
Abstract
Purpose:
To report early operative outcomes and assess continence in 100 consecutive patients who underwent Retzius-sparing robotic-assisted laparoscopic radical prostatectomy (RALP).
Materials and Methods:
This was a prospective, single-center, consecutive case series of 100 and 100 patients undergoing a Retzius-sparing and a conventional RALP, respectively, by a single surgeon between March 2015 and April 2017.
Results:
Baseline patient characteristics were similar between the two groups. The Retzius-sparing approach required significantly less console time (120.0 minutes vs 144.0 minutes, p < 0.001). There were no differences between intra- and post-operative complication rates, and hospital length of stay was similar in the two groups. Incidence of positive surgical margins was nonsignificantly different between the two groups, with 17% and 13% of pT2 patients and 49% and 48% of pT3 patients in the Retzius-sparing and conventional groups, respectively. Patients in the Retzius-sparing group had significantly superior rates of achieving post-operative urinary continence (log-rank test: p < 0.001), with 20% of patients continent within the first month, compared with 8% of patients in the conventional group. The mean number of pads per day needed at 3, 6, 9, and 12 months post-operatively was also significantly lower in the Retzius-sparing group.
Conclusions:
Retzius-sparing RALP requires shorter console time, is oncologically safe, and leads to significantly superior continence outcomes compared with conventional RALP.
Introduction
R
Almost all RALP techniques to date currently involve dropping the bladder and entering the Retzius space at some point during surgery. 2 Technique advances that preserve as much normal anatomy as possible are likely to improve post-operative functional outcomes. Galfano and colleagues recently reported their initial success using a novel Retzius-sparing RALP approach, with their study cohort of 200 patients having excellent oncological and functional outcomes. 6,7 In light of these advances, we compared the peri-operative, oncologic, and functional outcomes of patients undergoing a Retzius-sparing RALP with those undergoing a conventional RALP.
Materials and Methods
Study design, setting, and participants
This was a prospective, single-center case series of 200 consecutive patients undergoing RALP between March 2015 and April 2017. One hundred consecutive patients underwent a conventional RALP, followed by 100 patients who underwent a Retzius-sparing RALP. All procedures were performed by a single surgeon (R.M.) at a single institution (Augusta University Medical Center in Augusta, GA). Institutional review board ethics approval was obtained before study initiation.
Baseline patient characteristics recorded at the pre-operative clinic visit included: age, body mass index (BMI), ethnicity, clinical stage, biopsy Gleason score, number of positive biopsy cores, last pre-operative prostate-specific antigen (PSA) level, and the American Society of Anesthesia (ASA) physical status classification system score. Patients' lower urinary tract symptoms were assessed at baseline by using the International Prostate Symptom Score (IPSS), including the quality of life (QoL) question.
Intra-operative outcomes were recorded immediately after surgery by using a standardized, IRB-approved research form. Tissues specimens were handled and analyzed according to the latest International Society of Urological Pathology recommendations. 8 Patients were managed routinely post-operatively, and they were followed up on post-operative day 7–14 for a cystogram before Foley catheter removal. Surgical specimen pathology data was available from patients' medical records. Follow-up data were only available for patients who returned for a post-operative clinic visit, typically at 3-month intervals. At each follow-up visit, patients had PSA levels measured, were asked about number of pads used per day, and completed the IPSS questionnaire.
Study objectives
The primary study objective was to compare post-operative urinary continence outcomes between the two groups. Urinary outcomes were assessed as rates of re-establishing urinary continence after surgery, proportion of patients who had early return-to-continence, and patient-reported mean number of pads used per day. Secondary study objectives were to compare peri- and post-operative, oncologic, and lower urinary tract symptom outcomes between the two groups. Oncological outcomes were assessed by using proportions of patients who had positive surgical margins. Lower urinary tract symptoms were evaluated by using the IPSS questionnaire.
Outcomes definitions
Urinary continence was defined as using zero or one precautionary pad per day. A pad was defined as precautionary if the patient reported during a post-operative visit that he used the pad as a precautionary measure and that it was not wet by the end of the day. Patients were considered to have had early continence if they achieved continence within 1 month of surgery.
Patients filled IPSS and incontinence score questionnaires on their routine post-operative visits.
Retzius-sparing RALP technique
Our technique was closely similar to that described by Galfano and colleagues.
