
Abstract
Introduction:
Nephron-sparing surgery has emerged as the treatment of choice for small renal masses. However, its role in larger tumors remains controversial. In this study, we compare the outcomes of laparoscopic partial nephrectomy (LPN) vs those of laparoscopic radical nephrectomy (LRN) for T2 renal tumors.
Materials and Methods:
Thirteen patients who had LPN and 16 patients who had LRN for T2 renal tumors were retrospectively analyzed for preoperative factors (age, gender, comorbidities, hemoglobin, and creatinine levels and estimated glomerular filtration rate [eGFR]), operative and perioperative characteristics (tumor characteristics, operative time [OT], warm ischemia time [WIT], estimated blood loss [EBL], length of stay [LOS], and postoperative complications), histopathologic results, and follow-up data (eGFR and recurrences).
Results:
Tumor size was comparable between groups; however, tumors in the LRN group were more endophytic, central, and closer to the collecting system. There were no cases of positive surgical margins. Median OT was 160 minutes vs 230 minutes (p = 0.0029) and EBL was 25 mL vs 100 mL ([p = 0.0027], LRN vs LPN). Median WIT in the LPN group was 27 minutes, with three zero ischemias. Minor postoperative complications (≤Clavien–Dindo III) were noted in 6.25% and 23% (LRN vs LPN). Median LOS was 4.56 and 5.77 days (LRN vs LPN), respectively. Mean postsurgery eGFR was significantly lower for the LRN group (54.5 cc/[min ·1.73 m2] vs 76.3 cc/[min ·1.73 m2], p = 0.019). Within mean follow-up of 44.5 months, one tumor recurrence in the contra lateral kidney was observed in the LPN group and two cases of metastasis in the LRN group.
Conclusions:
We show that LPN is technically feasible for T2 tumors, with acceptable intra- and perioperative outcomes. Furthermore, our results show a significant advantage in preservation of renal function for LPN without compromising oncologic results. Taken together, we believe that LPN should be considered for larger tumors based on technical feasibility rather than only tumor size.
Introduction
H
Materials and Methods
Data collection
We reviewed our institutional database retrospectively to identify patients who underwent LPN or LRN for clinical T2 (≥7 cm) renal masses from 2012 to 2017. Patient demographics and preoperative data collected included age, gender, comorbidities, smoking status, baseline hemoglobin level, baseline serum creatinine levels, and estimated glomerular filtration rate (eGFR) calculated according to the four-variable modification of diet in renal disease equation. Tumor characteristics were determined based on preoperative imaging (CT or MRI) and graded according to the R.E.N.A.L. nephrometry score (size, centrality, and location). 16 Perioperative variables collected included operative time (OT), warm ischemia time (WIT), estimated blood loss (EBL), LOS, and postoperative complications classified according the Clavien–Dindo classification system. 17 Pathologic variables collected included tumor size, histologic subtype, Fuhrman grade, and surgical margins status. Follow-up data collected included eGFR 6 months postsurgery, follow-up period, recurrences, and mortality rate.
Surgical technique
We use the standard transperitoneal approach with three to four trocars as previously described. 18 When performing LPN, after dissecting the renal hilum and identifying the tumor, the tumor resection margins are marked with cautery. Typically, a bulldog clamp is applied to the renal artery and vein en bloc, unless a nonclamping approach is feasible. The mass is excised and trapped in a bag. The defect is then closed in two layers: a running suture secured on both ends with a clip controls the resection bed, and for the superficial layer, a running suture is interrupted by clips. In addition, synthetic surgical glue is used on the crater.
Statistics
Data were analyzed using Graphpad Prism version 7 (GraphPad Software, Inc., CA). Student's t tests and Pearson's chi-squared tests were used for statistical hypothesis testing for normally distributed and categorical data, respectively. Statistical significance was set at p < 0.05.
