
Abstract
Purpose:
To compare the oncological and functional outcomes of robotic partial nephrectomy (RPN) with radical nephrectomy (RN) in renal-cell carcinoma (RCC) cases with pT3a staging.
Patients and Methods:
A retrospective analysis of our IRB-approved nephrectomy database from 2005 to 2015 was performed. RPN and RN cases with confirmed RCC and pT3a staging were matched. Preoperative variables, functional, and oncological outcomes were compared between the groups, as well as Kaplan–Meier estimated overall survival (OS), cancer-specific survival (CSS), and recurrence-free survival (RFS). A multivariable Cox proportional hazards regression model for overall mortality rate was generated to evaluate hazard ratios (HRs) of potential risk factors.
Results:
Seventy patients with pT3a tumors composed each group. Preoperative variables were comparable between groups. The median follow-up time for the cohort was 20 (9–38) months and the renal function preservation was higher in the RPN group (86% vs 70%; p < 0.001). The estimated 3 years of OS (90% vs 84%; p = 0.42), CSS (94% vs 95%; p = 0.78), and RFS (95% vs. 100%; p = 0.06) were similar between RPN and RN groups, respectively. On multivariable Cox regression model, the presence of ≥2 aggressive tumor features was the only factor associated with increased risk of overall mortality rate (HR 4.01 95% confidence interval [1.13, 14.27)]; p = 0.03).
Conclusion:
Patients with localized pT3a RCC treated with RPN had similar short-term oncological and better renal functional outcomes compared with similar cases treated by RN. In the minimally invasive robotic surgery era, renal masses suspicious for pathological T3a disease should not be a deterring factor for performing nephron-sparing surgery when technically feasible by skilled surgeons.
Introduction
P
Renal cell carcinoma (RCC) growth into the renal vein, sinus fat, or perinephric fat (pT3a) is a poor prognostic factor 5 –7 and it is more likely to occur with increased tumor complexity. 8 There is paucity of literature regarding outcomes of robotic partial nephrectomy (RPN) in this setting and its utility is still open for debate. Thus, our objective was to compare the oncological and functional outcomes of RPN with radical nephrectomy (RN) in RCC cases with pT3a staging.
Patients and Methods
A retrospective analysis of our IRB-approved prospective nephrectomy database from 2005 to 2015 was performed. Patients with confirmed RCC and pT3a staging who underwent RPN or RN, including open, laparoscopic, and robotic, were matched according to age, R.E.N.A.L. nephrometry score, preoperative GFR, and pathologic tumor size. Four experienced surgeons performed the RPN cases. Patients with metastatic disease at the time of surgery or a solitary kidney, in which partial nephrectomy would be mandatory, were excluded.
Preoperative CT or MRI was used to calculate the greatest tumor diameter, the R.E.N.A.L. score, 9 and to classify the preoperative clinical stage for all patients. Tumors were classified as clinical T3 when the imaging study suggested invasion of sinus fat and/or beyond the renal capsule and/or presence of tumor thrombus within the renal vein branches. Pathological features analyzed included histological classification, Fuhrman grade, 10 and TNM stage, according to the current 2010 age-adjusted Charlson comorbidity index classification. 11 Glomerular filtration rate (eGFR) was estimated using the Modification of Diet in Renal Disease (MDRD) formula. 12 Renal function preservation was assessed as a proportion of eGFR at 3–6 months postoperatively to preoperative eGFR.
Preoperative variables and functional and oncological outcomes were compared between the groups. Local recurrence and metastasis were identified on follow-up imaging according to our institution guidelines. The patient is followed up with cross-sectional imaging (CT/MRI) and chest radiograph twice in the first postoperative year and annually after. Cause of death for assessment of cancer-specific survival (CSS) was obtained from clinical records. Length of follow-up was determined by the time between surgery and most recent office visit or time of death.
For variables with normal distribution, data are presented as mean ± standard deviation and the respective groups were compared using Student's t-test. For variables with non-normal distribution, data are presented as median (interquartile range [IQR]) and the respective groups were compared using Mann–Whitney U-test. Categorical variables were compared using chi-squared test. A multivariable Cox regression model for overall mortality rate was generated to evaluate hazard ratios (HRs) for variables of interest (surgery type, age-adjusted Charlson comorbidity score (ACCI), R.E.N.A.L. score, eGFR preservation, and histopathology features of the tumor, including clear cell type, positive surgical margin, necrosis, lymphovascular invasion, Fuhrman grade ≥3, presence of sarcomatoid element, and features contributing to pT3a staging: renal vein, perinephric, or sinus fat invasion). Significance was set at p < 0.05. Analyses were performed using SPSS v21 software (IBM SPSS Statistics; IBM Corp., Armonk, NY).
