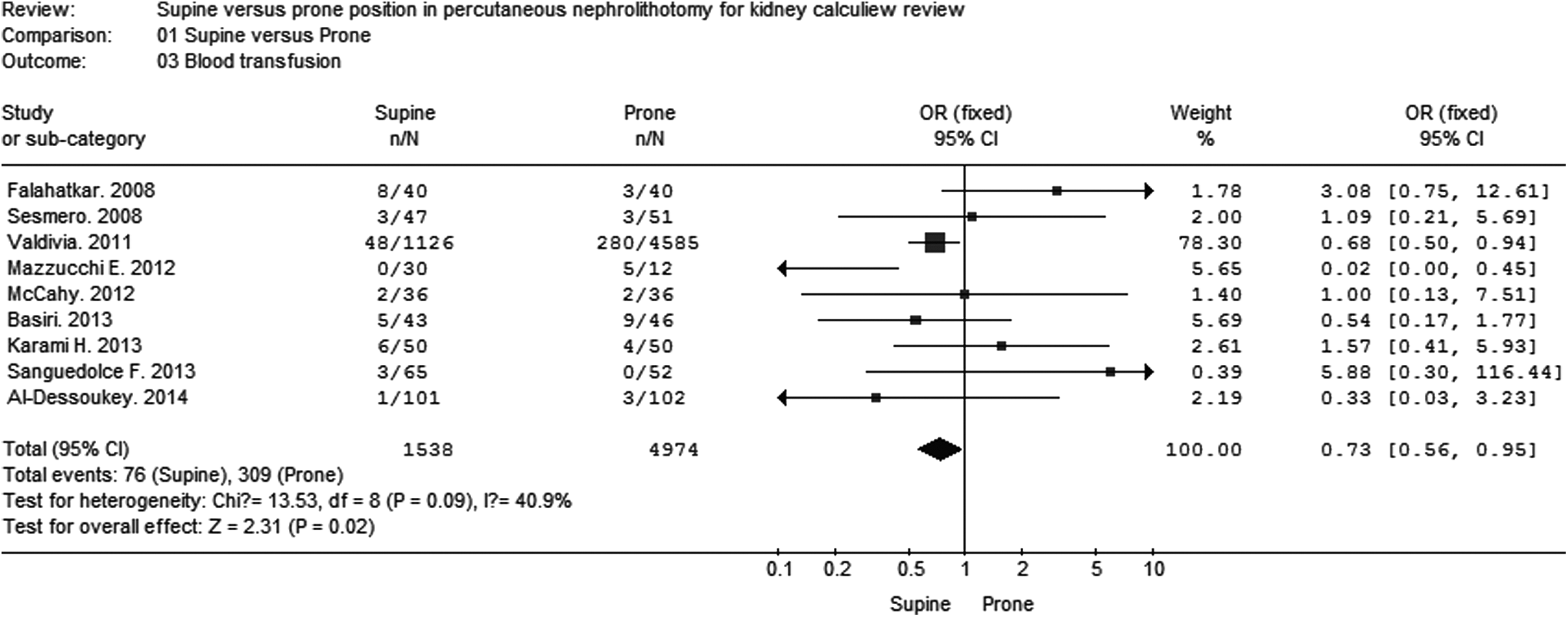
Forest plot showing blood transfusion between supine and prone positions.
Assessment of publication bias
We assessed potential publication bias using a funnel plot. The funnel plot shapes for the meta-analysis of stone-free rate, complication rate, and blood transfusion rate show nearly symmetry (Fig. 10). Hence, we did not detect the publication bias in this meta-analysis.