Results
Between 2012 and 2017, a total of 32 patients in our institution underwent laparoscopic surgery for T2 renal masses. Thirteen patients had LPN and 16 had LRN. Demographic and preoperative parameters of the two groups are summarized in Table 1. No statistically significant differences could be detected for mean age, gender, comorbidities, smoking status, and mean serum creatinine and hemoglobin levels. The mean age of both groups was 64.5 years with male predominance (82.7%). The radiographic tumor parameters were graded according to the R.E.N.A.L. nephrometry score (Fig. 1). Tumor radius was >7 cm for all tumors in both groups. Overall, tumors in the LRN group were more endophytic (2.25 points vs 1.67 points, p = 0.007), closer to the collecting system (2.75 vs 1.92, p = 0.0067), and more central (2.56 vs 1.31, p = 0.0001). Posterior lesions accounted for 50% of cases in the LRN group and 46.15% of cases in the LPN group. Pathologic tumor size was 8.3 cm in the LRN group and 7.7 cm in the LPN group, with no significant difference between groups (p = 0.134; Fig. 2). The majority of masses were of clear cell subtype (87.5% in the LRN group and 46% in the LPN group) with Fuhrman grade 2 in 37% and 53% and Fuhrman grade 3 in 56% and 38% of patients in the LRN vs LPN groups, respectively. There were no positive surgical margins in either group. In two patients in the LRN group (12.5%), the final T stage was T3a. All cases were managed laparoscopically with no conversions to an open technique. Median OT was 160 (IQR 100–250) minutes vs 230 (IQR 180–270) minutes in the LRN and LPN groups, respectively (p = 0.0029, Fig. 3). Median