
Abstract
Introduction:
Primary aim of this study was to investigate the feasibility and the safety of PERUSIA (posterior, extraperitoneal, robotic, under santorini, intrafascial, anterograde) radical prostatectomy (RP). Secondary aim was to evaluate oncologic and functional results. The main intent of PERUSIA is to reduce injury of the Neuro-Vascular Bundles (NVB) and to preserve periurethral anterior structures. This is the first reported prospective cohort study about our technique.
Materials and Methods:
We collected prospective data of a cohort of 210 patients who had undergone PERUSIA RP between January 2013 and May 2015. Key points of this technique included the following: posterior approach to intrafascial plane, which was developed from the median to lateral side, anterograde preservation of the Veil of Aphrodite, and development of an anterior avascular plane to preserve the santorini plexus. We included only sexually potent patients with low-risk disease. Perioperative, oncologic, and functional outcomes were collected. Postoperative full continence was defined as no pad use. Patients were defined potent when International Index of Erectile Function (IIEF-5) score was >17. Median follow-up was 22 months.
Results:
Median operative time and median estimated blood loss were 120 minutes and 150 mL, respectively. 25 patients (11.9%) experienced a total of 36 complications overall with an overall complication rate of 17.1%. We reported 3 (8.3%) grade IIIb complications and no major ones. Overall positive surgical margin rate was 20% with biochemical recurrence occurring in 3.8% of patients at a median follow-up of 22 months. Immediate urinary continence rate (1 day after catheter removal) was 66.6%. At 3 and 12 months, the continence rate was 90.4% and 96.1%, respectively, while sexual potency rate was 70.4% and 80.9%.
Conclusion:
PERUSIA RP has proved to be safe and effective for low-risk prostate cancer with exciting functional outcomes in terms of early recovery of urinary continence and sexual potency.
Introduction
I
The main intent of PERUSIA (posterior, extraperitoneal, robotic, under santorini, intrafascial, anterograde) is to reduce injury of the NVB and to preserve periurethral anterior structures. This is the first reported prospective cohort study about PERUSIA technique. Primary aim of this study was to investigate the feasibility and the safety of PERUSIA RP. Secondary aim was to evaluate oncologic and functional results.
Materials and Methods
Study population
In a High Volume tertiary Institution, 500 RARP were performed by a single skilled surgeon (E.M.), between April 2011 and February 2016. Internal review board approved the study, and written informed consent was obtained from all patients. We collected prospective data of a cohort of 210 patients who had undergone the previously described PERUSIA-RP 9 between January 2013 and June 2015. Preoperative clinical and demographic characteristics, surgical features, and postoperative parameters are listed in Table 1. An observational and prospective study was carried out evaluating perioperative, oncologic, and functional outcomes with a median follow-up of 22 months (range 12–37).
BMI = body mass index; IIEF-5 = International Index of Erectile Function; IPSS = International Prostate Symptom Score; PSA = Prostate Specific Antigen.
All patients were stratified according to prostate cancer (PCa) risk category of European Association of Urology guidelines, and an active treatment was offered to those who did not fulfill the criteria for Active Surveillance. 10 We included only patients with low-risk PCa and a life expectancy >10 years, who were sexually potent and did not accept active surveillance. Preoperatively, all patients were assessed through memorial Sloan-Kettering PCa nomograms 11 to evaluate lymph node involvement risk and to predict the postoperative probability of cancer remaining progression free. Usually, we perform pelvic bilateral lymphadenectomy when the involvement risk is higher than 2%. In the absence of well-defined criteria, we arbitrarily excluded those patients with extracapsular extension risk higher than 30%. In these cases, we performed a wider excision, according to the side-specific density of positive biopsy cores.
Surgical complications were evaluated according to the Clavien Dindo Classification system. Urinary continence was evaluated through direct interview according to question number 5 of the expanded PCa index composite questionnaire. 12 We evaluated urinary continence at 1 day after catheter removal (immediate) and at 3 (early) and 12 months after surgery. Patients were considered fully continent, slightly incontinent, and incontinent when they used no pad, one pad, and more than one pad, respectively.
