
Abstract
Background and Purpose:
Temporary drainage of the upper urinary tract after ureterorenoscopy for the treatment of urinary stones is almost a routine in endourologic practice. In these cases, a Double-J stent (DJS) is left for 7 or more days. In borderline cases, a ureteral catheter attached to the urethral catheter may be left for 24–48 hours. In some situations, tubeless approach is possible. The purpose of this study was to evaluate the necessity and immediate postoperative implications of upper tract drainage by comparing complications and symptoms at the immediate postoperative period in these three groups of patients.
Materials and Methods:
A database of 516 consecutive patients who underwent ureterorenoscopy for ureteral and/or renal stones between October 2014 and September 2016 was retrospectively evaluated. The cohort was divided according to postoperative drainage type of the upper urinary tract. The data consisted of demographic parameters, stone location, number and burden, severity of preoperative obstruction, and postoperative complications. Symptoms at the immediate postoperative period, assessed by visual analog scale (VAS) score, frequency, and type of analgesics used, were evaluated and compared. Categorical dependent variables were evaluated using chi-square or Spearman's correlation tests, whereas continuous dependent variables were analyzed using Pearson correlation analysis.
Results:
There were 196 (38%) tubeless, 214 (41%) UC, and 106 (21%) DJS cases. Patients who were drained with DJS at the end of the procedure were significantly with higher stone volume (p < 0.005), higher stone density (p < 0.005), and with more severe preoperative obstruction (p < 0.005). Postoperative complications (infection, stone-street, and acute renal failure), mean VAS score, or analgesics used were not different in the three subgroups.
Conclusions:
A tubeless approach is safe in properly selected cases. There is no difference in postoperative course compared with drained groups. Tubeless procedures may facilitate an outpatient approach for treatment of upper urinary tract stones.
Introduction
T
Materials and Methods
After Institutional Review Board approval, a cohort of 516 consecutive patients who underwent ureteroscopy or ureterorenoscopy for ureteral and/or renal stones was evaluated. The average stone burden and stone density were determined using noncontrast abdominal CT scan. In case of multiple stones, we measured the total stone volume and the average HU of all treated stones.
All patients were operated by the same experienced endourologist and one or two fellows in lithotomy position under general anesthesia. Stones located below the iliac vessels were treated using a 6.5F semirigid ureteroscope and 550 μm laser fiber, whereas other ureteral or renal stones were treated using 7.5F flexible ureteroscope and 200 μm laser fiber. When a semirigid ureteroscope was used, stones were fragmented and pulled out using a 2.2F Nitinol basket, whereas when the flexible ureteroscope was used, a dusting technique without using an access sheath was applied. The procedure was terminated when there were no apparent stone fragments left in the ureter or complete renal stone dusting was achieved. In patients with a high stone burden, severe preoperative hydronephrosis, impacted ureteral stones, previous infection, or when there was a doubt of incomplete fragmentation, a DJS was inserted at the end of the procedure. Patients with relatively small stone volume; without previous chronic obstruction, intraoperative ureteral edema, or trauma; and evidence of efficient dusting till 1 to 2 mm particles without apparent major stone fragments were left tubeless. In borderline cases, a temporary drainage of the treated upper urinary tract using a 5F UC attached to urethral catheter was utilized for 24 hours. In general, patients were discharged at postoperative day (POD) 1 or POD 2, depending on their symptoms and postoperative course.
In our institution, there is a clear postoperative analgesia protocol and it includes diclofenac, pethidine, dipyrone, and tramadol according to pain severity.
The immediate postoperative course was evaluated. Signs and symptoms such as fever, signs of obstructions, and patient discomfort were recorded and evaluated. The pain was assessed three times per hospitalization day using visual analog scale (VAS). The quantity and type of analgesics used were also evaluated.
Statistical analysis was conducted using SPSS software, version 17.0 (SPSS Inc., Chicago, IL). Categorical dependent variables were evaluated using chi-square or Spearman's correlation tests, whereas continuous dependent variables were analyzed using Pearson correlation analysis.
