
Abstract
Background and Purpose:
Although balloon dilatation is one of the main endoscopic procedures used to treat benign ureteral strictures, its precise efficacy remains controversial. We aimed to identify, combine, and analyze existing published data to ascertain the efficacy of endoscopic balloon dilatation for benign ureteral strictures.
Methods:
In December 2018, a literature search was performed using Medline, Embase, and Web of Science databases. We included reports in which the study population consisted of patients who underwent endoscopic balloon dilatation for the treatment of benign ureteral strictures. Technical, short-term, and long-term success rates (expressed as mean ± standard error) were adopted as the outcome measures.
Results:
Using our search strategy, a total of 19 studies (all series reports) were included for analysis. Using a random-effects model, the pooled technical success rate of endoscopic balloon dilatation for benign ureteral strictures was found to be 89% ± 4%. Furthermore, the short-term success rate (i.e., 3 months after surgery) was 60% ± 10%, and the long-term success rate (i.e., 6–12 months after surgery) was 54% ± 14%. In the subgroup analysis, the success rate of endoscopic balloon dilatation for ≤2-cm benign ureteral strictures was significantly higher than that for >2-cm ones (odds ratio [OR]: 0.13; 95% confidence interval [CI]: 0.05–0.35). In addition, the success rate in cases with strictures of onset timing ≤3 months was relatively higher than that in cases with strictures of onset timing >3 months (OR: 0.46; 95% CI: 0.15–1.43).
Conclusion:
Our study indicates that endoscopic balloon dilatation has a high success rate in the treatment of benign ureteral strictures with length ≤2 cm and onset timing ≤3 months. However, there is still no consensus on balloon type, dilatation pressure, expansion number, postoperative ureteral stent type, and stent retention time for the balloon dilatation technique.
Introduction
Ureteral stricture refers to urinary tract obstruction caused by partial or complete narrowing of the ureteral lumen. This inevitably leads to expansion of the upstream urinary tract and renal area pain and, eventually, irreversible renal failure without timely treatment. Ureteral strictures can be caused by a variety of factors mainly classified as benign or malignant. Benign causes include congenital factors and secondary causes such as surgical injury, stones, infection, trauma, radiotherapy, renal transplantation, urinary diversion, and idiopathic cases, while malignant ureteral strictures can develop due to primary ureteral malignancy or adjacent tumor extrinsic compression. 1 The incidence of ureteral stricture varies by causes and can be seen during impacted stone surgery (7.8%–26.2%), ureterointestinal anastomoses (1.4%–15%), and renal transplantation (3%–8%). 2 –6
The goals of ureteral stricture management are to relieve ureteral obstruction and preserve renal function. Traditionally, benign ureteral strictures have been managed using various open surgical techniques, including ureteral anastomosis, ureteral bladder anastomosis, and bladder ureteroplasty (Boari-plasty). 7 Although open surgery is a definitive approach that can save renal function, it is also associated with significant complications, long hospital stays, and high medical expenses. 8,9 Laparoscopic repair of benign ureteral strictures is also effective and feasible. 1 Although the laparoscopic approach is superior for blood loss and hospitalization, studies have shown similar complication rates and even longer operation times compared with open surgery. 10,11
More recently, the development of endoscopic techniques has provided an alternative to open surgery, with urologists increasingly choosing to treat ureteral strictures under endoscopy. This provides a cost-effective and minimally invasive approach for the management of specific ureteral strictures. 12 –14 Common endoscopic techniques include balloon dilatation, ureteral stent implantation, and stricture incision with a laser or cold knife. Among these, balloon dilatation was first introduced for ureteral strictures in 1926 by Dourmashkin. 15 In the early 1980s, the introduction of angiographic dilation balloons made it an accepted treatment mode for ureteral strictures. As balloon dilatation is easy to perform and has a short learning curve with fewer complications and low cost, it can be considered the most suitable initial treatment for ureteral stricture. 16 Even if balloon dilatation fails, it does not affect the subsequent open surgery. However, despite being commonly used, the exact efficacy of balloon dilatation remains controversial. We therefore aimed to evaluate the therapeutic effect of endoscopic balloon dilatation in the treatment of benign ureteral strictures by performing a systematic review and meta-analysis of the reported literature.