Sexual potency was evaluated using International Index of Erectile Function (IIEF-5) test 13 preoperatively and at 3 and 12 months after surgery. Specifically, patients were defined potent when IIEF-5 score was >17, while those who used phosphodiesterase-5 inhibitors to obtain an IIEF-5 score >17 were considered potent with drug; patients with an IIEF-5 score <17 were classified as impotent. Follow-up consisted of medical examination, Prostate Specific Antigen (PSA) measurement, administration of IIEF-5 questionnaires, and self-reported urinary incontinence. Oncologic outcomes were evaluated in terms of positive surgical margins (PSMs) and biochemical recurrence (BCR) (defined as PSA >0.2 ng/mL in two consecutive evaluations) at a median follow-up of 22 months. Data were analyzed with GraphPad Prism 6.0; the significance threshold was set at 0.05.
Patients' preparation
Extraperitoneal space is digitally created. We place optical trocar 1 cm under the navel and two robotic trocars 5 cm laterally, avoiding the rectus abdominis muscular belly. The last robotic trocar on the left and the assistant's one on the right are placed, under laparoscopic vision, 2 cm above and medially to the anterior–superior iliac spine. Then, the patient is placed in 20° Trendelenburg position. After induction of pneumoRetzius, we dock the robot (Da VinciSi, Intuitive Surgical, Sunnyvale, CA).
The main steps of PERUSIA technique are the following: • Bladder neck: U-shaped incision on the bladder neck preserving circular fibers. • Approach to seminal vesicles: Perpendicular approach to medial aspect of the seminal vesicles (SVs), which are mobilized from their lodge, maintaining a medial avascular plane, avoiding damage of proximal neurovascular plate (Fig. 1). • Anterograde intrafascial dissection: After incision of the Denonvilliers' fascia, an athermal dissection is performed in a lateral manner, with enlargement of the retroprostatic space toward the prostatic pedicles. • Preservation of the anterior periprostatic tissue: Following the medial aspect of the VA, we reach the anterior periprostatic tissue and detouch it bluntly from the fascia, without damaging the accessory neurovascular plate, which is a neural pathway for both cavernosal and sphincteric systems (Fig. 2). The preservation of the VA avoids the dissection of the endopelvic fascia that remains on the outside. • Preservation of santorini plexus: It is not ligated or cut, developing an anterior avascular plane to identify the prostatic urethral junction maximizing the urethral length (Figs. 3–4). • Urethrovesical anastomosis: It is performed in a semicontinuous manner using Quill®.
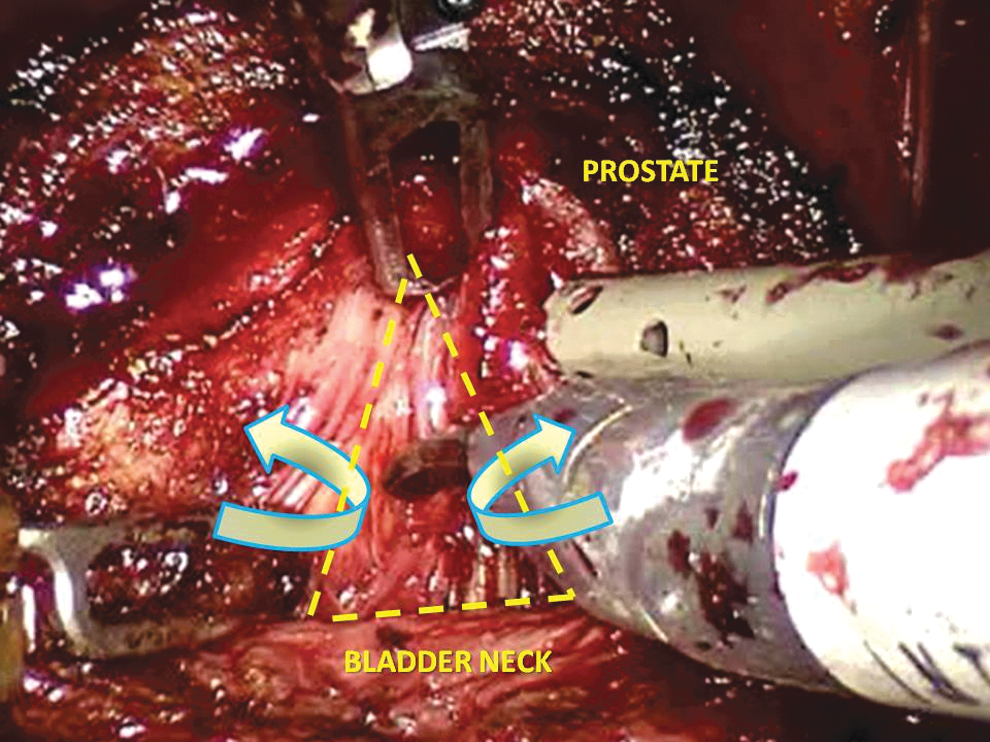
Posterior and median approach to seminal vesicles. Curved arrows show the course of dissection after seminal vesicle exposure.