Results
Mean age was 51.33 (10–88 years) years. Stones' characteristics, obstruction severity, preoperative drainage status, and ureteroscope type used are summarized in Table 1. The average stone volume was 344.1 mm3 (11–2847.85 mm3) with mean HU of 976.99 (203–1844). There were 196 (38%) patients who were left tubeless at the end of the surgery, 214 (41%) with a UC for 24 hours, and 106 (21%) patients were left with DJS for 2–4 weeks. In seven cases, bilateral stones management was completed during the same procedure.
Bold indicates the significant p-value.
DJS = Double-J stent; UC = ureteral catheter.
Patients in the tubeless subgroup had significantly smaller stone volume (210 mm3; p < 0.005), with less density (907 HU; p < 0.005) and with significantly less evidence of upper urinary tract obstruction (p < 0.005) compared with the other two groups. It seems that stone location and the type of ureteroscope used affected significantly the decision for postoperative drainage type. Forty percent of cases of kidney stones treatment ended without any type of postoperative drainage, whereas 47% ureteral stones drained by UC (p = 0.001). The tubeless approach was favored when flexible ureteroscope was used, p = 0.003 (Table 1). The decision to drain the upper tracts was not found to be related to simultaneous treatment of both sides or prior drainage of the treated unit with stent or nephrostomy.
The postoperative complications are summarized in Table 2. There was no statistically significant difference between the groups in terms of postoperative fever (>38°C), postoperative renal failure, or symptomatic stone street.
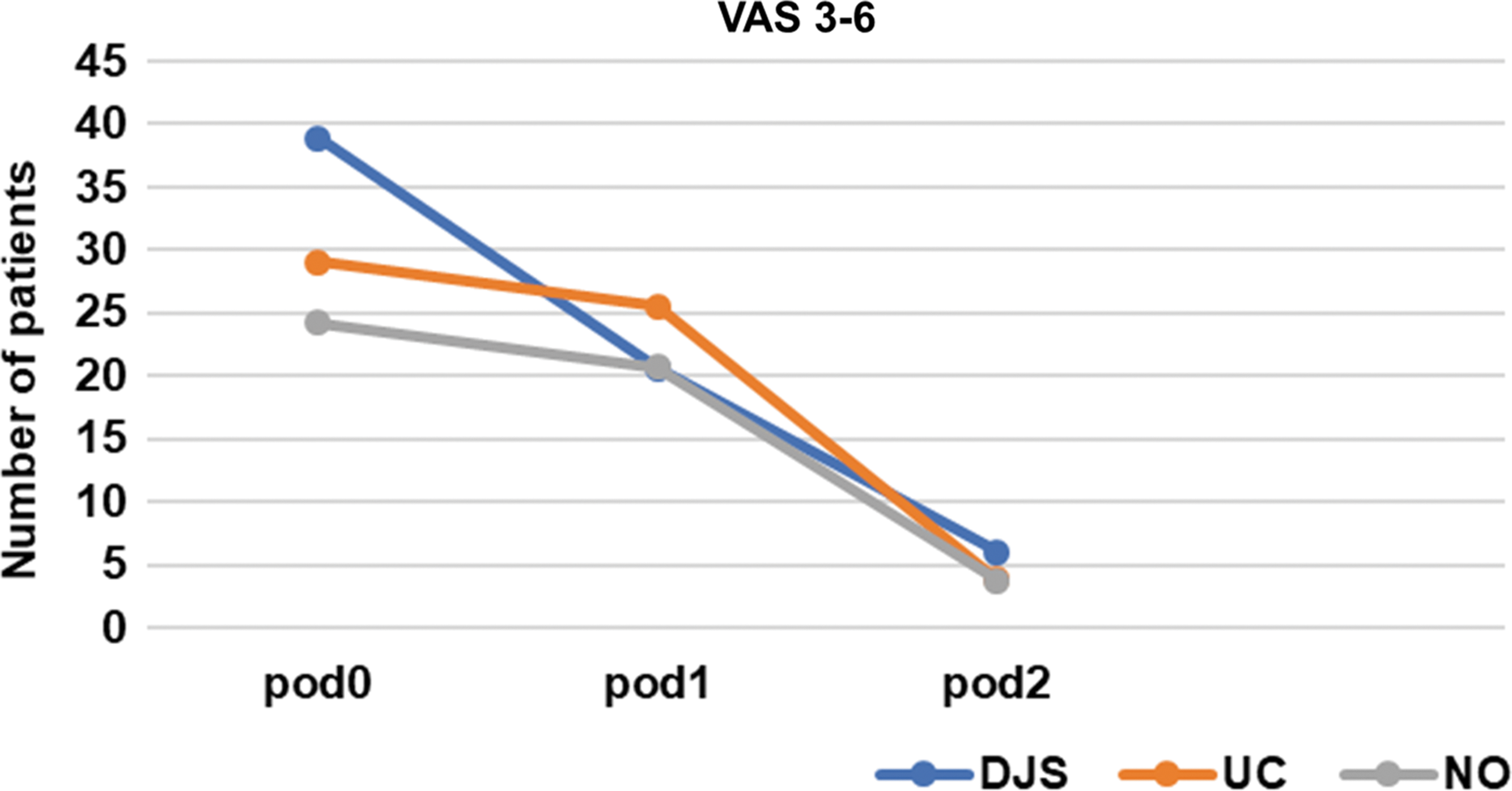
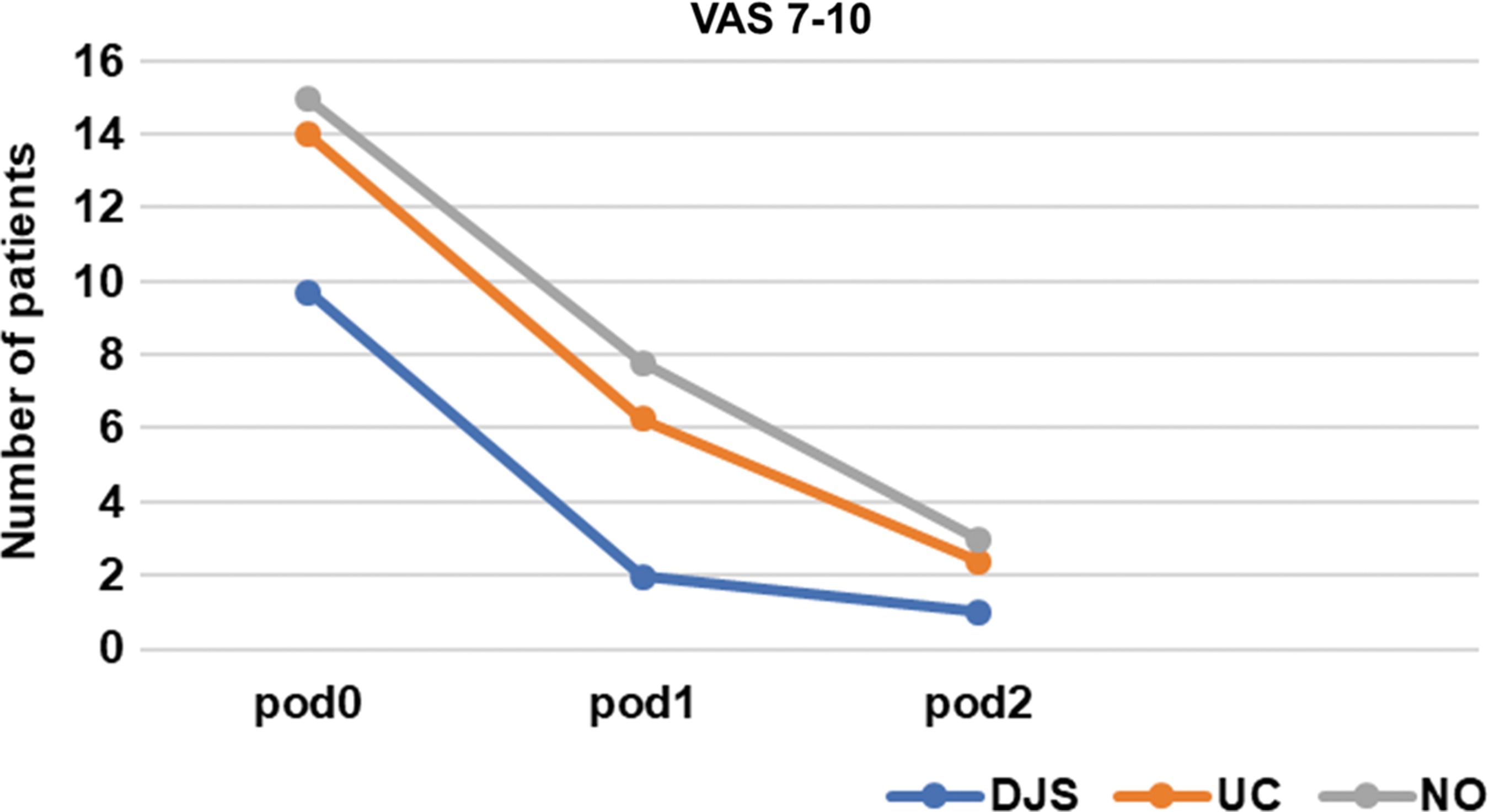
Mean VAS score and need for analgesia are summarized in Table 3. Treatment groups VAS score incremental severity through hospitalization is given in Table 4. Dynamics of VAS change from POD 0 to POD 2 according to VAS severity are shown in Figures 1 and 2. There was no statistically significant difference between the groups, but as given in Table 3 and shown in the Figures 1 and 2, VAS score and analgesics need were decreasing from the day of surgery to POD 2 in all groups.