WIT in the LPN group was 27 minutes, with three cases managed with zero ischemia. EBL was 25 mL in the LRN group vs 100 mL in the LPN group (p = 0.0027). Minor complications (≤Clavien–Dindo III) were noted in 6.25% and 23% (LRN vs LPN), respectively. Median LOS was 4.56 days vs 5.77 days for the LRN and LPN groups, respectively (p = 0.13). Mean eGFR before surgery for both groups was 83 cc/(min ·1.73 m2). Mean postsurgery eGFR was 54.5 and 76.3 cc/(min ·1.73 m2) for LRN and LPN groups, respectively (p = 0.019). Accordingly, ΔeGFR was −28 and −7.6 for LRN and LPN groups, respectively (p = 0.003, Fig. 4). Mean follow-up time was 44.5 months for both groups. During this period, in the LPN group, there was one tumor recurrence in the contralateral kidney that required RN. In the LRN group, two patients were found to have metastases of renal cell carcinoma (RCC) during follow-up: one to the lung 6 months after surgery and one to the pancreas 2 years after surgery.
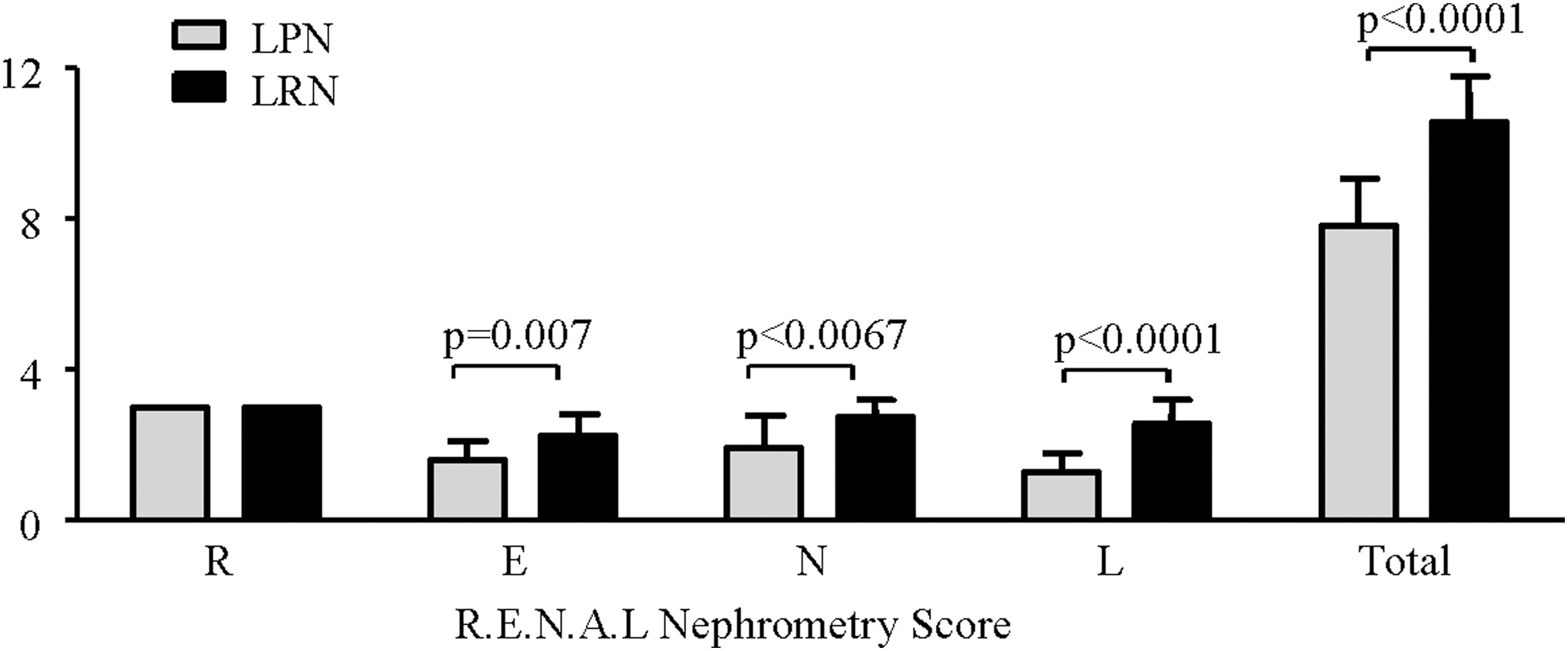
Comparison of radiographic tumor parameters between the LPN group (gray columns) and the LRN group (black columns). Radiographic parameters are based on preoperative imaging (CT or MRI) and graded according to the R.E.N.A.L. nephrometry score (radius, exophytic/endophytic, nearness of the tumor to the collecting system or sinus, anterior/posterior, location relative to the polar lines). LPN = laparoscopic partial nephrectomy; LRN = laparoscopic radical nephrectomy.
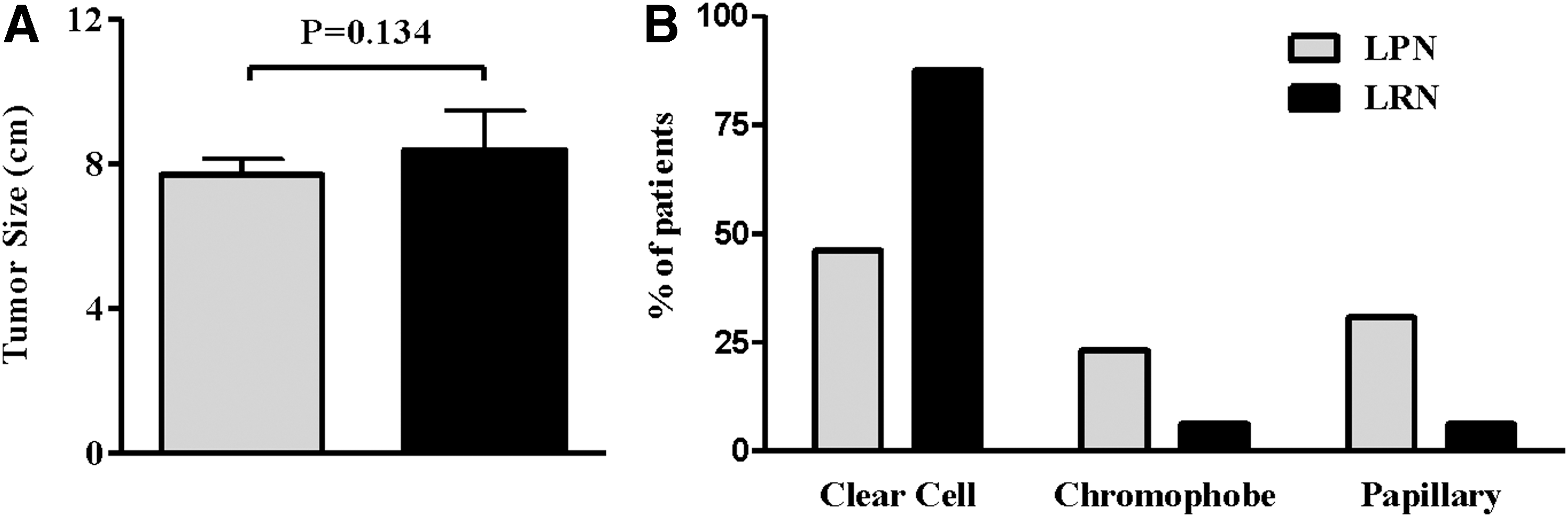
Comparison of pathologic variables collected from specimens, between the LPN group (gray columns) and the LRN group (black columns).