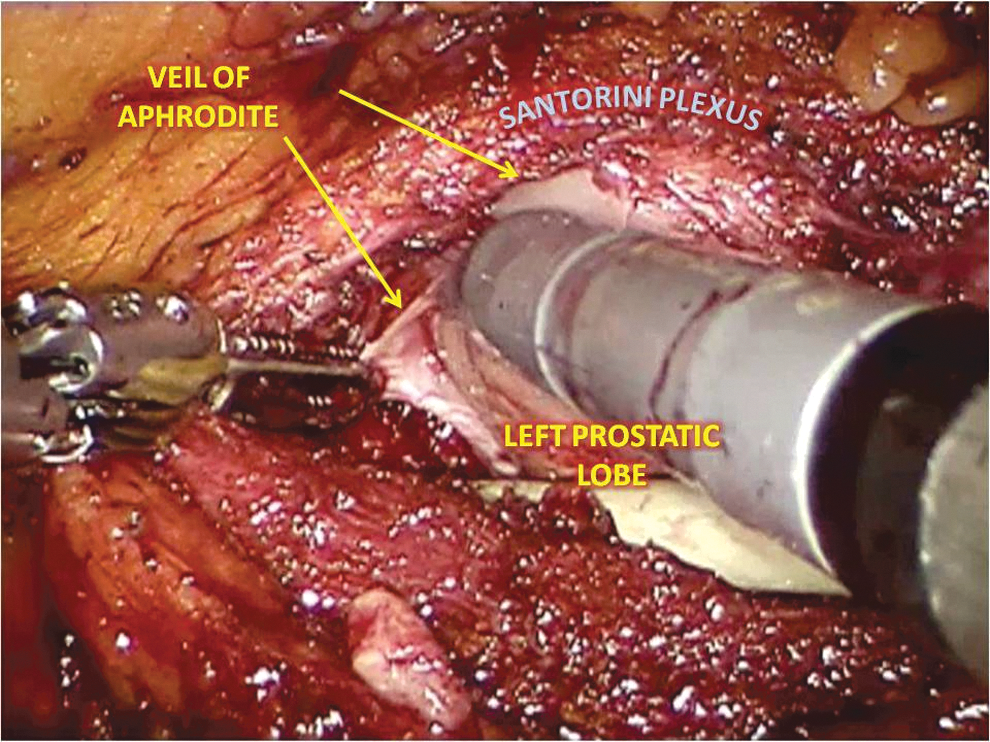
Veil of Aphrodite preservation during posterior–lateral prostatic dissection.