6
It has been previously detailed and publicly shared by our team on YouTube. (
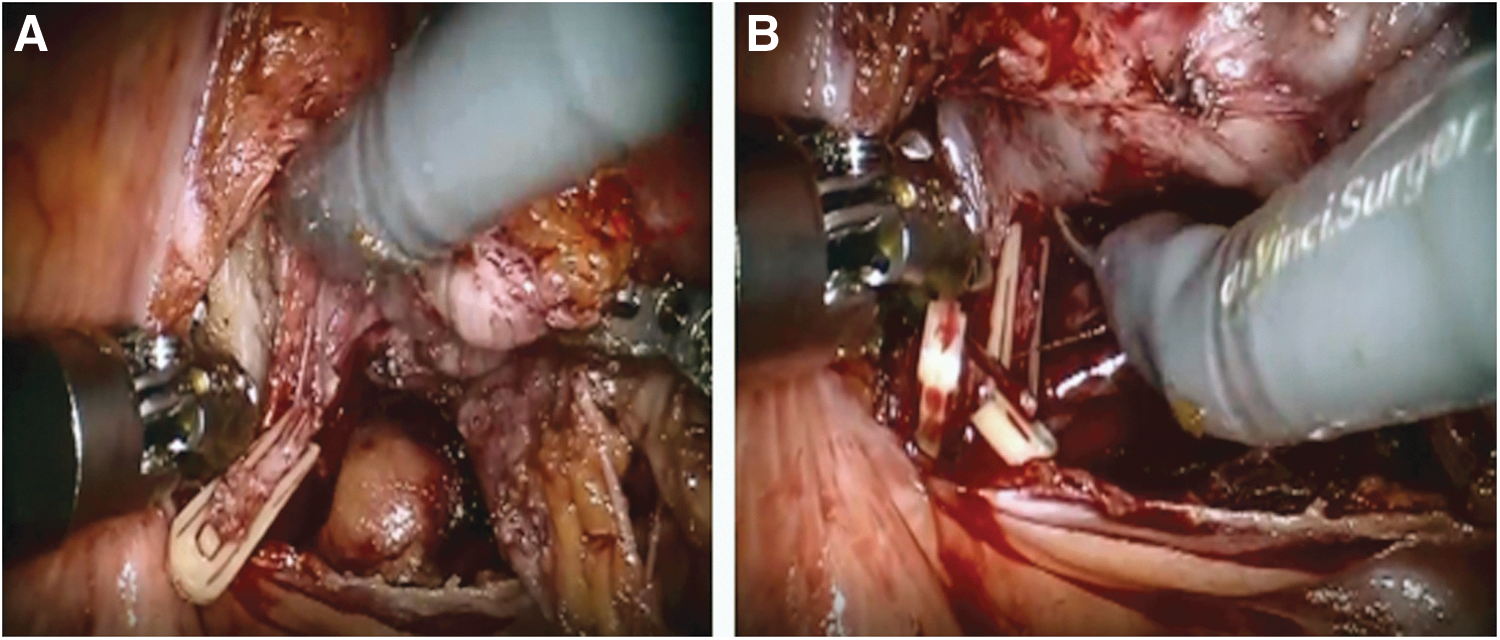
Step 1: posterior dissection
The peritoneum overlying the vas deferens and the seminal vesicles was incised, and the vas deferens and the seminal vesicles were controlled by using sharp and blunt dissections.
The key step involved identification of the initial prostate pedicle, which was found by lifting the seminal vesicle and developing a 0.5–1 cm space postero-lateral to the junction of the seminal vesicle and prostate base (Fig. 1A). Further control of the prostate pedicles and, if necessary, dropping of the prostatic fascia was then performed. Absorbable clips (Covidien Lapro-clip©) or bipolar cautery were used to achieve hemostasis (Fig. 1B).