Mean postoperative VAS = moderate. DJS = Double-J stent; POD = postoperative day; UC = ureteral catheter; VAS = visual analog scale.
Mean postoperative VAS, severe.
POD = postoperative day; VAS = visual analog scale.
To explore the significant factors that influence the VAS score at immediate postoperative phase, we conducted a multivariate analysis of various parameters. This includes patients' age, gender, stone size, location, HU, having a nephrostomy tube or stent before the surgery, type of ureteroscope used, bilateral treatment, hydronephrosis grade, drainage type (none vs UC vs percutaneous nephrolithotomy), and having a urethral catheter after the surgery. It was interesting to see that immediately after the surgery and on POD 1, the only significant factor that influenced the VAS score was patient's age (p < 0.005). Elderly patients did better. However, from POD 2, the only significant factor was the drainage type (p = 0.003).
Discussion
Ureteral stenting after ureterorenoscopy is a common practice among endourologists worldwide. 1 The main reasons for this practice is that stenting is suggested to lead to lower complications rate, prevent postoperative pain because of the expulsion of stone fragments and blood clots, and decrease stricture formation. 10 Pang et al. 11 suggested that after flexible ureterorenoscopy, it is prudent to leave an indwelling ureteral stent for a short period of time to allow any swelling and edema of the ureter to subside. In more complex retrograde intrarenal surgical procedures, stents are used to ensure drainage and to prevent obstruction by blood clots, stone fragments, or swelling that can arise from the manipulations within the urinary tract.