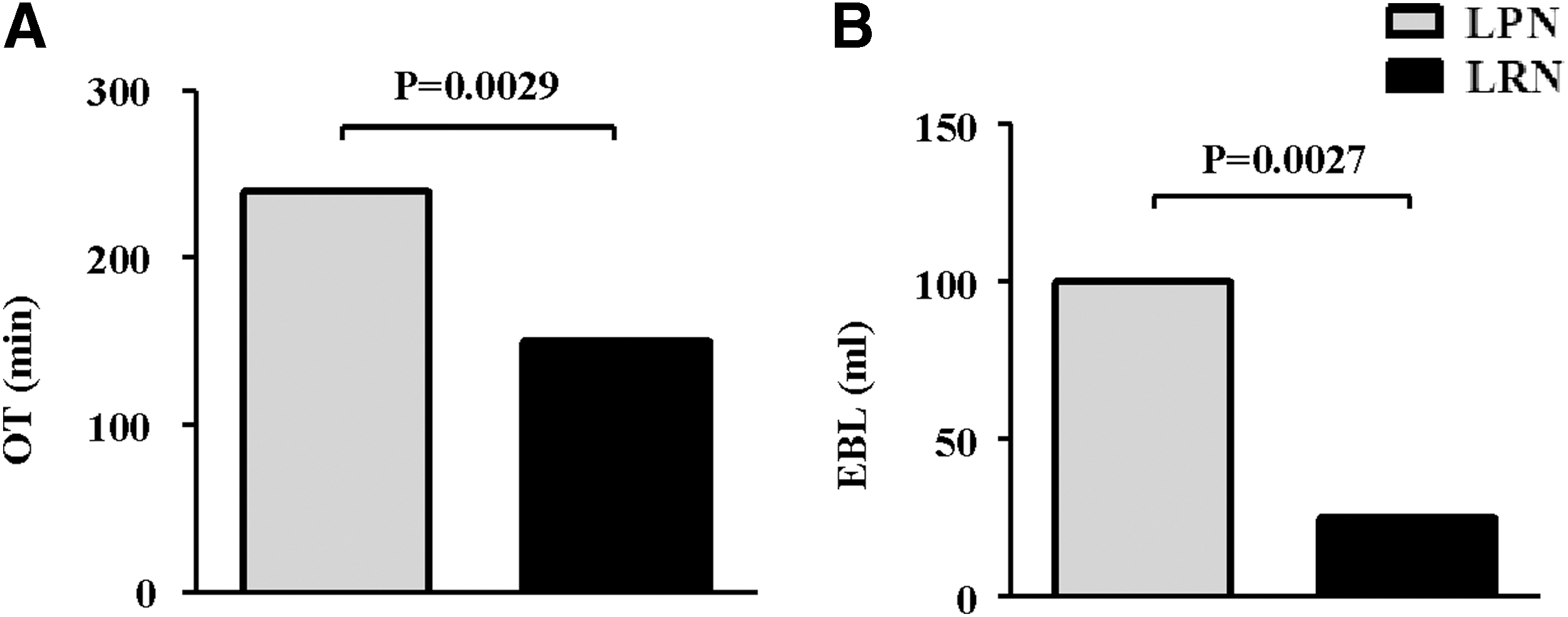
Comparison of intraoperative variables between the LPN group (gray columns) and the LRN group (black columns).