(
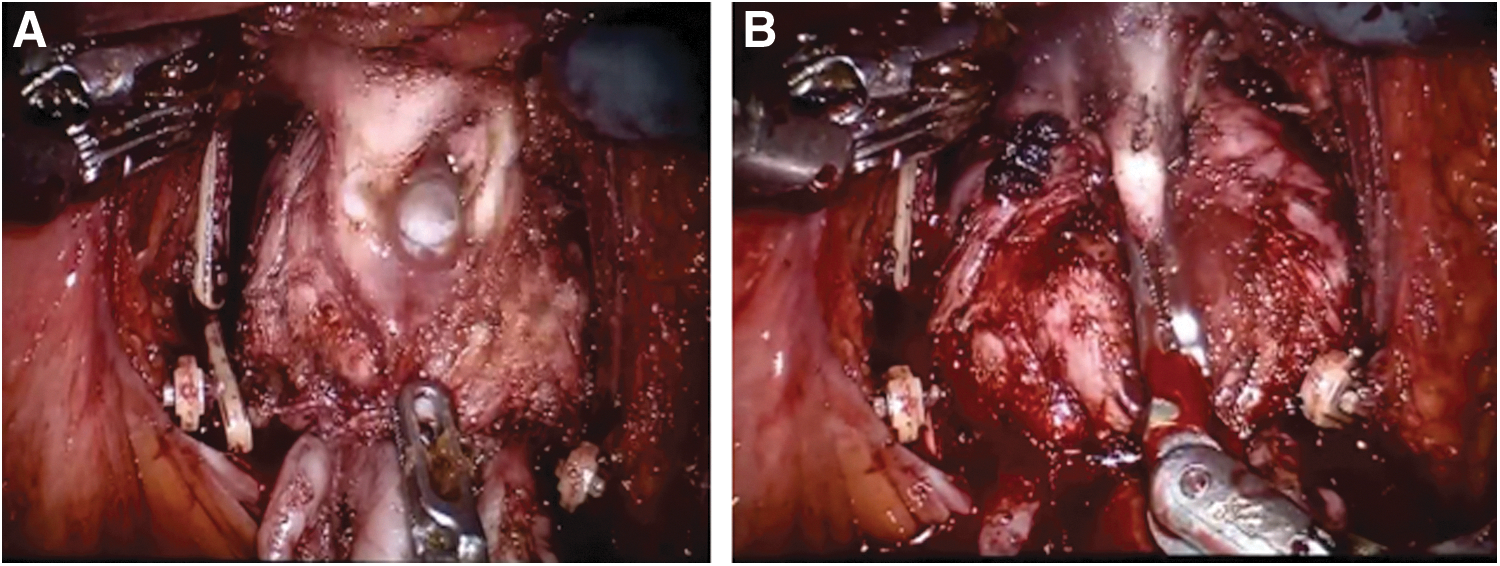
Step 2: identification and incision of the bladder neck
The bladder neck was identified via anterolateral dissection. Bladder attachments were controlled by using bipolar cautery. Efforts were made to clearly identify the posterior and anterior bladder neck before dividing them. The posterior bladder neck was initially incised, followed by incision of the anterior portion (Fig. 2A). The prostate was then dropped posteriorly, and cephalad retraction was applied to expose the anterior prostatic apex (Fig. 2B).
(
Step 3: incision of the urethra and anastomosis
The dorsal veins were controlled by using a bipolar cautery. The urethra was then identified and incised (Fig. 3). After the urethral incision, the whole prostate was subsequently freed and placed in an Endo Catch™ bag for later retrieval. Pelvic lymph node dissection was performed at this stage. The urethro-vesical anastomosis was performed by initially bringing the anterior bladder neck proximal to the anterior urethra (Fig. 4). We used a running technique with absorbable 3-0 braided sutures (Covidien V-loc) in our anastomosis.