Technological evolution in the past several decades enables flexible ureterorenoscopes with a smaller diameter and lasers machines that enable more efficient stone fragmentation while reducing the potentials of complications. Decreasing instruments size and stent-related symptoms in up to 50% of cases led to the conclusion that there is no need for routine upper tract drainage after uncomplicated procedures with efficient stone dusting. 12,13 Byrne and colleagues 14 described a tubeless approach in endoscopic procedures for treatment of ureteral stones. They concluded that there is no difference in urinary frequency, urgency, or dysuria between the stented and tubeless groups on POD 1, but all these symptoms were significantly reduced in the no-stent group further on. 14 Denstedt and colleagues 6 showed that routine ureteral stenting after ureteroscopy is not mandatory as long as the procedure is uncomplicated and performed without dilatation of the ureteral orifice; the author noted that patients with a stent have significantly more symptoms than those without a stent in the early postoperative period with no difference in complications later on or stone-free status. A recent meta-analysis by Wang et al. 7 combined data from 22 randomized controlled trials and concluded that stenting failed to improve stone-free rate and, instead, resulted in additional complications. However, ureteral stents were valuable in preventing rehospitalization. 7 No significant differences in the VAS score, stricture formation, fever, or hospital stay were found between stented and nonstented groups. Stenting was independent of stone size and location. 7
In our practice, stone volume, density, and previous severe obstruction were significant parameters in the decision to drain the upper tract. We utilize a sheathless dusting technique for stone management. Higher stone volume and higher stone density produce a considerable volume of bigger fragments, and postoperative drainage of the upper urinary tract was necessary. In other cases, according to our data, a stent or a UC may be omitted.