Results
From the total 1005 RPN performed during the period study, 76 patients had pT3a tumors on final histology. Six cases in the RPN group were converted intraoperatively to RN and were excluded from the comparison analyses since the outcomes could be different from the rest of NSS patients; however, their outcomes are also detailed. The remaining patients were matched to 70 RN cases (10 open, 49 laparoscopic, and 11 robotic) according to the variables mentioned previously.
Both groups were comparable regarding patient age, R.E.N.A.L. score, preoperative eGFR, and pathological tumor size (Table 1). Despite a trend toward the presence of larger tumors in the RN group, the difference was not statistically significant. RPN group had a higher ACCI compared with the RN group (4 vs 3; p = 0.02). The median warm ischemia time for the RPN group was 24 (19–30) minutes. Three cases were performed with cold ischemia (21, 25, and 28 minutes) and two with zero ischemia. No patient died or required dialysis related to surgery.
Aggressive histopathological features include: positive surgical margin, necrosis, LVI, Fuhrman grade ≥3, and presence of sarcomatoid element.
Estimated by percentage of GFR remaining from pre- to postoperative evaluation.
In the median follow-up period of 20 (9–38) months.
ACCI = age-adjusted Charlson comorbidity index; BMI = body mass index; eGFR = estimated glomerular filtration rate; IQR = interquartile range; LVI = lymphovascular invasion; RN = radical nephrectomy; RPN = robotic partial nephrectomy; SD, standard deviation.
The histopathologic assessment revealed a clear cell-type RCC in 71.4% and 91.4% (p = 0.002) of RPN and RN, respectively. The tumors removed by RPN showed similar rates of high-grade disease (Fuhrman ≥3) and positive margins compared with RN ones (61.5% vs 57.1%; p = 0.33, and 5.7% vs 5.7%; p = 1.0, respectively). The perinephric fat was the most common form of invasion in the RPN group (50% vs 22.9%; p < 0.001), while the renal vein and sinus fat were most involved in the RN group (85.7% vs 54.3%; p = 0.001). The renal function preservation, as estimated by percentage of postoperative to preoperative GFR, was higher in the RPN group (86.0% vs 70.0%; p < 0.001).
In total, three patients (two RPN [2.9%] and one RN [1.4%]; p = 1.0) developed local recurrence after 6, 18, and 48 months, respectively, and remain alive after a follow-up time of 39, 24, and 91 months. Ten patients (six RPN [8.6%] and four RN [5.7%]; p = 0.74) developed distant metastasis. The Kaplan–Meier estimated that 3 years of recurrence-free survival (RFS) (95% vs 100%; p = 0.06), CSS (94% vs 95%; p = 0.78), and overall survival (OS) (90% vs 84%; p = 0.42) were similar between RPN and RN groups, respectively (Fig. 1). On multivariable Cox regression model, the presence of ≥2 aggressive tumor features (including positive surgical margin, necrosis, lymphovascular invasion, Fuhrman grade ≥3, and presence of sarcomatoid element) was the only factor associated with increased risk of overall mortality rate (HR 4.01 95% confidence interval [1.13, 14.27)]; p = 0.03) (Table 2).