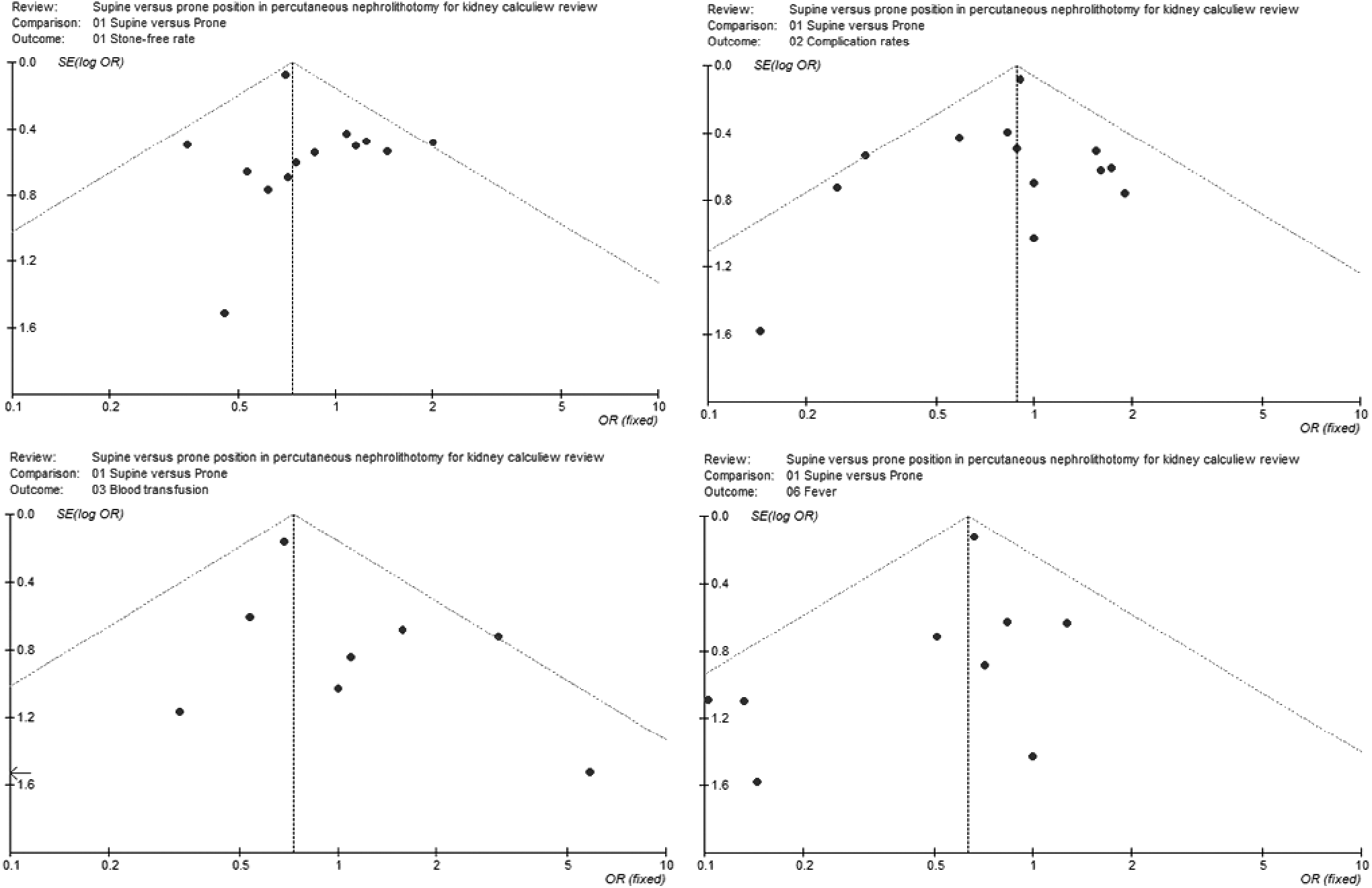
Funnel plot for the results from all studies comparing stone-free rate, complication rate (fever), and blood transfusion in patients between supine versus prone position.
Sensitivity analyses
In sensitivity analyses, five outcomes were included. The results are shown in Table 3. This analysis suggested that the OR, the WMD, and the level of significance for the three outcomes (complication rates, the mean operative time, and hospital stay) were not obviously altered. However, the OR and the level of significance for the stone-free rate and blood transfusion were notably different in RCTs. In addition, the stone-free rate and the blood transfusion were not significantly different between two groups.
No statistically significant difference.
CI = confidence interval; supine = supine position in PCNL; prone = prone position in PCNL; PCNL = percutaneous nephrolithotomy; OR = odds ratio; WMD = weighted mean difference.
Discussion
Compared with open surgery and shock wave lithotripsy for the larger and complex stones, the PCNL in the prone position has lower morbidity and covalescence, cost. 22 It has been the preferred position for PCNL for decades. It provides a wide surface area for puncture sites and offers adequate space for nephroscopic manipulation. 23 –25 Nevertheless, it has some disadvantages. Foremost is the compromised weight distribution, a milieu that can lead to cardiopulmonary complications, especially in obese patients and individuals with cardiac diseases. It also increases the difficulty in the airway management for the anesthesiologist. The need for several assistants to reposition the patient before surgery and for additional intraoperative position changes in case of simultaneous ureteroscopy can also be problematic. The prone position may be contraindicated in some patients due to circulatory and ventilatory impairment. 26,27
In 1987, Gabriel Valdivia and colleagues described the first case of PCNL in the supine position (sPCNL). They touted several benefits for the patient, especially for those patients with higher anesthetic risk. Recently, more and more sPCNL have been reported. 28 –30 It increased the confidence for the endourologists to practice this technique and overcome the drawbacks of the prone position. However in normal healthy individuals, there is still the controversy over the efficacy and safety of operating in the supine versus the prone position in PCNL.
In this meta-analysis, we included 13 clinical studies 9 –21 that compared sPCNL with pPCNL for renal calculi to adjudicate the superior position for the treatment of kidney stones. The heterogeneity of the location and the type of calculi, as well as the different study types was overcome by sensitivity analysis of the combined data. Meanwhile, three common complications rather than the overall complication rate were selected for this meta-analysis for a better evaluation of the safety of the supine position in PCNL.