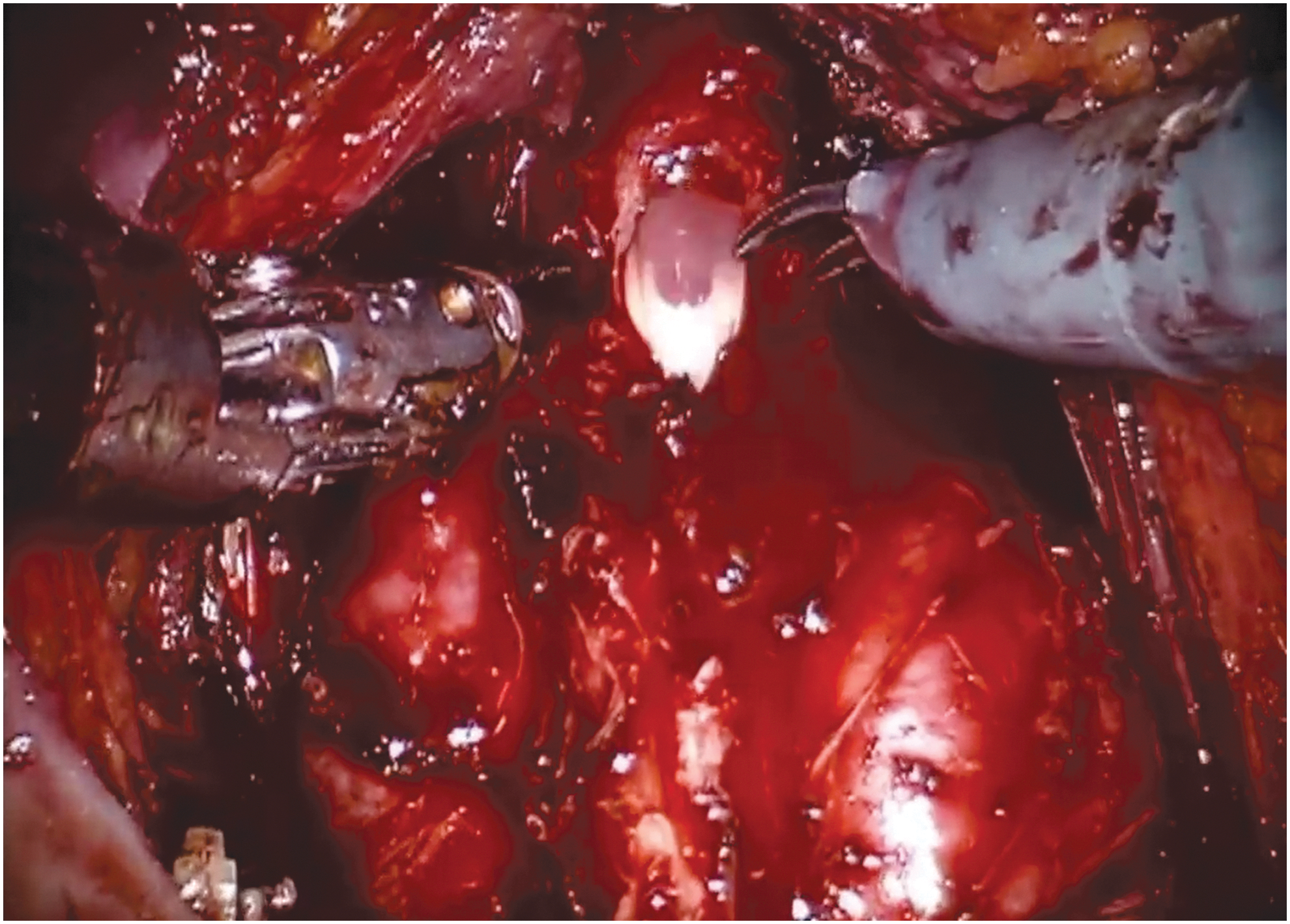
Control of dorsal veins using bipolar cautery and urethral division.
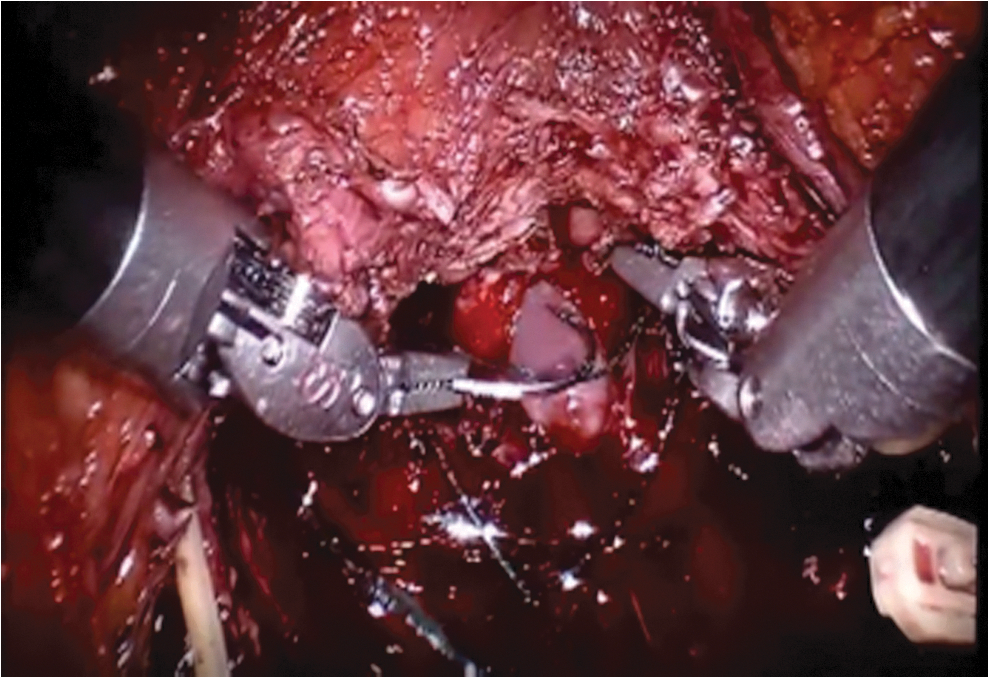
Urethro-vesical anastomosis.
