
Abstract
Objective:
To assess and compare the applicability of the Resorlu-Unsal Stone Score (RUSS) and the Modified Seoul National University Renal Stone Complexity (S-ReSC) score for flexible ureterorenoscopy (f-URS).
Patients and Methods:
We retrospectively analyzed the hospital files of 719 patients who had been treated with f-URS for kidney stone at two referral centers between July 2012 and December 2015. The RUSS and Modified S-ReSC scores were calculated by the same surgeon for each patient by using imaging methods and were compared as to their predictive capability for postoperative success.
Results:
A total of 339 patients (168 men and 171 women) with a mean age of 46.5 ± 16.1 (range:1–86) years and a mean body mass index of 27.1 ± 4.1 (range: 12.8–38.5) were included in the study. The mean stone size was 14.4 ± 5.4 (4–40) mm, and the mean stone surface area was 145.3 ± 76.8 (20–658) mm2. The overall stone-free rate was 70.1%. The mean scores were 0.5 ± 0.7 and 1.8 ± 1.1 for the RUSS and Modified S-ReSC, respectively. In the logistic regression analysis, musculoskeletal deformity, stone size, and the RUSS were identified as independent predictive factors affecting stone-free status (p: 0, p: 0.014, p: 0.048, respectively). Among these parameters, the RUSS had the highest predictive capability (area under curve value 0.65, [95% confidence interval 589, 721]).
Conclusions:
Stone size, presence of musculoskeletal abnormalities, and the RUSS score are important factors affecting SF status after f-URS. Despite the RUSS being an independent predictive factor for SF status, more comprehensive systems with higher predictive capability are needed for clinical usage and academic reporting.
Introduction
P
In the literature, recent discussions focused on preoperatively estimating the outcomes of PNL and f-URS by using imaging modalities and other parameters. An accurate prediction of postoperative success is important, because it helps determine the type of surgery and the necessity of any ancillary procedures before surgery. In this context, three scoring systems have been developed to predict success after f-URS. First, Resorlu et al. developed a scoring system called the Resorlu-Unsal stone score (RUSS). 2 Jung and colleagues developed another scoring system called the Modified Seoul National University Renal Stone Complexity (S-ReSC) score. 3 Both scoring systems have been validated by independent external cohorts. 4,5 A new scoring system has recently been introduced, 6 but it has not yet been externally validated and so is not included in the present study.
This study aimed at assessing and comparing the applicability of the RUSS and the Modified S-ReSC for f-URS by using a large cohort of patients from two referral centers. Ours is the first article that externally compares these validated scoring systems.
Patients and Methods
Study design
After obtaining approval of the local ethics committee, we retrospectively analyzed the hospital files of 719 patients who had been treated with f-URS for kidney stone at two referral centers between July 2012 and December 2015. The prospectively collected data included demographic characteristics (age, gender, body mass index [BMI], previous treatment, renal malformation), stone characteristics (laterality, number, size, surface area, location, lower pole infindibulopelvic angle [IPA]), and perioperative and postoperative parameters (operation and hospitalization time, complications, stone-free [SF] status at first month). Excluded from the study were bilateral cases and those with missing data. Secondary f-URS procedures were also not included in the study.
Before surgery, all patients underwent a routine evaluation, including medical history, physical examination, complete blood count, serum biochemistry, coagulation tests, and urine culture. Computed tomography (CT) and/or intravenous urography (IVU) were used for evaluating stone characteristics and urinary tract malformations. Stone size (mm) was determined by measuring the longest axis on preoperative imaging. Stone surface area (mm2) was calculated according to the European Association of Urology (EAU) guidelines. 7 In case of multiple stones, the sum of measurements was used. The RUSS and Modified S-ReSC scores were calculated by the same surgeon for each patient by using imaging methods and were compared as to their predictive capability for postoperative success.
