
Abstract
Objective:
We assessed the effects of music and noise-canceling headphones (NCHs) on perceived patient pain and anxiety from extracorporeal shockwave lithotripsy (SWL).
Patients and Methods:
Patients with renal calculi scheduled for SWL were prospectively enrolled. All 89 patients between the ages of 19 and 80 years were informed about this study and then randomized into three groups: Group 1 (controls), no headphones and music; Group 2, music with NCHs (patients listened to Turkish classical music with NCHs during SWL); and Group 3, music with non-NCHs (patients listened to Turkish classical music with non-NCHs during SWL). Hemodynamic and respiratory parameters were recorded before and just after the SWL session. All patient visual analog scale (VAS) and State-Trait Anxiety Inventory (STAI) scores were recorded just after the SWL procedure.
Results:
There were significant differences in VAS scores among the groups (5.1, 3.6, and 4.5, respectively, p < 0.001), including between Groups 2 and 3 (p = 0.018). There were also significant differences in STAI-State anxiety scores among the groups (43.1, 33.5, and 38.9, respectively, p = 0.001), including between Groups 2 and 3 (p = 0.04).
Conclusions:
Music therapy during SWL reduced pain and anxiety. Music therapy with NCHs was more effective for pain and anxiety reduction. To reduce pain and anxiety, nonpharmacologic therapies such as music therapy with NCHs during SWL should be investigated further and used routinely.
Introduction
E
Music has been accepted as a nonpharmacologic alternative treatment modality for many diseases since ancient times. The use of music to promote relaxation and alleviate perceived pain has been shown to be beneficial. 4 –6 However, there are only a few publications on the effects of music in SWL in the current literature. 3,7 These studies have shown the beneficial effects of music on pain and anxiety in SWL.
Active noise-canceling headphones (NCHs) have microphones outside the headset that input external ambient noise and create new sound waves that neutralize and reduce the unwanted noises. They are most effective for sounds generated by machinery and aircraft engines. 8,9
In this study, we assessed the effects of music and NCHs on perceived patient pain and anxiety from SWL.
Patients and Methods
After obtaining institutional review board approval and patient informed consent, patients scheduled for SWL between January 2015 and August 2015 were enrolled prospectively. The patients were randomized into three groups, one by one. Only patients with radiopaque renal calculi were included. Patients who had undergone SWL treatment before, patients with ureteral stents, and those with renal colic were excluded. None of the patients were receiving any treatment for urolithiasis before entering the study. Patient demographics were recorded. All 89 patients were between the ages of 19 and 80 years. They were randomized into three groups: Group 1 (controls), no headphones and music; Group 2, music with NCHs (patients listened to Turkish classical music with NCHs during SWL; Sony MDR NC8; Sony Electronics, Inc.); and Group 3, music with non-NCHs (patients listened to Turkish classical music with non-NCHs during SWL; Sony MDR ZX100).
All patients received diclofenac 75 mg intramuscularly for analgesia. The SWL treatment was performed with an electrohydraulic device (Elmed Multimed Classic; Elmed Electronic Industry Trade Corporation) by one experienced radiographer. All patients were treated in a supine position under fluoroscopic guidance as an outpatient procedure. Each SWL treatment typically started at 12 kV and then increased incrementally to a maximum of 21 kV. We aimed to deliver 3000 shocks at a frequency of 60 Hz in each SWL session.
Hemodynamic and respiratory parameters were recorded before and just after the SWL session. A visual analog scale (VAS) was used to determine pain levels by having patients mark a point along a 0 to 10 cm line segment to indicate the severity of pain (0 = no pain, 10 = maximal possible pain). The State-Trait Anxiety Inventory (STAI) was used to assess patient anxiety levels. 10 STAI is a scale to measure the trait and state anxiety that contains two subscales of 20 multiple-choice questions each. The overall score ranges from 20 to 80; larger scores indicate greater anxiety levels. In all patients, VAS and STAI scores were recorded just after the SWL procedure. Patients in Groups 2 and 3 listened to instrumental classical Turkish music where the ney (reed flute) was the musical instrument.
