
Abstract
Objective:
To assess whether morphometric and clinical parameters influence accessibility to the upper calyx through a lower calyx tract during supine percutaneous nephrolithotomy (SPCNL).
Patients and Methods:
Data for 114 consecutive SPCNLs performed between June 2014 and March 2016 in an academic medical center were analyzed. Successful approachability was defined as rigid nephroscopic access to the upper calyx introduced through a lower calyx access as attested by direct visualization of the upper calyx papillae and position of the nephroscope on intraoperative pyelography. Demographic, morphometric, and clinical parameters were assessed. Analysis of variance, Fisher's exact, chi-square tests, and univariate and multivariate models were applied.
Results:
Successful approach was achieved in 94 (82%) patients. In univariate analyses previous kidney operations (p = 0.03), body weight (p = 0.04), and acute lower calyx access to the upper calyx axis angle (p = 0.01E-13) correlated with failed access. Multivariate analyses revealed that an acute angle was the sole independent factor for failed access (odds ratio [OR] 1.4, p < 0.05; confidence interval [95% CI] 1.021, 2.035). Limitations include the inability to objectively determine the mobility of the kidney as a co-factor in successful approachability.
Conclusions:
SPCNL offers effective endoscopic accessibility through a lower calyx access. Previous kidney operations and body weight tend to negatively influence this accessibility. An acute angle between the lower calyx and the upper calyx is the single independent factor associated with failed accessibility.
Introduction
I
Our current aim was to further assess whether factors other than anatomical ones, such as morphometric data and clinical features, might limit efficient access to the collecting system through a lower calyx in SPCNL in a large series of patients.
Patients and Methods
All 124 patients referred for percutaneous procedures from June 2014 to March, 2016 were considered as being eligible for prospective and consecutive enrollment in this study. Ten patients were excluded, four of them for having undergone PPCNL because of the interposition of intraabdominal organs (i.e., liver, bowel, spleen) that precluded a supine access (as assessed by preoperative cross-sectional imaging), and six who underwent percutaneous resection of upper-tract urothelial carcinoma, a pathology that was not our point of interest in this study. The final study group was comprised of 114 patients.
The study patients were placed in a supine position and the lower posterior calyx was punctured, serving as our first and principal access. Our basic surgical approach consisted of general anesthesia, retrograde pyelography through a 5F open-ended ureteral catheter, and renal puncture under combined ultrasonographic and monoplanar anteroposterior fluoroscopic guidance. Our techniques have been reported in greater detail elsewhere. 13,14 The operations were performed in the tubeless fashion, thus avoiding postoperative nephrostomy tubes, and an internal stent was left in place for 5 days. The approachability to the upper calyx was assessed using rigid 18F to 21F nephroscopes (Richard Wolf Medical Instruments Corporation, Vernon Hills, IL). It was considered successful when the upper calyx papillae were endoscopically identified in the center of the operative field and the position of the nephroscope in the upper calyx was confirmed by intraoperative pyelography. The ECIRS technique 15 using a Flex-X2 ureteroscope (Karl Storz, Tuttlingen, Germany) was applied whenever the anatomical position of the lower calyx did not allow for endoscopic access to the entire intrarenal collecting system either by rigid or by flexible nephroscopes.
The analyzed demographic, clinical, morphometric, and anatomic parameters were as follows: age, gender, side, stone area (mm2), type of stone (staghorn vs nonstaghorn), previous ipsilateral renal operations (yes or no), operative time (minutes), hospital stay (days), height (cm), weight (kg), body mass index (BMI [kg/m2]), body circumference at chest, waist, and hip levels (cm), and the angle between the tract axis and the upper calyx longitudinal axis as measured on the intraoperative pyelography.
Statistical analyses were done using SPSS® employing comparisons of continuous data by analysis of variance and discrete variables by Fisher's exact and chi-square tests, defining significance at a p-value <0.05. A multivariate model and a logistic regression analysis, including parameters with a p-value <0.2 in the univariate evaluation, complemented the statistical analysis.