Conventional technique
As for the conventional technique, we used the posterior approach, with the vas deferens and seminal vesicles identified first. The bladder was then dropped, and the prostate was removed in an antegrade fashion. In an effort to improve post-operative continence outcomes, we routinely performed an anterior reconstruction and hitching of the urethra (Supplementary Fig. S1; Supplementary Data are available online at
Statistical analysis
Mean, median, standard deviation, and interquartile ranges were used to describe continuous variables, whereas frequencies and proportions were used for categorical variables. Student's t-test and Fisher's exact test were used to compare continuous variables, whereas the Chi-square test was used for categorical variables. One-minus survival functions were used to determine rates of continence post-RALP. Continence rates between the two study groups were compared by using the log-rank test. Statistical significance was set at p < 0.05. All analyses were performed by using R version 3.3.1 (The R Foundation for Statistical Computing, Vienna, Austria).
Results
Median patient ages in the Retzius-sparing and conventional groups were 61.0 and 62.0, respectively. Median follow-up time was 210 days (interquartile range: 90.0–270.0). Patients' baseline characteristics are displayed in Table 1. There were no significant differences with respect to patient age, BMI, ethnicity, clinical stage, biopsy Gleason score, number of biopsy cores involved, pre-operative PSA level, D'Amico risk group classification, and IPSS and ASA physical status classification system scores between the two groups (Table 1).
Student's t-test.
Fisher's exact test.
Chi-square test.
ASA = American Society of Anesthesia; BMI = body mass index; IPSS = International Prostate Symptom Score; IQR = interquartile range; PSA = prostate-specific antigen; RALP = robotic-assisted laparoscopic radical prostatectomy.
Retzius-sparing RALP required significantly less console time compared with conventional RALP (120 minutes vs 144 minutes, p < 0.001). Bladder neck sparing was performed in 88% of Retzius-sparing RALPs compared with 71% of conventional RALPs (p < 0.001). There were no significant differences in number of intra- or post-operative complications, estimated blood loss, hematocrit on discharge, number of needed transfusions, or length of hospital stay (Tables 2 and 3).
Denotes statistical significance.
Student's t-test.
Chi-square test.
Fisher's exact test.
Denotes statistical significance.
Student's t-test.
Chi-square test.
Fisher's exact test.
With respect to final pathological outcomes, median prostate mass of patients in the Retzius-sparing group was significantly less compared with the conventional group (44.6 g vs 48.0 g, p = 0.03). Thirty-four percent of patients in the Retzius-sparing group had pT3 or disease or worse, compared with 23% in the conventional group (p = 0.08). Bladder neck invasion was more prevalent in the Retzius-sparing group (16% vs 6%, p = 0.02). As for positive surgical margins, 11 (16.7%) patients with ≤pT2 disease in the Retzius-sparing group had positive margins, compared with 10 (13%) in the conventional group (p = 0.54). Conversely, 16 (47.1%) patients with ≥pT3 disease in the Retzius-sparing group had positive margins, compared with 11 (47.8%) patients undergoing conventional RALP (p = 0.95). There were no significant differences with regards to distribution of positive margin locations. Eleven patients (11%) in the Retzius-sparing group and 12 (12%) in the conventional group had positive lymph nodes.