In the presence of significant preoperative obstruction and/or secondary renal function failure, postoperative edema and stone fragments may cause further deterioration, and stenting is mandatory.
It is common to believe that prestenting enables easier retrograde access, decreases intraoperative ureteral damage, and facilitates a better stone fragments expulsion. Surprisingly, in our cohort, the number of prestented cases was not significantly different among tubeless and UC cases. In our practice, we did not use access sheath during ureterorenoscopy. Our flexible and semirigid instruments' outer diameter is small (∼7.5F) and usually we do not perform an orifice dilatation. This might be an explanation that in our series, prestenting had less influence on results.
We did not find any statistically significant difference in postoperative renal failure, infections, or stone street between the groups. This fact demonstrated that tubing may not be necessary in every ureteral and/or renal stone treatment, and the decision should be made on the basis of each individual case.
In agreement with previous studies, 6 –9 we did not find a significant difference in VAS score between our study subgroups. Looking more thoroughly at the data divided to PODs (Table 3), the UC group needed more amount of analgesia and had the highest mean VAS at POD 0 and POD 1. In respect to that, it is needed do stress that the UC group symptoms may be because of Foley urethral catheter that is left as well. At POD 2, the tubeless group needed more analgesia and had higher VAS scores. Surprisingly, the stented group was the least painful through immediate hospitalization period in comparison with others. With ongoing hospitalization, all groups showed decreasing painkiller use and mean VAS severity.
The majority of the patients in all groups had VAS 0–2 (Table 4). Tubeless patients with severe symptoms (VAS 9–10) were more common (9%, 4%, and 3% at PODs 0, 1, and 2, respectively). This can be explained by the possible postoperative edema and fragment expulsion through the “undrained” ureter. In contrast, the UC subgroup did not differ significantly from the tubeless group by means of postoperative pain. Stented patients had mostly minor to moderate symptoms. Figures 1 and 2 show change in symptoms between patients with moderate (3–6) and severe (7–10) range of VAS scores. During the initial postoperative period, stented patients were less symptomatic than tubeless or UC groups. There was no statistically significant difference between UC and tubeless groups in terms of symptoms, in both moderate and severe VAS ranges. At the end of hospitalization, all groups were equal with slight, not significant, tendency for fewer symptoms in the stented group.
It was interesting to see that immediately after the surgery and on POD 1, the only significant factor that influenced the VAS score was patients' age. Elderly patients did better. However, from POD 2, it became insignificant and the only significant factor changed to be the drainage type as discussed. It is important to mention that these procedures are usually being done in most places as an ambulatory procedure. These results give us the opportunity to be aware of patient's symptoms after POD 2, or in other words, after discharging the patient.
There are several limitations to this study, being a retrospective study is the most important. Our database is collected prospectively, but its retrospective analysis enabled us to produce three relevant groups and analyze drainage type effect on postoperative course.
In this study, it is shown that stone burden affected significantly the decision of postoperative drainage type, which then affected the VAS score. As some of the patients were drained postoperatively, it precludes to make a conclusion of a relation between stone burden itself and VAS scores as the groups of comparison depended on tubing placement. It is interesting though to divide tubeless and stented patients to stone volume subgroups in a prospective randomized trial.
Conclusions
There is no consensus on the indications for postoperative ureteral stenting after ureterorenoscopy for ureteral and/or renal stones. Stents may decrease immediate postoperative symptoms. Short-term drainage with UC does not change the postoperative course and, therefore, its use postoperatively is questionable. The tubeless approach is safe and justified in properly selected cases: patients with small stone burden, mild obstruction, and stone with low density. In such cases, there is no difference in postoperative course compared with patients who were drained using UC or DJS. Tubeless procedures enable an outpatient approach to upper urinary tract stones treatment.
Footnotes
Author Disclosure Statement
No competing financial interests exist for all authors of this article.