Results
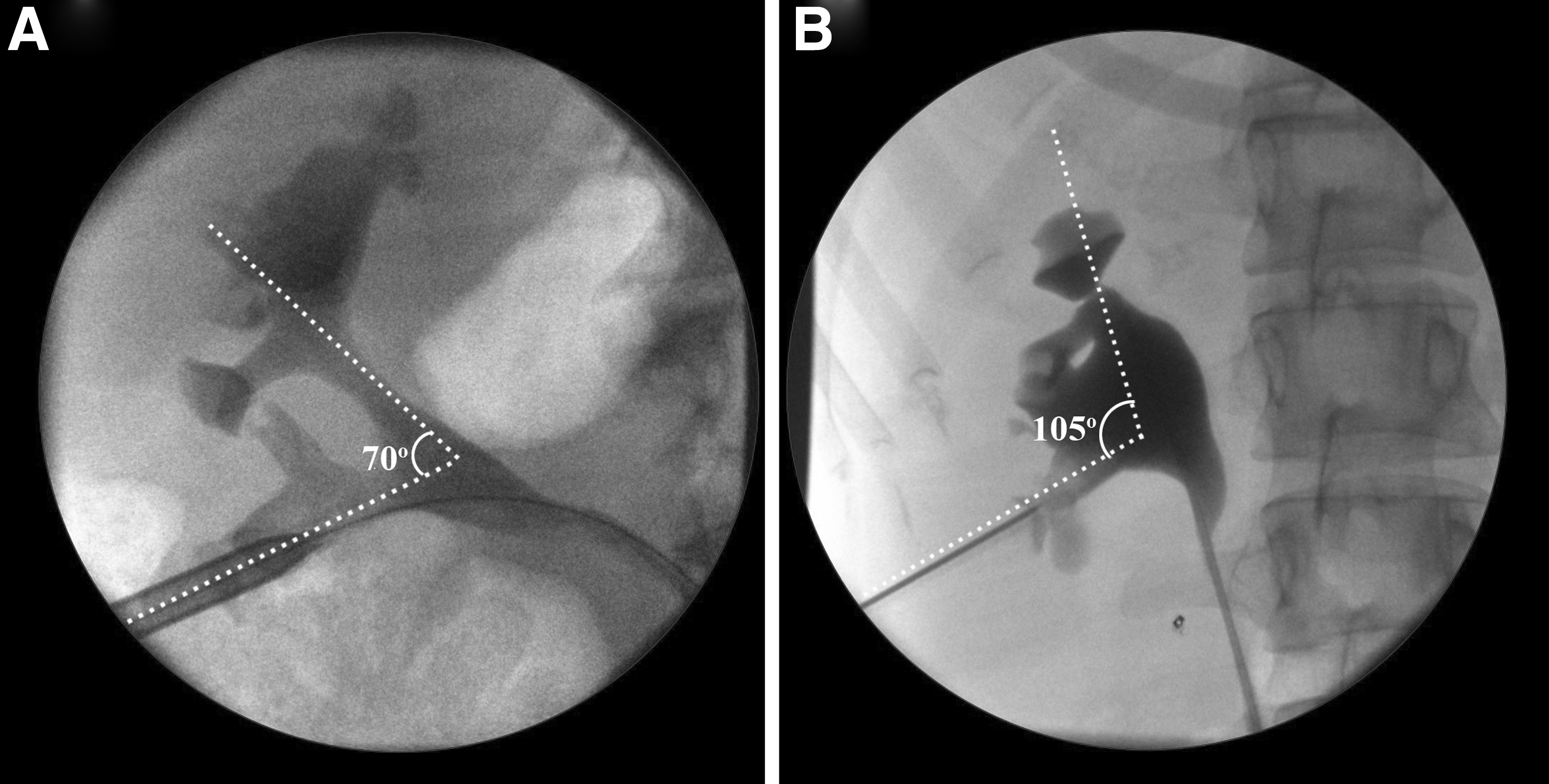
A successful endoscopic approach to the upper calyx through the lower calyx access by means of a rigid nephroscope was achieved in 94 (82%) patients who underwent SPCNL. Univariate analysis revealed that previous renal operations (p = 0.03), body weight (p = 0.04), and an acute angle between the lower and upper calices axes (p = 0.01E-13) correlated with a failed approach (Table 1). None of the other anatomical, morphometric, or clinical parameters influenced the results. The multivariate model and the logistic regression analysis revealed only an acute lower calyx-upper calyx angle as being an independent factor associated with endoscopic approachability (odds ratio [OR] 1.4, p < 0.05; confidence interval [95% CI] 1.021, 2.035) (Table 2). Examples of an acute angle that interferes with accessibility and a wide angle that permits an upper calyx approach through a lower calyx puncture are showed in Figure 1. None of the patients needed more than the lower calyx puncture. The positive predictive value of the angle between the lower calyx and the upper calyx axis for a successful approach to the upper calyx through a lower calyx puncture is presented in Figure 2. ECIRS was needed in four (4%) successful cases and in four (22%) failed cases (p = 0.03). All ECIRS procedures were performed on patients with complete staghorn stones.