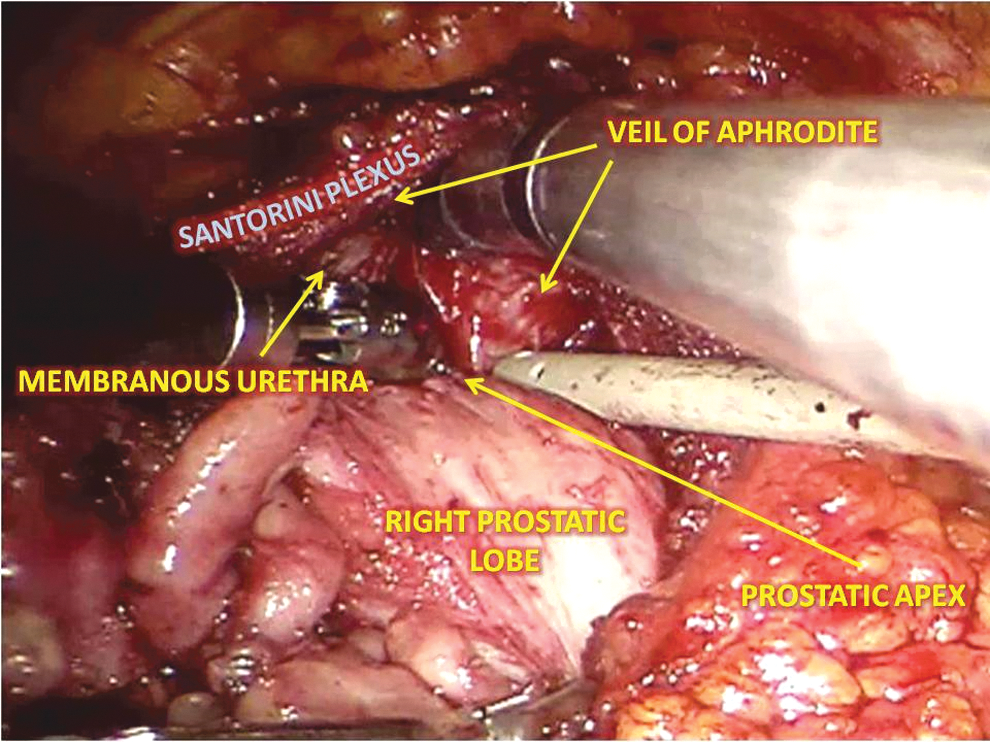
Circumferential dissection of the apex after development of an anterior avascular plane.
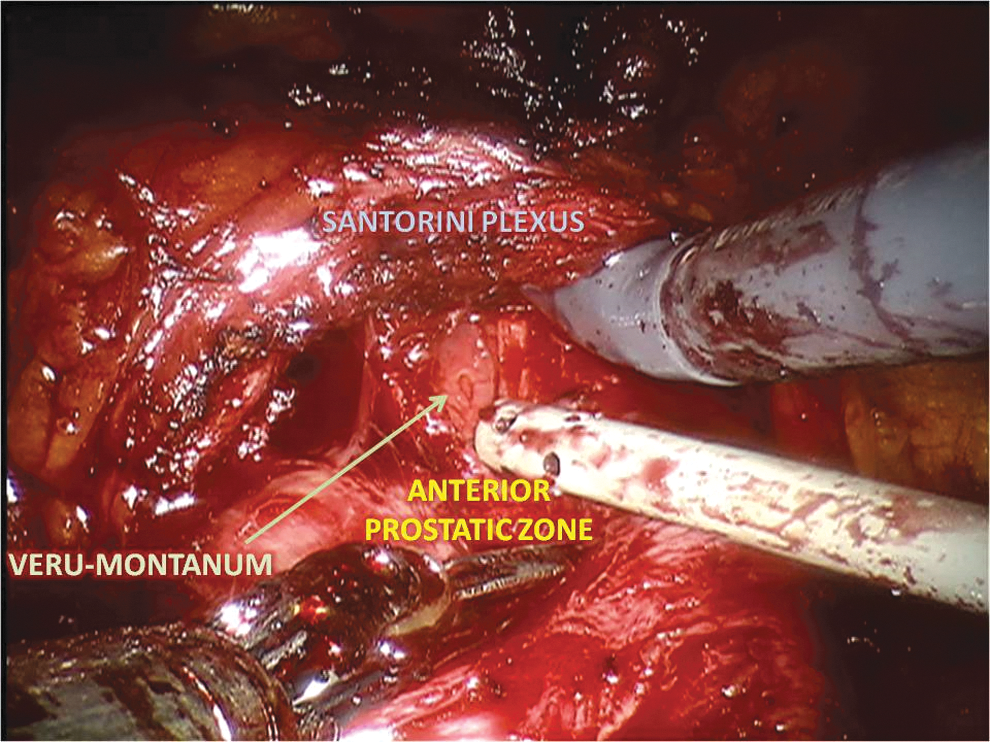
Exposition of anterior aspect of prostate–urethral junction and visualization of Colliculus seminalis after section of anterior urethra.