Scoring systems
Resorlu-Unsal stone score
The RUSS is based on stone size (>20 mm), stone number in different calices (>1), lower pole stone location with IPA <45°, and abnormal renal anatomy (horseshoe kidney or pelvic kidney). One point is given for each clinical condition. Total RUSS is calculated as the sum of these four clinical conditions for a total score of 0–4. 2
Modified S-ReSC score
The Modified S-ReSC system is based on only the number of sites of renal stones involved, regardless of the size and number of those stones. These anatomical sites are as follows: renal pelvis (#1); superior and inferior major caliceal groups (#2, 3); and anterior and posterior minor caliceal groups of the superior (#4, 5), middle (#6, 7), and inferior calix (#8, 9). Each anatomical site is calculated as one point. If the stone involved the inferior caliceal area (#3, 8, 9), one additional point per site is added to the original score. The total Modified S-ReSC score varies from 1 to 12. 3
Surgical technique
All procedures were performed by two experienced surgeons (A.E., A.T.) by using a 7.5F Flex-X 2 (Karl Storz, Tuttlingen, Germany) or 8.8F Wolf Viper (Richard Wolf Medical Instruments, Vernon Hills, IL) fiberoptic flexible ureteroscope. Under general anesthesia, patients were placed in the lithotomy position. Diagnostic ureteroscopy using a 9.5F semi-rigid ureteroscope was routinely performed before the procedure to dilate the ureter, to place the guidewire, and to exclude ureteral pathologies. A 9.5/11.5 or 11/13F ureteral access sheath was placed below the ureteropelvic junction. The stones were fragmented by using a holmium:YAG laser with 200 μm laser fibers until they were deemed small enough to be able to pass spontaneously. The larger fragments were extracted by using a stone basket catheter. At the end of the procedure, the entire collecting system was inspected to confirm achievement of adequate fragmentation and to evaluate stone clearance. A 4.8F Double-J stent was routinely placed and was removed two weeks after the procedure. SF status was defined as no evidence of residual stones or fragments at 1 month follow-up imaging (by plain kidney-ureter-bladder radiography, ultrasound, or CT scan). Treatment success was defined as SF.
Data analysis
All statistical analyses were performed by using SPSS software package version 22 (SPSS, Inc., Chicago, IL). Continuous variables were presented as mean ± standard deviation of mean. Student's t-test was used to compare variables showing a normal distribution, and the Mann–Whitney test was used for variables with nonparametric distribution. Statistical significance was considered as p < 0.05 for all analyses.
Logistic regression analysis was used to identify independent predictive factors affecting SF. The area under the curves (AUCs) of the receiver operating curve (ROC) of the RUSS, and Modified S-ReSC scores were compared to assess the predictive accuracy for stone-free rate (SFR).
Results
A total of 339 patients (168 men and 171 women) with a mean age of 46.5 ± 16.1 (range: 1–86) years and a mean BMI of 27.1 ± 4.1 (range: 12.8–38.5) were included in the study. The mean stone size was 14.4 ± 5.4 (range:4–40) mm, and the mean stone surface area was 145.3 ± 76.8 (range: 20–658) mm2. There were 52 (15.3%) patients who had abnormal renal anatomy. Seventy-nine (23.3%) of the patients had musculoskeletal deformities (35 patients had scoliosis, 25 had kyphosis, 10 had spinal cord injury, 7 had ankylosing spondilitis, and 2 had spina bifida). Of the patients, 10% (n: 34) had stones >20 mm, 61% (n: 207) had stones 11–20 mm, and 28.9% (n: 98) had stones ≤10 mm. Lower calix stone rate was 39%. More than half of the patients had a single stone (n: 239; 65.4%). Patient demographics and basic characteristics of stones are shown in Table 1.
RUSS = Resorlu-Unsal stone score; S-ReSC = Seoul National University renal stone complexity.
The overall SFR was 70.1% (n: 238) for our cohort of 339 patients. Residual fragments <4 mm were identified in 24 patients (7%). Significant differences between the SF and non-SF groups about patient demographics and basic characteristics of stones were identified for the following parameters: BMI, gender, renal malformation, musculoskeletal deformity, number of stones, usage of an access sheath, lower pole IPA, stone size, and stone surface area (p: 0.038, p: 0.012, p: 0, p: 0, p: 0.001, p: 0, p: 0.004, p: 0, p: 0, p: 0.004, respectively) (Table 1).
The mean scores were 0.5 ± 0.7 and 1.8 ± 1.1 for the RUSS and Modified S-ReSC, respectively. Both scoring systems were significantly associated with SFR (p: 0.000, p: 0.003). In the logistic regression analysis, musculoskeletal deformity, stone size, and RUSS were identified as independent predictive factors affecting SF status (p: 0, p: 0.014, p: 0.048, respectively) (Table 2).
CI = confidence interval.
Figure 1 and Table 3 show values for the ROC curves and AUCs. The AUCs of the RUSS and Modified S-ReSC scores for predicting SFR were 0.655 (95% confidence interval [CI] 589, 721) and 0.596 (95% CI 527, 665), respectively.