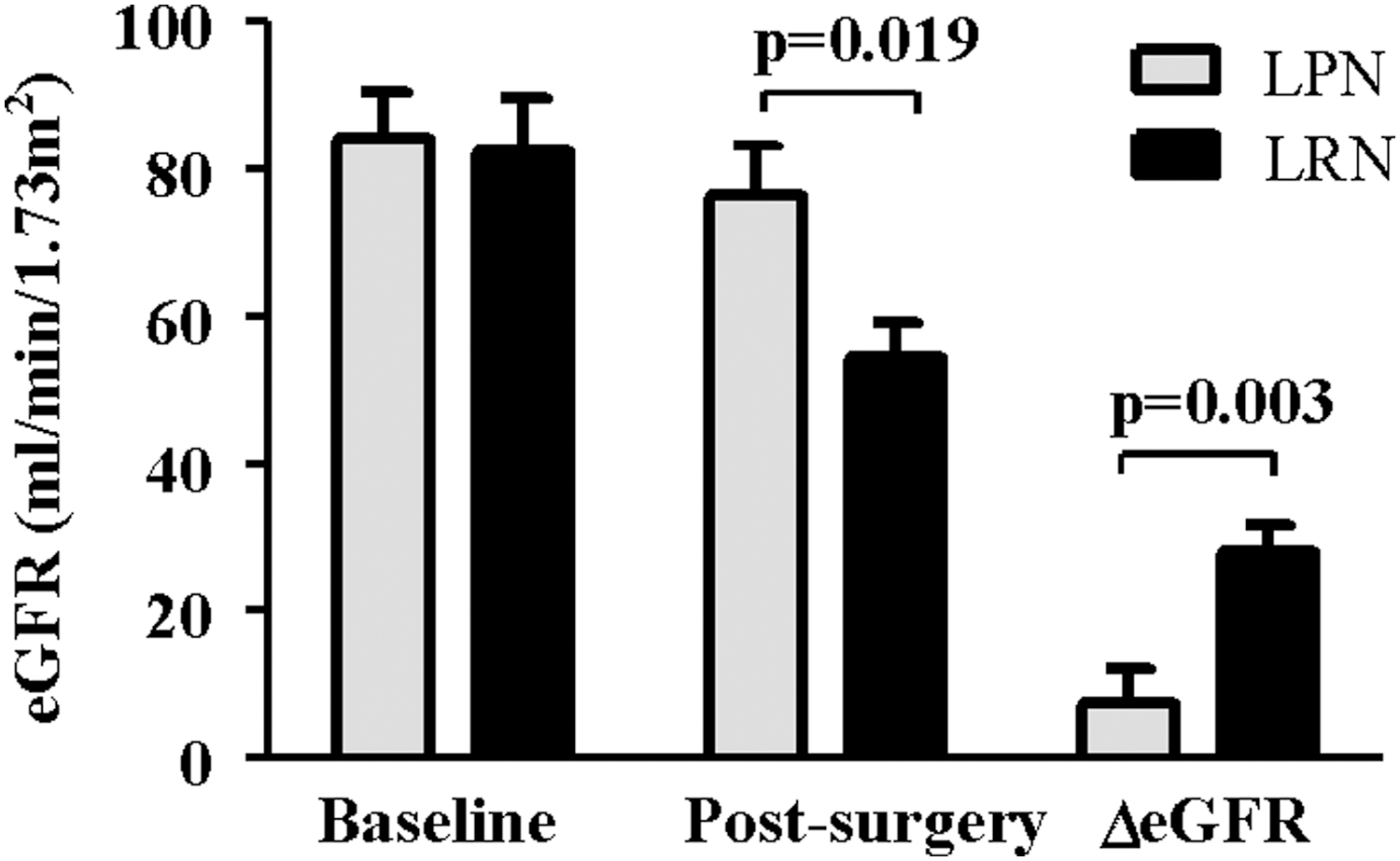
Comparison of renal function pre and postsurgery between the LPN group (gray columns) and the LRN group (black columns). Renal function was measured using the eGFR at baseline and 6 months postsurgery. eGFR was calculated according to the four variable modifications of diet in renal disease equation. eGFR = estimated glomerular filtration rate.
t Test.