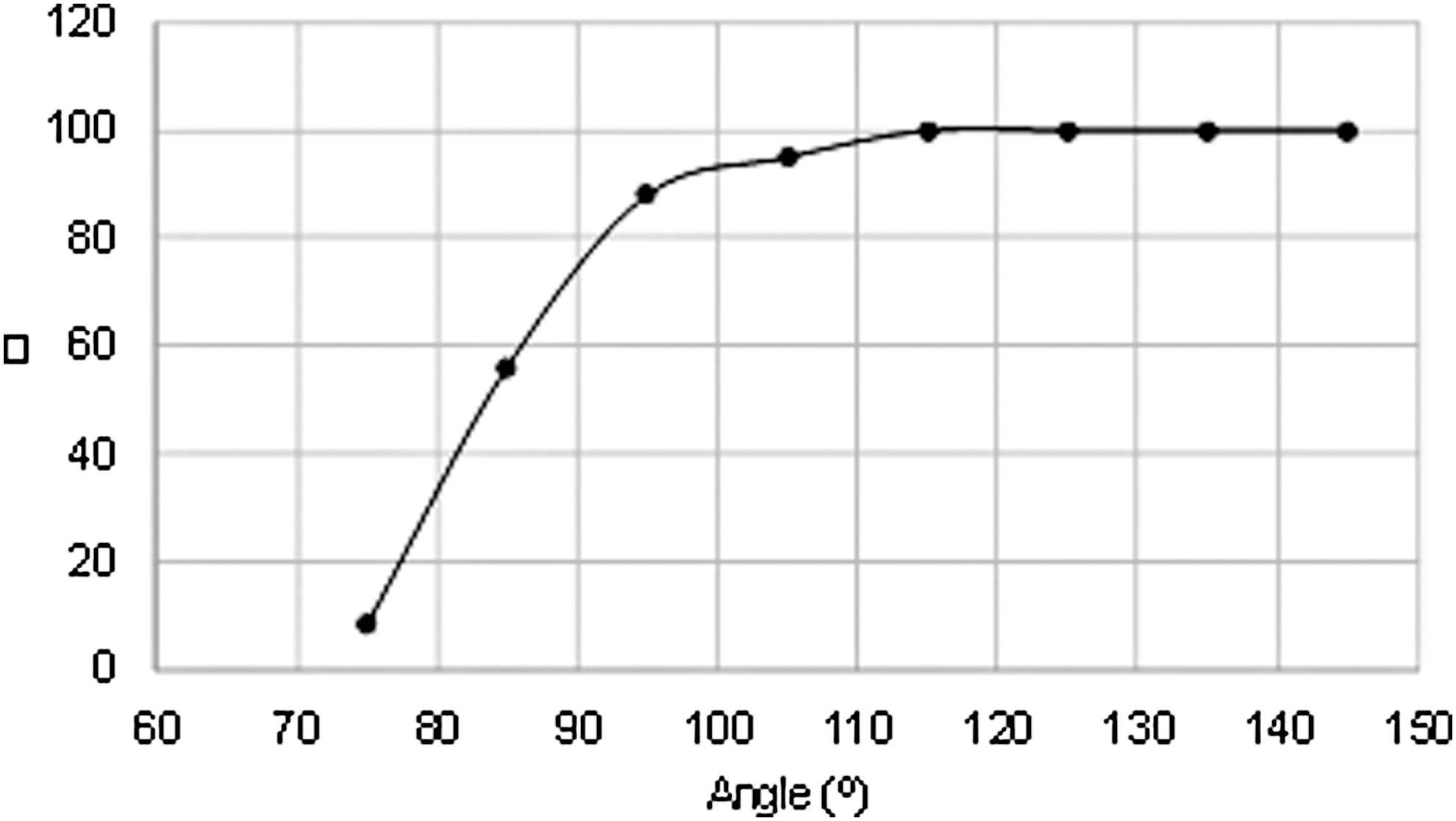
The positive predictive value of the angle between the lower calyx and the upper calyx axis for accessibility to the upper calyx through a lower calyx puncture.