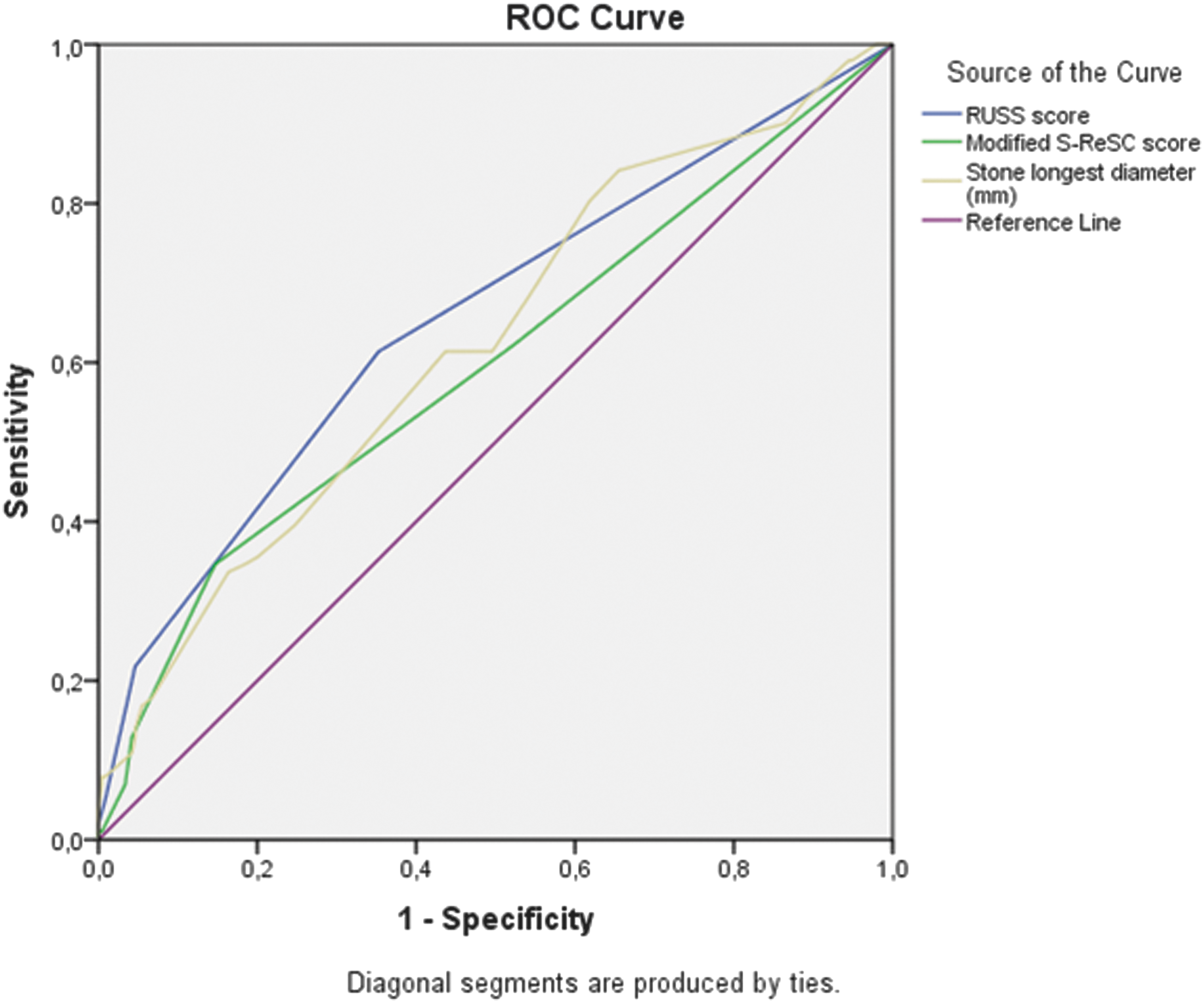
ROC curves of the RUSS, Modified S-ReSC scores, and stone longest diameter. ROC = receiver operating curve; RUSS = Resorlu-Unsal stone score; S-ReSC = Seoul National University renal stone complexity.
A total of 18 intraoperative or postoperative complications were observed in 17 (5%) patients. Most complications were mild (Clavien grade I or II), but seven patients (2%) experienced Clavien grade IV complication (urosepsis).
Discussion
Current EAU guidelines on the treatment of renal stones recommend PNL as the first-line treatment for stones >2 cm, and f-URS and SWL for stones <2 cm. 1 Technological advances and satisfactory success rates have extended therapeutic indications of f-URS in the past two decades. In high-volume centers, f-URS has been used as a treatment option with comparable success and complication rates even for larger stones >2 cm. 8 Medium-sized renal stones that are not appropriate for SWL or PNL, SWL-resistant small renal stones, bleeding disorders, and concomitant renal and ureteral stones are considered the main indications of f-URS. 9
In renal stone surgery, an accurate prediction of SFR is important when considering surgical modalities and the necessity of any ancillary procedures. Four new predictive nomograms have recently emerged to systematically and quantitatively assess kidney stone complexity to predict outcomes after PNL. 10 –13 These systems have already been externally validated and extensively discussed in the literature. 14 The widespread use of a standardized nephrolithometric nomogram can improve patient care by providing information to assist in informed clinical decision making and patient counseling, in addition to improving academic reporting. On the other hand, only two validated tools have been developed to predict surgical success after f-URS.