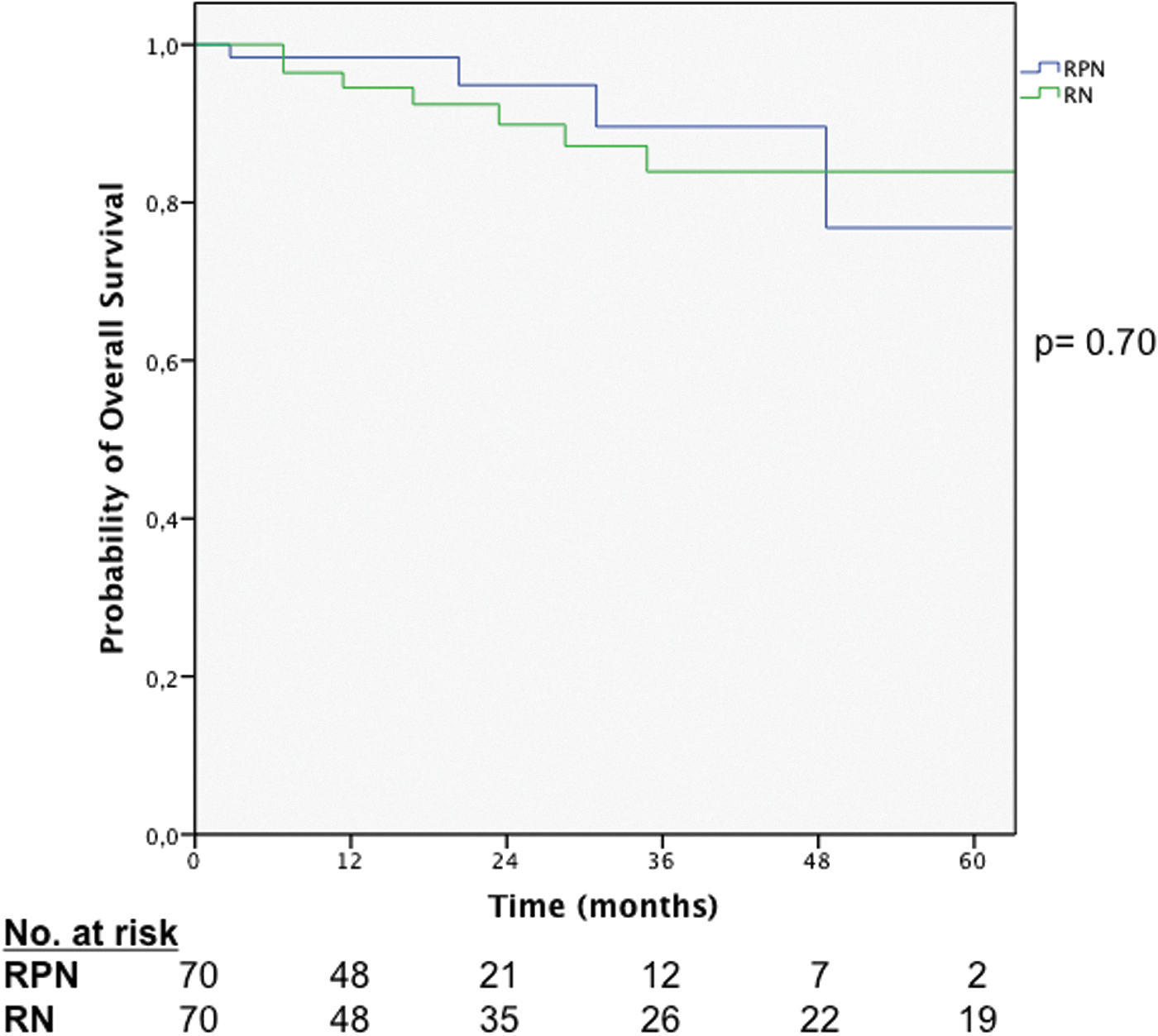
Probability of overall survival according to the surgical technique.
Aggressive histopathological features include positive surgical margin, necrosis, LVI, Fuhrman grade ≥3, and presence of sarcomatoid element.
CI = confidence interval.
Six patients with initial plan for RPN were converted to robotic RN intraoperatively due to concern for oncological safety (gross margin positive in four cases) or due to the presence of positive margin within the sinus fat on frozen section (two cases). All patients ultimately had a pT3a tumor with negative margins on final pathology assessment. During a median follow-up of 11 (IQR 10–28) months, no local recurrence or metastasis was detected in this subgroup.
Discussion
Partial nephrectomy and minimally invasive approaches for the management of T1a tumors have evolved during the last two decades, demonstrating oncological safety and renal function preservation 13 and in the near future may become the standard of care for T1b tumors as well. RPN is already an established and widely adopted approach for the surgical treatment of small renal masses 14 and contemporary studies have demonstrated its feasibility in more complex cases with the growing experience with this technique. 2 –4 Nonetheless, RPN is still a challenging technique for T3a tumors and its utility in this setting warrants further debate. In this study, we compared the outcomes of patients with pT3a tumors who underwent RPN with those treated by RN.