Average.
Tubeless operations were performed in 106 (93%) patients, 101 (89%) of them with placement of an internal stent and five (4%) in a totally tubeless fashion. Nephrostomy tubes were placed in eight (7%) patients due to bleeding that obscured the surgeon's view and did not allow assurance of complete clearance of the stones. The bleeding in each of those cases originated from the parenchyma at the site of the puncture and it was not related to the assessment of the upper pole approachability. Blood transfusion was administered to three (2.6%) patients. A postoperative noncontrast computed tomography scan showed residual fragments in five of the nephrostomy tube patients, and they were treated with a second-look SPCNL using the nephrostomy tube tract and during the same hospitalization. The patients in the tubeless group were assessed for stone clearance by the noncontrast computed tomography scan at the first follow-up, which was held at an average postoperative period of 6 weeks (range 5–9). Following this protocol, 100 (88%) patients were diagnosed as being stone-free following the primary surgery. Six (5%) patients were additionally treated by ureteroscopy and retrograde intrarenal surgery, resulting in a final overall stone-free rate of 93%. The remaining eight (7%) patients with residual fragments were left for observation. The residual stones were located as follows: nine (64%) in the lower calyx, two (14%) in the renal pelvis, two (14%) in the mid-upper calyx, and one (7%) in the upper calyx. Eight (8/94; 9%) of the residual stones were found in the successful upper calyx-accessed group and six (6/20; 30%) in the unsuccessful upper calyx-accessed group (p < 0.05).
The overall complications rate was 11%, involving six (5%) patients with urinary tract infection, three (3%) patients with perioperative bleeding, and one (1%) patient each with positional injury of the right shoulder, a single functioning kidney with obstructive uropathy due to distal ureteral stone load, and delayed bleeding due to an arteriovenous fistula treated by selective angioembolization.