The stone-free rate in the supine group was 74.3%, and the rate for the prone group was 77.7%. This meta-analysis demonstrated that operating in the prone position was significantly better than in the supine position for the stone-free rate. This was contrary to two previous meta-analyses results, 31,32 but it was in accordance with the conclusion by Zhang et al. 33 . The reasons for the higher stone-free rate in the prone position might be due to the wider choice for the renal puncture site and more space for the manipulation of the nephroscope. In addition, in the supine position, it is more challenging to follow migratory stones, and the upper pole approach could also be more technically difficult. 3,28,31,34 Therefore, in conclusion, we believed that the stone-free rate was better achieved in the prone group.
There are only six trials 9,11,16 –19 that include hospitalization times. Our meta-analysis revealed that hospital stay was not significantly different between the supine and the prone groups, which is in accordance with/in agreement with/consistent with the findings by Zhang et al. 33 . These data lend further support to the efficiency of the supine approach.
Our meta-analysis of six clinical studies 9,11,16 –19 revealed significantly less operative time in the supine groups than in the prone groups. We attributed this mainly to not having to reposition the patient from the lithotomy to the prone position and to the repeated preparation of the operative field. Time was saved when PCNL and ureteroscopic procedures had to be performed simultaneously. Furthermore, the sensitivity analysis also supports the fact that sPCNL required less operative time than pPCNL.
The meta-analysis revealed that the blood transfusions 9,11,12,14 –20 in the supine position were significantly less than those of the prone position (This was perhaps because the kidneys are more medial and have greater mobility in the retroperitoneum with the supine position, which may reduce the need for blood transfusion.). This could likely be the result of the shorter operative time with the sPCNL.
Many complications may occur after surgery. Relatively common complications were selected in this study, which included urinary leakage, pleural effusion, and fever. The total complication rate 9 –21 in the supine group was 18.1%, whereas that in the prone group was 20.5%. Our meta-analysis showed that the total complication rate was not significantly different between these two groups. We then analyzed each of the complications individually. Urinary leakage 9,15,18,20,21 and pleural effusion 9,14,15,17 had similar complication rates between the two groups, whereas the rate of fever 9,10,12,13,15 –18,20 was significantly less in the supine group. This is possibly due to the lower respiratory stress during the supine position.
Some limitations cannot be neglected in this meta-analysis. First, the paucity of comparative studies on supine versus prone PCNL was the most significant drawback. Second, between-study heterogeneity was common in the included studies. Some series paid attention only to the different results. Others used quite a different definition for the PCNL complications. With such a high degree of heterogeneity, many of these studies would have been excluded. To explain the source of heterogeneity, we performed sensitivity analysis. Third, different surgeons might have had different experiences with sPCNL and pPCNL. Since this meta-analysis included non-randomized trials, these might have affected the studied outcomes. Therefore, further prospective, randomized, and multicenter RCTs would be needed for a more comprehensive and convincing evaluation. Fourth, different studies might have different defining criteria for the outcomes in which we were interested; these might not have been reported in the study methodology. Fifth, due to the inclusion of nonrandomized studies, there were two inherent selection biases in these two groups. Sixth, most of the surgeons who performed the sPCNL had actually switched from the pPCNL. It indicated that they were already experienced surgeons and found sPCNL to be beneficial. The surgeons' experience might have affected the studied outcomes. Finally, we could not account for the limitation of the unpublished data and the selection bias.
Conclusions
This study highlighted statistically several advantages of sPCNL over pPCNL, especially in quantifying the safety advantages. Although it was shown that the stone-free rate was somewhat lower in sPCNL, there was the distinct advantage in reducing the mean operative time and with no effect on the length of hospitalization time. Safety outcomes in the present study highlight several advantages with lower rates of blood transfusions and cases of presentation with fever, despite the lack of difference in WMD for the overall complication outcomes. However, the majority of the studies in our meta-analysis were retrospective, which might lead to some selection bias (especially with heterogeneity of complication outcomes). Therefore, to be conclusive, prospective, multicenter RCTs would be necessary.
Footnotes
Acknowledgments
The study was supported by the outstanding youth science and technology talent cultivating object of Guizhou Province in 2013 (2013-18), the young talents project of Guizhou Province in 2012 (2012-185), the National Natural Science Foundation of China (81360119), the International Scientific and Technological Cooperation Projects of Guizhou Province (20137031), and the Science and Technology Program of Guangzhou, China (2011J4100054).
Authors' Contributions
Conceived and designed the article: JianGuo Zhu, ZhaoLin Sun, and WeiDe Zhong. Literature search and data extraction: DongBo Yuan, HaoFu Rao, and TianFei Cheng. Analyzed the data: JianGuo Zhu, YuanLin Wang, WeiHong Chen, and YongDa Liu. Wrote the article: JianGuo Zhu, Jun Liu, DongBo Yuan, and YongDa Liu. All authors read and approved the final article.
Author Disclosure Statement
No competing financial interests exist.