First, in 2012, Resorlu et al. analyzed 207 patients who underwent f-URS in a single institution and developed a scoring system called the RUSS. 2 The RUSS is based on stone size, stone number, lower pole stone location with narrow IPA, and renal anatomy. An RUSS final score can range from 0 to 4. It has been externally confirmed that higher RUSS scores reflect more complex cases, with lower probabilities for postoperative success. 4 The RUSS is easy to apply in clinical practice, except for the identification of lower pole IPA, which is slightly troublesome to measure in daily practice. In the present study, IPA measurements were done by two experienced surgeons using either IVU or coronal plane CT. The RUSS system has some limitations. The main limitation of the RUSS system is that the study analyzed only a limited number of patients who scored more than three points. In addition, the cohort included only two renal malformations: horseshoe kidney and pelvic kidney. In contrast, our cohort had patients' malrotation, ureteral or pelvicaliceal system duplication, ureteropelvic junction stenosis, cross ectopy, diverticulum stone, and solitary kidney other than horseshoe kidney and pelvic kidney. We added one point to the total score for each renal malformation. Furthermore, our cohort included 79 patients with musculoskeletal deformities. In the statistical analysis, only musculoskeletal deformity was found as an independent predictive factor.
Second, in 2014, Jung and colleagues reviewed 88 patients and developed another scoring system called the Modified S-ReSC score. 3 The original S-ReSC score was designed for PNL in 2013 and was based on the position of the stones, regardless of their size and number. 15 In the modification of this system for f-URS, stones located in the lower calix had higher scores. In addition, authors claimed that stone size and stone number were no hindrance to f-URS except when a stone was large. They excluded from their study any patients who had stones they deemed to be too large, and PNL was performed on these patients. The stone burden is not considered an important factor in this scoring system. This point seems to be the main limitation of the Modified S-ReSC score. On the other hand, in the same study, the authors internally compared the Modified S-ReSC and RUSS systems and reported that, according to their logistic regression analyses, the predictive accuracy of the Modified S-ReSC score was higher than that of the RUSS. They, however, had a very small sample size (n: 88); however, with our cohort of 339 patients, we identified the RUSS as an independent predictive factor.
Recently, a new nomogram has been reported. 6 In it, 310 f-URS procedures were retrospectively analyzed and five independent predictors of SF were identified: stone volume (≤500 mm3, 500–1000, 1000–2000, ≥2000), stone number (solitary, multiple), hydronephrosis (absent, present), lower pole calculi (absent, present), and operator's experience (<50, ≥50). The authors reported that the mean value for AUC for nomogram predictions was 0.87. This assertive figure is higher than those of the RUSS and Modified S-ReSC scoring systems. For wide clinical applications of a scoring system, external validation by an independent cohort is critical; therefore, this nomogram should be validated by such a cohort.
In the present study, the overall success rate was 70.1%. This figure may be slightly lower than results in the literature, because we defined “success” as complete stone clearance (SF). When residual fragments <4 mm were added, the rate was 77.1%. We analyzed the predictive factors and identified that BMI, gender, renal malformation, musculoskeletal deformity, number of stones, usage of an access sheath, lower pole IPA, stone size, stone surface area, and RUSS and Modified S-ReSC scores were predictors of SF. Among these modalities, musculoskeletal deformity, stone size, and RUSS were identified as independent predictors, but the RUSS had a weak correlation in logistic regression analysis (p: 0.048). The AUC values of the RUSS and Modified S-ReSC scores were 0.655 and 0.596, respectively, figures that are not fully satisfactory in terms of a nomogram's predictive accuracy.
As to the limitations of the present study, first, it was retrospective in nature. Second, SF was assessed by different imaging modalities, in addition to CT. A limited number of patients (40%) were assessed with CT for postoperative SF. Furthermore, many factors, including stone density, stone composition, and prestenting, were not assessed in the study. However, this study contributes to the literature, because it is, to the best of our knowledge, the first to externally compare the RUSS and Modified S-ReSC scoring systems.
Conclusions
Our study shows that despite the RUSS being an independent predictive factor for a successful outcome of renal stone surgery, both it and the Modified S-ReSC had low predictive accuracy for identifying SF after f-URS. More comprehensive systems are needed for the development of these modalities for clinical usage and academic reporting.
Footnotes
Acknowledgment
The authors appreciate the contributions and editorial assistance made by S. Delacroix, a native English speaker.
Author Disclosure Statement
No competing financial interests exist.