Discussion
There are numerous publications attesting to the idea that the pioneers of PCNL had intuitively chosen the prone position for patients undergoing the procedure. 16 –19 Although none of those early reports provided any rationale for their choice as opposed to alternative positions, it became the standard and remained the singular position for almost two decades. 5 The advantages of this position were described later, and they included short access to the posterior calyces situated on the avascular line of Brödel, reduced risks of other viscera interposition along the working tract, and a large available area for puncture. 4 PPCNLs have been widely popularized, and they have now entirely replaced open surgery: specific indications for them have been established, and both their success and complication rates have been well described. 20,21 In addition, experience gained with large series of patients led to the conclusion that staghorn stones should be approached with the patient in a prone position through an upper calyx access. This choice of access takes advantage of the renal anatomical features of the upper calyx axis being aligned to the ureteropelvic junction, thereby allowing endoscopic accessibility to the upper, lower, and most of the middle calyces. 11,12 However, most of the upper calyx punctures are supracostal and significantly increase the complication rates and their severity. 12,21
The introduction of SPCNL in the 90s opened new horizons. The advantages of this approach over the PPCNL are facile single positioning of the patients throughout the entire procedure, no limitations in ventilating the patients, better access of the anesthesiologist, the enabling of ECIRS, and significant improvement in the ergonomic environment of the surgeon who may choose to operate while seated. 1,5,21 Various positional refinements of Valdivia's original description increased the applicability of this procedure while reducing its initial limitations. 6 –8
Despite all of these reports in its favor, the popularity of SPCNL is still limited. 9 This reluctance to implement SPCNL probably derives from conservatism, tradition, and beliefs that tracts are longer in the supine position and that SPCNL is not effective in the treatment of staghorn and complex stones. 11,12 We recently addressed this paradigm by showing that the tracts to the lower calyx are shorter and that the spatial anatomy of the kidney offers a reliable lower calyx access to most of the intrarenal collecting system when the patient is in the supine position, similarly as when coming from the upper calyx in the prone position. 13 In that study, anatomical factors were assessed as they appeared on three-dimensional cross-sectional imaging in correlation to the intraoperative outcome. This study was designed to further validate our earlier conclusions in a large series of patients.
We also addressed the questions of which, if any, clinical and morphometric factors might interfere with the effectiveness of lower calyx access in SPCNL—these issues have been raised during international meetings by our colleagues. We found that the patient's body weight and previous renal surgery may have some negative influence on the accessibility to the surgical site, but only the angle between the lower calyx and upper calyx axis was associated with the endoscopic effectiveness of such an approach. Our accessibility rate of >80% in this study reproduced the results of our previous work, supporting the concept that complex and staghorn stones can be effectively addressed through a lower calyx in SPCNLs. This result can be better conceptualized by comparing the difference of the site of access in supine and prone positions. The anatomical position of the kidney with the lower pole located anterolateral and the upper pole located posteromedial effectively endoscopically exposes the collecting system from the lower calyx in the supine position and from the upper calyx in the prone position. The significantly wider lower-to-upper calyx angle in the supine position allows for accessibility to most of the intrarenal collecting system. Additionally, considering that a supine position facilitates performance of ECIRS using flexible ureteroscopes in a retrograde fashion, the approach to a large and complex stone in this position becomes a more attractive option. 2,3,15 It offers the advantage of avoiding the more risky upper pole access that is needed in such cases when the patient is in a prone position.
One possible limitation of this study may be our impression that the kidney is more mobile when it passively lies on the psoas muscle without consequential anterior compression, thus allowing easy horizontal-oblique movements of the nephroscopes when the patient is in a supine position. In contrast, the surgeon encounters the resistance of the more massive body wall and relatively immobile kidney compressed between the psoas muscle and the anterior body content when the patient is in the prone position. The level of kidney mobility could not be objectively quantified. As such, this parameter remains subjectively interpreted, and it is not clear to what extent, if any, it influences accessibility to the collecting system. However, in the eventuality that it does play a role, it can be considered as being another advantage of surgery in the supine position.
Our aim was not to claim superiority of SPCNL over PPCNL, but rather to disclose and address prejudices associated with SPCNL in terms of its effectiveness in complex stone situations and to show its similarity to PPCNL in terms of stone-free status. It should be borne in mind that a successful PCNL is defined by complete stone clearance without complications and that each surgeon should perform it in the position in which these goals can be achieved.
Conclusion
There is highly satisfactory accessibility of the upper calyx through a lower calyx by means of a rigid scope and with the patient in a supine position. The patient's weight and previous renal surgery may have a negative influence on that accessibility, however, a wide angle between the lower calyx tract and the upper calyx is the sole independent factor that facilitates it. The availability of flexible nephroscopes and ureteroscopes permits overcoming the limited accessibility found in a minority of these cases, making SPCNL effective even in highly complex surgeries. We hope that our studies contribute to greater awareness of this procedure as a viable option for treating complex cases of renal stones.
Footnotes
Author Disclosure Statement
No competing financial interests exist.