Results
Perioperative outcomes
Median operative time and median estimated blood loss were 120 minutes (range 90–290) and 150 mL (range 100–450), respectively. Transfusion rate was 2.8% (6/210). Median time to flatus was 16 hours. Median catheterization time was 7 days (range 6–14), and median length of hospitalization was 8 days (range 4–12). No conversion to transperitoneal approach needed even when small lacerations were noted in the peritoneum. Of 210 patients, 25 (11.9%) experienced a total of 36 complications. Overall complication rate was 17.1%. Grade I and II complications were 15 (41.6%) and 14 (38.8%), respectively. Grade III complications were 7 (19.4%): 4 (11.1%) pelvic lymphocele requiring percutaneous drainage (IIIa) and 3 (8.3%) reoperations for bleeding (IIIb). No IV or V grade complications occurred.
Oncologic outcomes
Overall PSMs were 42/210 (20%); upstaging to pT3 occurred in 15 patients (7.1%). In pT2 and pT3 PSMs, rate was 17.4% (34/195) and 53.3% (8/15), respectively. Focal PSMs rate was 21/210 (10%) and were all in pT2. Table 2 shows the pathologic stratification. We observed BCR in eight patients (3.8%) at a median follow-up of 22 months.
GS = Gleason Score; pGS = pathological Gleason Score; PSMs = positive surgical margins.
Functional outcomes
One hundred forty patients (66.6%) reached immediate urinary continence. At 3 months, 190 patients (90.4%) were fully continent. At 12 months, urinary continence rate was 96.1% (202/210), eight patients (3.9%) were slightly incontinent, whereas nobody was incontinent. Sexual potency rate was 70.4% (148/210) at 3 months: 72 (48.6%) were fully potent and 76 (51.4%) potent with drug. At 12 months, 170/210 (80.9%) patients were potent, of which 80 (47%) with drug.
Discussion
RARP is an established treatment for localized PCa with a 10-year life expectancy. 14 The equivalent efficacy between the ERP and transperitoneal RP is by now demonstrated. 15 A recent meta-analysis demonstrated that the ERP guaranteed shorter operative time and minor complication rate in particular bowel ones, reducing the risk of postoperative ileus and intraoperative bowel injuries because the peritoneal cavity was not violated. 15 Furthermore, Trendelenburg of 20° consents to decrease the complications related to body positioning, as well as cardiovascular and respiratory ones. 16 A limitation of ERP is the difficulty to carry out an extended lymphadenectomy. However, our study included only low-risk PCa, who are not suitable for an extended lymph node dissection, because the risk of involvement does not exceed 5%. 17
Our perioperative parameters as well as complication rate are in line with those reported in previous extraperitoneal and transperitoneal series, 15 confirming that our technique is a safe procedure. Inferior epigastric vessel damage is a peculiar complication of ERP, but in our experience it never occurred because the extraperitoneal space is created digitally at the beginning, and then the space development and trocar placement are completed through laparoscopic vision. Median estimated blood loss was 150 mL. This low bleeding rate is due to the preservation of dorsal vascular complex (DVC) and the development of an avascular intrafascial plane for preservation of NVBs.
The presence of proximal and accessory neurovascular plate, described in the tri-zonal model of periprostatic anatomy, 8 and the histologic demonstration that seminal vesicle fascia extends and scatters laterally into NVB 18 justify our median approach to the SV, and our full nerve-sparing technique begins from the middle, where the nervous fibers are not represented, toward the posterior–lateral side in the intrafascial plane. Some authors have reported the presence of neurovascular structures in the context of VA, even in its higher and anterior aspect. 6,8 Respect to Vattikuti's experience, we preserve the VA completely, not only in the lateral side but also in the anterior, following the virtual space between prostatic lobe and surrounding fascia through an athermal detachment. 14 In this way, we reduce to the maximum the manipulation of the NVBs and their damage, decreasing also the bleeding. Furthermore, the anterograde dissection allows us to better identify the VA before it becomes thinner anteriorly, thus the prostate gland may be shelled out from the overlying VA and DVC. Using this avascular plane, we preserve DVC and its hemodynamic function, reducing bleeding and the employment of thermal energy.