Statistical analyses
The SPSS software (ver. 15.0 for Windows; SPSS, Inc.) was used for statistical analyses. The Kolmogorov–Smirnov test was used to test the normal distribution of continuous variables. Data are presented as mean ± standard deviation. To determine differences between groups, the Student's t-test and one-way ANOVA were used for variables with a normal distribution, while the Mann–Whitney U test and Kruskal–Wallis test were used for non-normal variables. Pearson's χ2 was used to test the differences by gender between the groups. p Values <0.05 were considered to indicate statistical significance.
Results
In total, 89 patients who underwent a first session of SWL were randomized prospectively into Group 1 (n = 32), Group 2 (n = 28), and Group 3 (n = 29). The mean age of the patients was 47.9 ± 1.5, and the mean stone size was 11.8 ± 4.5 mm. Patient demographic characteristics and SWL variables are presented in Table 1. There were no differences in terms of gender, age, stone size, side, given shockwaves, energy, or preprocedural hemodynamic or respiratory parameters among the groups.
Postprocedure mean pain scores, anxiety scores, and hemodynamic and respiratory parameters of patients are presented in Table 2. There were significant differences in terms of VAS scores among the groups (5.1, 3.6, and 4.5, respectively, p < 0.001). The highest VAS score was observed in Group 1 and the lowest in Group 2, although there were also significant differences between Groups 2 and 3 (p = 0.018). There were no significant differences in STAI-Trait anxiety scores among the groups (p = 0.96), but there were statistically significant differences in STAI-State anxiety scores (43.1, 33.5, and 38.9, respectively, p = 0.001), including between Groups 2 and 3 (p = 0.04). Postprocedure hemodynamic and respiratory parameters were similar among all groups.
STAI = State-Trait Anxiety Inventory; VAS = visual analog scale.
Discussion
SWL has become a routine procedure for the management of urinary stones since the initial attempt by Chaussy et al. 30 years ago. 11 SWL is an efficient noninvasive treatment modality with low morbidity for urinary tract calculi. 12 Despite the latest-generation machines, SWL is still a painful procedure and can be a distressing experience for patients during the procedure. 13,14 According to the EAU guidelines on urolithiasis, careful control of pain during SWL treatment is necessary to limit pain-induced movements and excessive respiratory excursions. Strong shockwaves can cause patients to move and then recontrol of stone localization with imaging is required. 15 Acute pain stimulates respiration and increases ventilation, which can lead to the kidney moving 2 to 4 cm. 16 Thus, SWL can become ineffective, because of not focusing exactly on the stone. Ktari et al. 17 showed that pain was correlated with anxiety scores of patients during SWL procedures. Because of the pain and anxiety, patients may not want to continue further SWL sessions.
There have been various treatment approaches for such pain and anxiety, including nonsteroidal anti-inflammatory drugs, opioids, local anesthetics, and general anesthesia. 2 However, severe side effects in the gastrointestinal system, hematopoietic system, kidneys, respiratory system, and central nervous system may occur with such medications. 18 Demir et al. 16 reported that decreasing patient anxiety was one of the most important issues when choosing an analgesic agent and emphasized the importance of adequately decreasing anxiety to provide comfort to patients for repeated sessions of SWL. However, using opioids for anxiety and analgesia may cause significant complications, such as respiratory depression, hypotension, and bradycardia. Thus, there is a need for complementary therapies to decrease such pain and anxiety. Acupuncture, transcutaneous electrical nerve stimulation, auricular acupressure, and music have been used. 19 It has been shown that music therapy reduces pain by activating the cingulofrontal cortex. 20 Music also has anxiolytic effects and it is recommended for use as a therapy in stressful interventions. Several studies have confirmed the beneficial effects of music therapy on pain and anxiety during endoscopic procedures, such as rigid-flexible cystoscopy, prostate biopsy, and colonoscopy. 4 –6,21
There are four studies in the current literature about SWL with music. The first two were published in 1998 and were about the use of opioids during SWL. In the study by Kock et al., 22 a reduction in the alfentanil requirement was found in the music group. However, Cepeda et al. 23 argued that music did not reduce the alfentanil requirement during patient-controlled analgesia use in SWL, although all patients were premedicated with morphine and ketorolac. Yilmaz et al. 7 showed lower opiate (fentanyl) requirements with music during SWL and suggested that the use of music therapy had an anxiolytic effect. 7 Our study differs from these studies in that both of these previous studies investigated the need for opioid analgesia. We did not use any opioid analgesic. All patients received only diclofenac intramuscularly before the procedure, and anxiety and pain scores were recorded just after their first session of SWL.