Methods
Literature search
Our search strategy is summarized in Figure 1. A computer literature search was performed using the PubMed, Embase, and Web of Science databases with the key words “ureteral stricture” OR “ureteral stenosis” OR “ureteral obstruction” AND “balloon dilatation” OR “balloon dilation” on December 2, 2018. The search was limited to studies that were reported in English and conducted with human populations. Simultaneously, reference lists of included articles and relevant review articles were manually searched to obtain the most comprehensive literature for analysis. The retrieved articles were independently viewed by C.L. and W.Z.
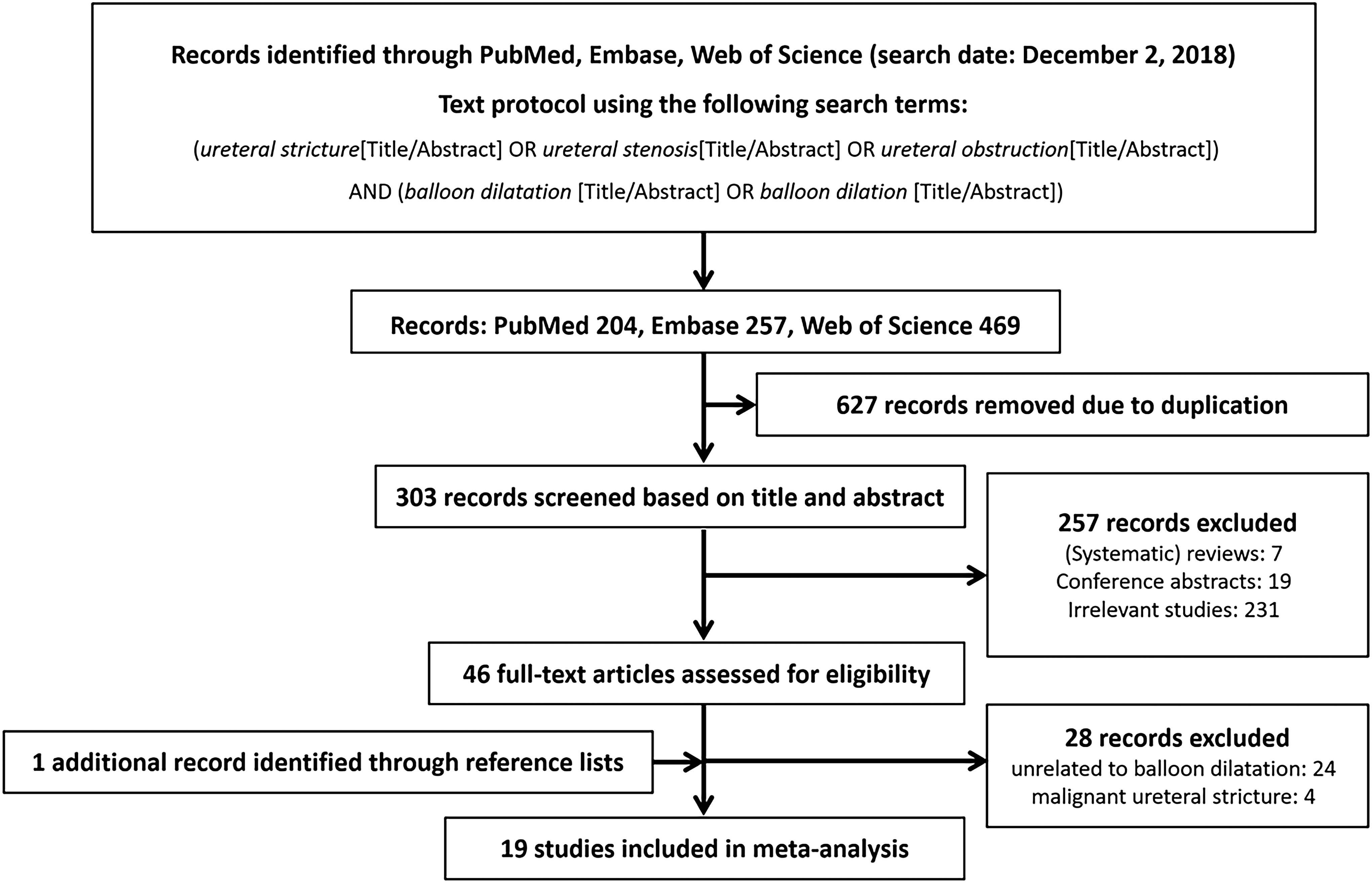
Flow diagram of the literature search strategy.