Median time to continence in the Retzius-sparing group was 90.0 days, compared with 160.0 days in the conventional group (p < 0.001). Twenty patients (20%) in the Retzius-sparing group never leaked, compared with only two (2%) in the conventional group (p < 0.001) (Table 4). Figure 5 illustrates the rates of re-establishing urinary continence after surgery. Patients in the Retzius-sparing group had significantly superior post-operative urinary continence rates (log-rank test: p < 0.001). After 3 months of follow-up, 59.0% (95% confidence interval [CI]: 46.2, 69.5) of patients in the Retzius-sparing group had achieved urinary continence, compared with 29.1% (95% CI: 18.9, 38.4) of those in the conventional group. The corresponding proportions after 6, 9, and 12 months of follow-up were: 80.7% (95% CI: 66.9, 89.3), 89.7% (76.5, 95.3), and 97.5% (82.8, 99.5), respectively, in the Retzius-sparing group, compared with 50.3% (39.3, 59.9), 63.3% (51.1, 72.2), and 68.5% (56.0, 77.6), respectively, in the conventional arm (Fig. 5). The numbers of pads needed per day at 3, 6, 9, and 12 months post-RALP were significantly lower in the Retzius-sparing group (Table 4). With respect to urinary symptoms, both the mean IPSS (7.6 vs 12.0, p = 0.002) and QoL scores (2.2 vs 3.4, p < 0.001) were significantly better in the Retzius-sparing group after 6 months of surgery (Table 5).
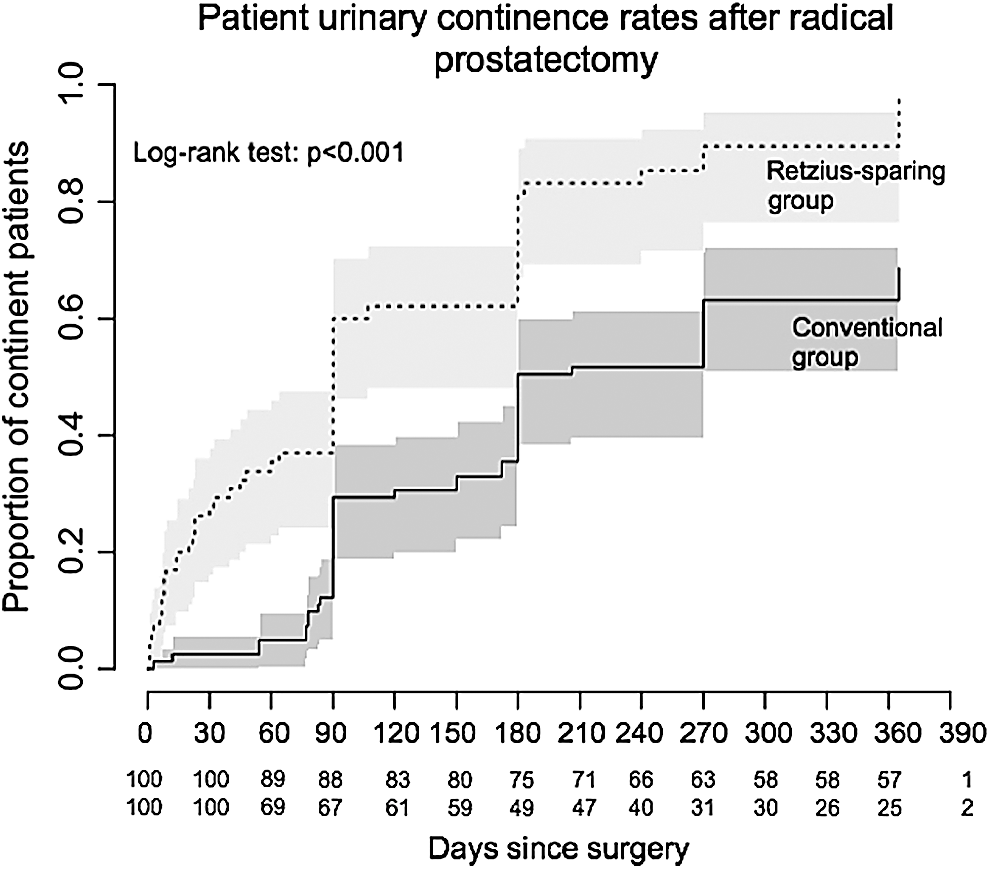
Patient urinary continence rates after radical prostatectomy.
Denotes statistical significance.
Student's t-test.
Fisher's exact test.
SD = standard deviation.
Student's t-test.
Denotes statistical significance.
QoL = quality of life.