Chi-square test.
LPN = laparoscopic partial nephrectomy; LRN = laparoscopic radical nephrectomy.
Discussion
The basic principles of NSS for RCC are complete excision of the lesion with negative margins, while preserving as many viable renal parenchyma as possible. Sparing nephrons will eventually result in long-term preserved renal function and, consequently, improved metabolic and cardiovascular function. In our opinion, PN should be considered even for larger tumors whenever technically feasible. Laparoscopy as the surgical technique for PN still remains the mainstay of minimally invasive surgery in many parts of the world and, therefore, its applicability for T2 tumors is relevant and important. Generalization of our data to other minimally invasive surgical techniques (e.g., robotic or nontransperitoneal laparoscopic approaches) could be made with caution depending on the institutional experience in each approach. We see an advantage in the description of one pure surgical technique in our series, since it enables to focus on the comparison between RN vs PN for T2 renal masses without the confounding factor of the surgical approach. Our results show a statistically significant advantage in the preservation of renal function for LPN without compromising oncologic results. Since our study is based on retrospective data, a somewhat inherent bias in patient selection for PN vs RN can be observed. Analysis of preoperative tumor parameters shows that although the tumor radius in both groups was >7 cm, tumors in the LRN group were more central, more endophytic, and closer to the collecting system. This might suggest that indications for PN should depend primarily on technical feasibility rather than only on tumor size. As expected, OT was in favor of LRN. However, OT time in the LPN group is in line with our 19 and others' 20 series of LPN for smaller renal masses and, therefore, reasonable also for larger tumors. Median WIT in the LPN group (27 minutes) was slightly longer than the WIT reported and measured in our experience with LPN of smaller masses 19 ; however, it is still under the 30-minute safety limit for minimizing renal ischemic damage. 21 Moreover, three patients who had LPN using the nonclamping technique showed its feasibility for T2 tumors in select cases. EBL was in favor of LRN; however, blood loss in the LPN was of no clinical significance. Taken together, intraoperative differences did not affect the need for blood transfusions nor LOS. Our results show no oncologic disadvantage for LPN. There were no cases of positive margins, and during a follow-up period of 44.5 months, there were no local recurrences or distant metastasis in the LPN group. It should also be taken into consideration that the incidence rate of a metachronous contralateral tumor varies from 2% to 6% after RN and remains constant for >10 years after surgery. 21 Indeed, in our study, one patient in the LPN group was found to have a metachronous contralateral tumor during the follow-up period, which emphasizes the importance of PN in these patients.
Our present study has several limitations. It is a small retrospective single-center study with a limited follow-up period. We acknowledge the fact that drawing meaningful comparison is difficult in such a small cohort; however, we did reach significant differences both in the preoperative tumor parameters (e.g., nephrometry score): the perioperative variables (e.g., OT and EBL) and the follow-up data (e.g., mean postsurgery GFR and ΔGFR). It should also be taken into consideration that since PN for larger tumors is not yet the common practice and is not always feasible, it results in relatively small series as seen in our study and the literature. We believe that our data could add up to the current available literature and contribute to the minimally invasive kidney cancer literature. We do plan to continue follow-up in order for our oncologic outcomes to mature.
Conclusions
To the best of our knowledge, this is the first report that compares the outcomes of pure LPN with those of LRN for T2 renal masses. In our study, LPN for larger renal masses appears feasible with acceptable intra- and perioperative outcomes and with significant advantage in preservation of renal function, without compromising oncologic results. One must keep in mind that the approach suggested here may be challenging and may be suggested for centers with high volume of laparoscopic renal surgery. Additional data, especially prospective studies, are needed to further explore the benefits of minimally invasive surgical approaches to larger renal masses.
Footnotes
Author Disclosure Statement
No competing financial interests exist.