Inclusion and exclusion criteria
Studies were included in our analysis if they met the following criteria: (i) controlled trial or series report with >10 cases, (ii) included patients of any gender or age with benign ureteral strictures confirmed by imaging and ureteroscopy, (iii) endoscopic balloon dilatation was performed with or without a postoperative indwelling ureteral stent, and (iv) postoperative evaluation included determination of technical, short-term, and long-term success rates. The exclusion criteria were (i) case reports and controlled trials or series reports with 10 or fewer cases, (ii) included patients with malignant ureteral strictures, and (iii) nonballoon dilatation endoscopic management was performed.
Statistical analyses
Meta-analysis was performed using Stata, v12.0, software (StataCorp, College Station, TX). First, heterogeneity between studies was assessed using the Q statistic. If there was no significant heterogeneity (p ≥ 0.1, I 2 ≤ 50%), the fixed-effects model was used for pooled analysis. If heterogeneity existed (p < 0.1, I 2 > 50%), we first tried to identify the source of heterogeneity and conducted subgroup pooled analysis. If heterogeneity could not be eliminated, the random-effects model was used for pooled analysis. The combined outcome measures were technical, short-term, and long-term success rates of surgery, with rates reported as mean ± standard error. Since the majority of surgical failures and stricture recurrences occur within 1 year of endoscopic management, 17 we defined short- and long-term success rates as those at 3 and 6–12 months, respectively. Subgroup analyses were performed to evaluate the influence of stricture length (≤2 cm vs >2 cm) and stricture onset timing (≤3 months vs >3 months) on the success rate using the pooled odds ratio (OR) and confidence interval (CI) as risk estimates.
Results
Study characteristics
A total of 19 studies were finally included. 7 –9,18 –33 A total of 683 subjects with follow-up periods from 3 months to 5 years were included (Table 1). The methodological index for nonrandomized studies (MINORS) was estimated for all included studies, 34 which showed relatively high or medium quality (MINORS score: 9–12 of 16 points). The baseline characteristics of patients were sufficiently presented and endpoints were appropriate for the study aims. Common quality defects were attributed to lack of prospective calculation of study size and no blinded evaluation of endpoints. As the pathogenic categories of ureteral strictures and definition of success were not coincident among the included studies, we have illustrated the detailed etiology in Supplementary Table S1 and each definition in Supplementary Table S2.
Characteristics of Studies Included in the Meta-Analysis
Follow-up period expressed as mean (range) where applicable.
NA = not applicable; MINORS = methodological index for nonrandomized studies.
Meta-analysis results
Technical success rate
Fourteen studies reported the technical success rate of balloon dilatation management, of which 10 were published before 2000. Technical success meant delivery and subsequent expansion of the balloon past the ureteral stricture, followed by placement of an indwelling ureteral stent. Meta-analysis using a random-effects model showed a technical success rate of 89% ± 4% (Fig. 2).