Akbas et al. 13 showed the efficacy of music therapy to lower anxiety and pain scores during SWL, as in our study. However, that study was carried out at three centers, and three different technicians might cause bias. In addition, they did not use NCHs.
In our study, we found that pain and anxiety scores of patients who received music therapy (Groups 2 and 3) were lower than patients who did not (Group 1). In Group 2, we used active NCHs to reduce the external disturbing noise of SWL. When we compare Groups 2 and 3 according to pain and anxiety scores, we found that these scores were statistically lower in Group 2. NCHs reduce unwanted ambient sounds using active noise control. This is distinct from passive headphones. They incorporate a microphone that measures ambient sound, generate a waveform that is the exact negative of the ambient sound, and mix it with any audio signal the listener desires 24 (Fig. 1). About 70% of ambient noise was effectively blocked by this way. In the current literature, there is no study about SWL using NCHs.
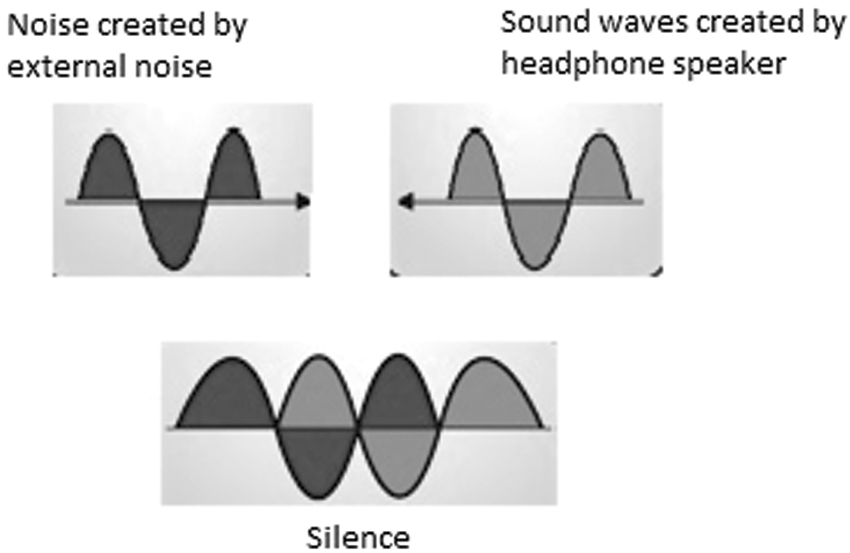
Destructive interference.
SWL is quite noisy, which may make patients uncomfortable. Thus, every approach, such as NCHs, should be investigated and developed to reduce this unwanted noise. More specific NCHs for sound waves that occur during SWL should be developed and used with SWL patients.
The ney (reed flute) was used in ancient times as a relaxing instrument for patients. Ovayolu et al. 6 showed that listening to Turkish classical music featuring the ney decreased anxiety and pain during colonoscopy. In our study, we also used ney music.
Conclusions
Our findings suggest that music therapy during SWL reduces pain and anxiety. Music therapy allows better tolerability of SWL; thus, higher frequencies and more shockwaves can be used. It is a noninvasive, inexpensive, simple, and nonpharmacologic method. Thus, patients are protected from any unwanted side effects of drugs. Music therapy with NCHs was more effective for pain and anxiety reduction. Nonpharmacologic therapies, such as music therapy with NCHs, during SWL should be investigated further and used routinely.
Footnotes
Author Disclosure Statement
No competing financial interests exist.