
Abstract
Introduction:
The most commonly performed procedure among urologists is cystoscopy. However, urologists in developing countries have limited access and funds to purchase the equipment necessary to perform this procedure. The novel Endockscope (ES) mobile endoscopic system aids in reducing this gap in both cost and accessibility.
Materials and Methods:
ES kits were distributed at the 2016 World Congress of Endourology in Cape Town, South Africa. All participants were given instructions on how to use the device and each participant attended a live demonstration during the conference. Eight months later, all participants were contacted via email, regular mail, or phone to complete a questionnaire designed to assess the impact of the ES device.
Results:
A total of 24 ES kits were distributed. After numerous emails, questionnaires sent by regular return mail, and phone calls, 12 (50%) participants completed the survey as instructed. Seventy percent of participants reported that they performed more endoscopic procedures due to the ES system. Overall, 90% of participants stated that they would purchase the ES system for personal use ($40.53). All participants reported that they would recommend the ES to others.
Conclusion:
The ES system provided an effective inexpensive system to enable urologists in resource-challenged countries to offer cystoscopy to more of their patients.
Introduction
C
The rapid development of new and improved technologies (e.g., flexible cystoscopy and digital endoscopes) has allowed for a more accurate diagnosis and overall comfort for the patient undergoing diagnostic cystoscopy. However, the impact of these advances is limited by their cost; a complete standard high-definition endoscopic system has a purchase price of ∼$46,000, 2 well outside the realm of many impoverished countries.
The introduction of the Endockscope (ES), an affordable mobile videocystoscopy system that utilizes a mobile phone for image display and a rechargeable light-emitting diode self-contained cordless light source, may possibly provide global access to videocystoscopy (Figs. 1 and 2). 2 Previous studies comparing the quality of the ES with conventional cystoscopy systems revealed that the ES produces similar outcomes and comparable diagnostic capabilities. 3 At the 2016 World Congress of Endourology (WCE) in Cape Town, South Africa, we distributed this novel device to urologists from developing countries and then, 8 months later, conducted a survey to determine user assessment of the ES system in a clinical practice.

ES system showing a smartphone along with the rechargeable light source (foreground) and the smartphone attachment lens (on the right). ES = Endockscope.

ES system attached to flexible fiber optic cystoscope.
Materials and Methods
The ES system was designed and produced through a collaborative effort between the Department of Urology and the Department of Engineering at the University of California, Irvine. The system we developed utilizes a smartphone for image display and a rechargeable, wireless light source. 2,3
ES kit
Each ES kit was secured in a small and lightweight (9.5′′ × 6.5′′ × 2.2′′, 4.8 oz.) carrying case to allow for easy storage and transportation. Each case consisted of an 8 × optical zoom lens with a custom coupling mechanism for attachment to an endoscope's eyepiece, light source with custom coupling mechanism for attachment to an endoscope's light port, battery, and battery charger (Figs. 1 and 2). Each kit also included a variety of compatible Apple iPhone smartphone cases that were available at the time of distribution (iPhone 4/4s, 5/5c/5s, 6/6s, 6+/6s+) (Apple, Cupertino, CA). The ES system was assembled using both commercially available and custom three-dimensional (3D)-printed components. 2,3 We used SolidWorks software (Dassault Systemes SolidWorks Corp., Waltham, MA) and an uPrint SE Plus 3D printer (Stratasys Ltd., Rehovot, Israel) to design and print the custom coupling mechanisms. The cost of each kit was ∼$40.53 (Table 1).
3D = three dimensional.
World Congress of Endourology 2016
ES kits were taken to the 2016 WCE in Cape Town, South Africa, supported by a grant from the Endourological Society. During the meeting, we distributed the ES kits to 24 urologists, free of charge. All participants were given instructions and a hands-on live demonstration of the device. Subsequently, all participants were asked to complete and submit a questionnaire 8 months after the congress to determine the impact of the ES device (Appendix A1). The questionnaire evaluated user satisfaction, comfort, similarity with standard endoscopic systems, and procedure type. In addition, participants were asked whether they were able to perform more endoscopic procedures, and whether they used any of the other smartphone features. Participants were also asked if they would purchase the ES system for personal clinical use ($40.53) and if they would recommend the ES to others.
Results
The ES kits were distributed to 24 participants from the following countries: Philippines, South Africa, Chile, Kenya, Burkina Faso, Chad, Nigeria, Uganda, Zimbabwe, Slovenia, Sudan, and Mauritius. All participants stated that they had access to a fiber optic cystoscope.
Of the 24 participants, after numerous emails, regular mail return letters, and phone calls, 12 urologists returned a completed questionnaire. The 12 respondents were from Zimbabwe, Nigeria, South Africa, Sudan, Slovenia, and Chile.
Of the 12 respondents, 83% (10) reported having used the ES in their clinical practice (Fig. 3). The two respondents who did not use the ES reported that it was due to a lack of flexible cystoscopes for in-office cystoscopy in their countries, Slovenia and Zimbabwe. Of the group that used the ES, 80% used it only for cystoscopy, while 20% used it for both flexible cystoscopy and flexible ureteroscopy (Fig. 3). Ninety percent reported that the device was satisfactory for use, 80% found the device comfortable to use, and 80% reported that the ES was similar to a standard endoscopic setup (Table 2). In addition, 70% reported that they were able to perform more endoscopic procedures than normal because of the ES and were able to use smartphone features to share images and video to assist with making a diagnosis. Overall, 90% of participants reported that they would purchase the ES system for personal use and all of the respondents noted they would recommend the ES to other urologists.