Patel and coworkers proposed a standardized nerve-sparing grading system based on intraoperative visual cues, using a landmark artery to delineate the course of the NVB in a retrograde manner. 2 In our experience, visualization is not necessary because the NVB remains outside of the plane of dissection. The preservation of the anterior compartment has already been described by Bocciardi and coworkers. 19 Compared to their transperitoneal technique, we use an extraperitoneal approach with lower Trendelenburg degree and do not need to open the Douglas space to reach the Denonvilliers' fascia.
The overall PSMs rate was 20%; in pT2 and pT3 PSMs, rate was 17.4% and 53.3%, respectively. These results were slightly elevated, even if consistent with those reported in recent Literature. 20 Our full nerve-sparing technique 9 could, in part, justify this result, but we would emphasize that the focal PSMs (defined as <1 mm) were 21/34 (61.7%) in pT2: the high rate of focal PSMs in low-risk disease should reduce the prognostic impact of our slightly elevated PSMs rate. Even if historically PSMs are considered associated with BCR, at longer follow-up this risk should not differ between patients with negative surgical margins and those with PSMs <1 mm. 21 However, we would also like to stress that many PSMs were reported during the learning curve of our technique; further studies will be needed to evaluate if the PSMs rate may improve with increasing confidence with PERUSIA technique.
We reported an immediate urinary continence rate of 66.6%, while at 3 and 12 months continence rate was 90.4% and 96.1%, respectively. These results are similar to those of major RARP series, ranging from 69% to 96% at 12 months when the no pad definition was used. 22 Specifically, we would like to highlight the quick recovery of continence, in terms of immediate and early continence. In Literature, the weighted mean continence rate immediately after catheter removal is reported at about 25.7%. 23 This exciting result may be due to our full nerve-sparing technique with preservation of the VA that allows to reduce the damage of intrapelvic nerves supplying the rhabdosphincter and to perform a “no touch” approach of DVC.
A recent meta-analysis has reported that the degree of preservation of NVB is associated with urinary continence in the first postoperative 6 months. 24 Steineck and coworkers demonstrated the same association also in the long term. 25 Furthermore, a conservative management of the DVC has a positive effect on the continence recovery. Porpiglia and colleagues demonstrated that a selective ligature of DVC permits quicker continence recovery than a standard one. 26 Recently, Ganzer and colleagues demonstrated that DVC overlaps 37% and 30% of the cross-sectional urethral sphincter surface at the prostatic apex and 5 mm distal to the apex, respectively. 27 Some authors proposed the reconstruction of the periurethral muscular–fascial structures to avoid caudal traction on urethra–sphincter complex. 22,28,29 PERUSIA technique does not include any muscular–fascial reconstruction because the preservation of both endopelvic fascia and VA avoids the urethral retraction and the damage of anatomic structures that physiologically support the external sphincter. Moreover, the anterograde dissection allows us a better visualization of prostate–urethral junction and, therefore, a more careful apical dissection that results in improved preservation of urethral length. Meticulous dissection also reduces the injury of pudendal nerve branches to the rhabdosphincter that is in close proximity to the prostate apex and endopelvic fascia. 9
The sexual outcome is also satisfying, with a potency rate of 70.4% and 80.9% at 3 and 12 months, respectively. These results are at least comparable to those of larger series. A recent systematic review reported potency recovery rates of 50% (32%–68%), 65% (50%–86%), 70% (54%–90%), and 79% (63%–94%) at 3, 6, 12, and 24 months, respectively. 30 We would like to point out the quick recovery of potency in the PERUSIA technique. This finding is likely due to preservation of the posterolateral as well as anterior periprostatic nervous and vascular structures. Indeed, a recent study has demonstrated that cavernous nerve fibers were a continuation of the nervous fibers running on the anterior and lateral side of the prostate. 31
The main limitation of our study was a restricted follow-up, in particular, regarding the evaluation of oncologic outcomes.
Conclusions
PERUSIA-RP has proved to be safe and effective for low-risk localized PCa with the advantage of achieving encouraging functional outcomes in terms of quick recovery of urinary continence and sexual potency. PERUSIA-RP might help to reduce injury of the NVB and to preserve periurethral anterior support minimizing urethral retraction. Otherwise, particularly during the learning curve, PSMs rate seems still high and further studies are needed to understand if the PSMs rate may improve with increasing experience.
Footnotes
Author Disclosure Statement
No competing financial interests exist.