The safety of partial nephrectomy for T3a tumors has already been addressed in some studies, most of them suggesting equivalent oncological outcomes when comparing partial with RN. 8,15 –19 However, these studies included all types of surgical modalities (open, laparoscopic, and robotic), 16,19 incorporated cases with aggressive tumors characteristics other than pathological T3a (tumors >7 cm and high Fuhrman grade 17,18 ), or used prior T3a classification, in which renal vein invasion were considered as T3b. 15 In a recent multi-institutional study, Oh and colleagues 16 demonstrated that partial nephrectomy had local recurrence rate comparable with RN in the subset of clinical T1 tumors upstaging to pathological T3a and supported the notion that for selected cases, PN is a safe treatment even in the face of adverse pathological findings.
In contrast, reporting the outcomes of RPN for pT3a tumors, Gorin and colleagues 8 showed that clinical T1 tumors that upstaged to pT3a had worse RFS compared with those with pT1-2 tumors (91.8% vs 99.2%; p = 0.003, respectively). However, in this study, the pT3a-upstaged cohort was not compared with similar pT3a tumors treated by RN, so one cannot firmly conclude that the surgical approach (RPN) and not the aggressive tumor biology is the responsible factor for the higher recurrence rate.
In our study, we compare pT3a tumors treated by different approaches in two comparable groups (RPN vs RN) encompassing moderate complex tumors (median R.E.N.A.L. score of 8 of both groups). The clinical stage demonstrated differences in T1a and T1b tumors between groups; however, the clinical T3a rate was similar (39 [55.7%] vs 43 [61.4%]; p = 0.49) in RPN and RN groups, respectively.
Regarding the oncological outcomes, the rates of local recurrence and distant metastasis were comparable between the groups in a short-term follow-up, as well the 3-year estimated Kaplan–Meier RFS, CSS, and OS. Moreover, RPN has the additional benefit of better renal function preservation. The multivariable Cox regression analysis assessing risk factors predicting worse outcomes demonstrated a 4.01 HR for overall mortality rate in patients with two or more aggressive features in the histopathological evaluation, while the surgical modality (RPN or RN) was not a predicting factor.
The components of T3a stage were also included in the multivariable analysis because this remains a debatable topic. Bedke and colleagues 20 demonstrated that sinus fat invasion was an unfavorable prognostic factor compared with perinephric fat invasion (HR 2.24, p = 0.019). Other previous studies 5,21,22 demonstrated that isolated fat invasion (perinephric and/or renal sinus) has similar behavior as renal vein invasion, while if both components were present, worse outcomes were observed, advocating modification of the current staging system. However, a recent large multi-institutional study, 23 including 1247 patients with pathological T3a tumors, demonstrated no difference regarding cancer-specific mortality rate among patients with fat invasion and those with renal vein invasion with or without fat invasion. In our study, we hypothesized that tumor growth into sinus fat and/or renal vein could facilitate the wide spread of the disease due to the rich lymphatic and vascular tissues present in this compartment. This factor in addition to the absence of the barrier capsular layer could lead to worse oncological outcomes when compared with tumors with perinephric fat infiltration. However, when comparing both types of invasions in the pT3a stage, individually or in combination, none was associated with worse outcomes.
Among the six cases converted intraoperatively to a robotic RN, all patients are alive without local recurrence or metastasis. This also supports the rational for attempting NSS in selected T3a cases and the oncological safety of conversion to RN if necessary.
The present study has some limitations that should be acknowledged. First, although a prospective database was used, it has a retrospective design and even with a match comparison, the groups could be prone to a selection bias. Finally, the cohort's follow-up is relatively short, especially when oncological safety is in debate; however, as a relative new technique, long-term follow-up series are still lacking in the robotic surgery literature and further studies will be required to validate our findings.
Conclusions
Patients with localized pT3a RCC treated with RPN had similar short-term oncological and better renal functional outcomes compared with similar cases treated by RN. With the growing experience in the minimally invasive robotic surgery, suspicion for pathological T3a disease should not be a deterring factor for performing NSS when it is technically feasible by skilled surgeons.
Footnotes
Acknowledgments
Dr. Andrade was supported by a grant from CAPES foundation: Ministry of Education of Brazil; and FFM: HCFMUSP Funding Agency.
Author Disclosure Statement
J.H.K. is a consultant for Endocare. No competing financial interests exist for the other authors.