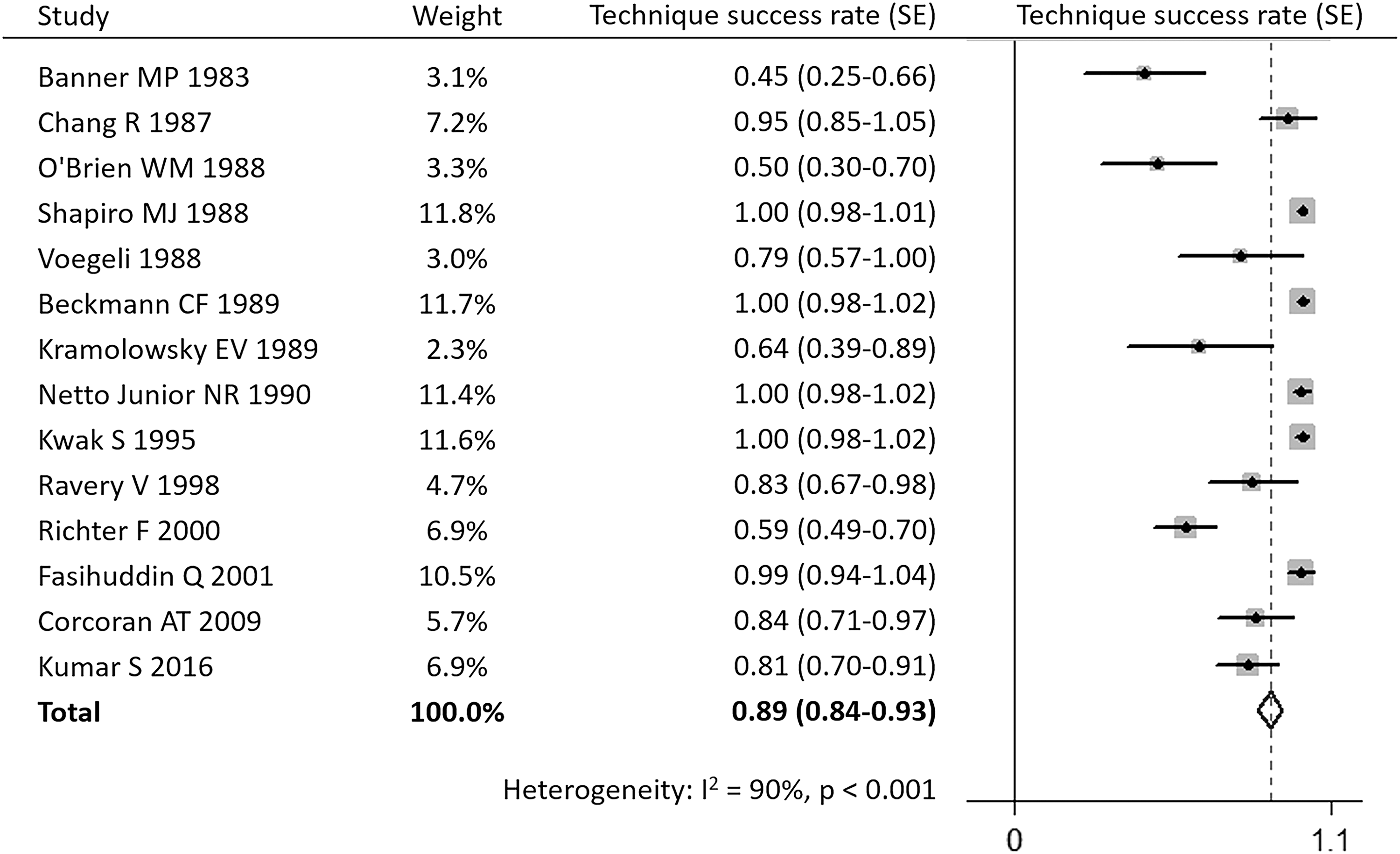
Forest chart for the technical success rate.
Short-term success rate
Five studies (all published before 2000) reported the success rates of balloon dilatation management after a mean follow-up period of about 3 months. The criteria used to identify ureteral patency after surgery in these studies were the disappearance of clinical symptoms such as backache and nausea, improved hydronephrosis by imaging, and improved renal function indexes such as the glomerular filtration rate. Meta-analysis using a random-effects model showed a short-term success rate of 60% ± 10% (Fig. 3).