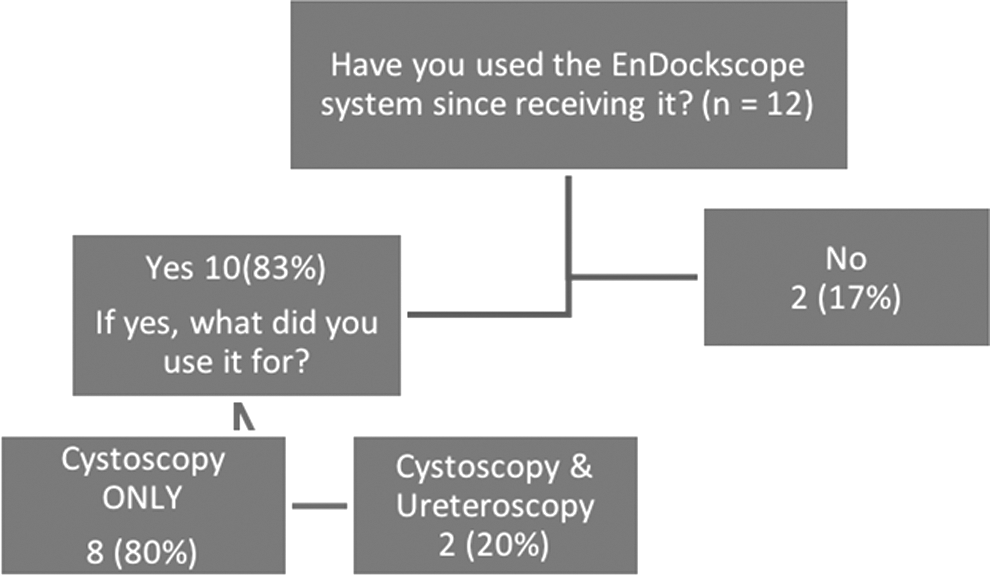
Global ES Survey responses.
Discussion
Cystoscopy is the most common procedure performed by urologists. 1 While cystoscopy is well documented and is an invaluable tool for diagnosing lower urinary tract pathology, it has been limited in developing countries by a lack of supplies and other resources. Cystoscopy currently requires the use of a large endoscopic tower system, which includes a tower, monitor, light box, video box, camera, and cables. While these are readily available in many countries, the cost, as much as $46,000, prohibits their use in many developing countries. 2
The ES seeks to replace the usual $46,000 setup, with a $40.53 array of devices that turn a smartphone into a video camera/recorder. The ES acts as a docking system that optimizes the coupling of a smartphone to the eyepiece of existing endoscopes. In this system, the smartphone can be utilized as the monitor, camera, and video box to create an endoscopic viewing platform. This, in addition to the included wireless and rechargeable light source, provides a low-cost solution. The entire system fits into a small case (9.5′′ × 6.5′′ × 2.2′′, 4.8 oz.) that can be easily stored or transported.
Among the participants, who reported using the ES, all were able to use it effectively to perform cystoscopy, ureteroscopy, or both. The majority of participants found the device to be satisfactory for use as well as comfortable, and similar to their hospital's endoscopic setup. Of note, 70% reported that they were able to perform more endoscopic procedures than usual because the ES was available for them to use both in the hospital and in any office setting.
Continued advances in mobile technology and the global widespread use of smartphones have allowed the incorporation of mobile technology into different facets of medicine. 4 –7 Worldwide, there are over 1 billion smartphones in use and this number is expected to double in coming years. 8 In this study, 70% of participants reported that they were able to use smartphone features to record and transmit images and videos to help with diagnosis. As smartphone technology continues to advance, we can incorporate features for medical use such as an app for pathology recognition during or after the procedure as well as sharing of videos with experts at a remote center.
This study has several limitations. Due to costs of distributing the ES free, we had a relatively small sample size. Despite vetting each recipient and assurances that they had a flexible fiberoptic cystoscope available to them, it was disappointing that half of the urologists who accepted an ES failed to respond to numerous requests to complete the questionnaire and, indeed, two could not readily access a flexible fiberoptic cystoscope. Of note, as the participants were informed, the ES kits were only compatible with Apple iPhone models available at the time of the study; it is possible that some of the participants did not clearly understand this limitation. Over the past year, the ES has been further developed such that it is now also compatible with a wide variety of Android devices.
Conclusions
Smartphone use continues to rapidly spread across the globe regardless of a country's economy. Exploiting the smartphone as a medical device with the ES, in this pilot study, provided an opportunity for urologists in a challenging environment to perform flexible fiber optic cystoscopy as well as ureteroscopy in an effective, low-cost manner.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Abbreviations Used
Appendix A1. Questionnaire
1. Which iPhone model did you use the Endockscope kit with?
2. Have you used the Endockscope system since receiving it?
3. If yes for what did you use it for?
4. Have you been able to perform MORE endoscopic procedures than normal because of the Endockscope?
5. How many times over the last 3 months have you used the Endockscope kit?
6. Are you still using your Endockscope kit?
7. If you answered “no,” please explain why you are no longer using the Endockscope.
8. Have you used any smartphone features to transmit any of your images/videos to help with diagnosis?
9. Have you experienced any problems using the Endockscope system?
10. If you answered “Yes” to the question above, please comment below.
11. Was the Endockscope system satisfactory for use?
12. Was the Endockscope image similar to your standard endoscopic setup?
13. Was the Endockscope system comfortable to use?
14. Would you purchase the Endockscope system for personal use (∼$40)?
15. Would you recommend the Endockscope system to others?
16. Comments/Suggestions.