Discussion
This is the largest prospective series to date comparing the peri-operative, continence, and oncological outcomes of patients undergoing a Retzius-sparing RALP with those undergoing a conventional RALP. Retzius-sparing RALP required a significantly shorter console time. Compared with patients who underwent a conventional RALP, patients in the Retzius-sparing group had significantly superior continence rates after surgery, with almost 20% of patients never leaking after surgery. Further, the number of pads needed per day within the first year after surgery was also significantly lower in patients undergoing this novel technique.
Reassuringly, the proportions of patients with a positive surgical margin were similar across the two groups. Surgical margin status, which is commonly used as a surrogate for long-term oncologic outcomes, 9 is a known predictor of biochemical recurrence and prostate cancer-specific mortality. 10 –13 Thus, the nonsignificant differences in surgical margin status are reassuring. We are currently collecting data on PSA recurrence at 3, 6, 9, and 12 months, respectively.
Galfano and colleagues were the first to describe the Retzius-sparing RALP approach and recently reported the functional and oncologic outcomes of 200 patients operated using this approach. 7 Importantly, they demonstrated that the Retzius-sparing approach was oncologically safe, with positive surgical margins recorded in 15% and 45% of patients with pT2 and pT3 cancers, respectively. These are similar to our reported outcomes of 17% and 47%, respectively. They also demonstrated that this approach was associated with high early continence rates, which is also consistent with our results. 7 The major limitation of this study was the lack of a control group (i.e., patients undergoing conventional RALP) with which to compare functional and oncological outcomes. By including a comparison group of 100 patients undergoing conventional RALP, we have addressed this limitation by comparing outcomes of this novel approach with those of patients who underwent the procedure that is currently accepted as standard of care.
Lim and colleagues compared the peri-operative, oncological, and continence outcomes of 50 patients who underwent a Retzius-sparing RALP with 50 matched patients who underwent conventional RALP. Similar to our findings, they demonstrated that the Retzius-sparing approach needed significantly less console time, was oncologically safe with respect to positive surgical margins, and was associated with superior urinary continence outcomes. 14 Dalela and colleagues also recently compared, in a randomized controlled trial setting, the same outcomes in 60 patients undergoing Retzius-sparing RALP with 60 patients undergoing conventional RALP. Their results confirmed that the Retzius-sparing approach is associated with superior urinary continence outcomes, although with a nonsignificantly higher positive surgical margin rate (25% in the Retzius-sparing arm vs 13% in the conventional arm, p = 0.1). 15 The study was restricted to patients with low-intermediate-risk prostate cancer (per the National Comprehensive Cancer Network guidelines), as opposed to our study, which included patients of all risk categories. We believe that including patients of any risk group increases the external validity of our results and confirms the safety/efficacy of this approach in all prospective patients.
Our study has several important strengths. To the best of our knowledge, this is the largest series to date comparing oncological and continence outcomes of patients undergoing a Retzius-sparing RALP with those undergoing conventional RALP. All RALPs were performed by the same surgeon (R.M.), thus precluding the possibility of inter-surgeon variability with regards to oncologic and functional outcomes. 16 The surgeon is a fellowship trained urologist oncologist and minimally invasive surgeon and has more than 10 years of experience performing robotic surgery. Limitations include the nonrandomized nature of the study. Although patients were nonsignificantly different with regards to baseline characteristics (Table 1), future randomized studies that balance out potential unmeasured confounders are warranted. We did not account for the learning curve effect that is typically associated with novel techniques. 7,9 Our study also lacked long-term follow-up data for all included patients. Three-month continence outcomes were available for only 67% and 88% of patients in the Retzius-sparing and conventional groups, respectively. The reporting of continence is not ideal, and it is based on subjective patient reporting during post-operative visits. Ideally, it should be more objective and based on pad weighing. Post-operative erectile function was also not compared between the two groups as International Index of Erectile Function scores were not available for a large portion of these patients both pre- and post-operatively. Long-term oncologic outcomes data was also unavailable for these patients. Continued oncologic follow-up for these patients will need to be reported in the future to conclusively compare oncologic outcomes.
Conclusions
This is the largest prospective series to date comparing the peri-operative, oncologic, and functional outcomes of Retzius-sparing RALP and conventional RALP. Retzius-sparing RALP requires shorter console time, is oncologically safe, and is associated with markedly improved short- and long-term continence outcomes. The Retzius-sparing approach is an acceptable choice for prostate cancer patients being considered for RALP.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.