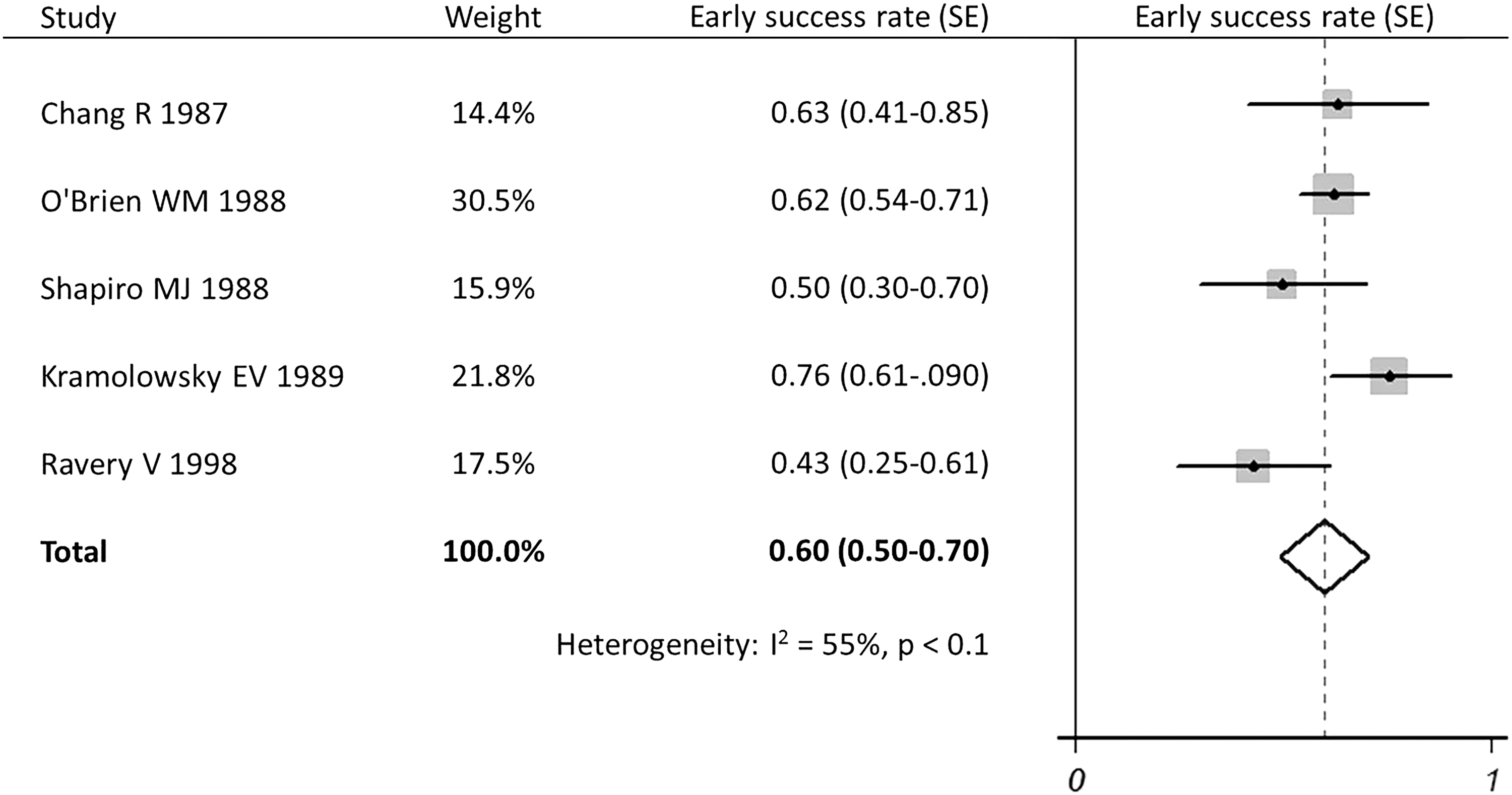
Forest chart for the short-term success rate.
Long-term success rate
Twelve studies reported the success rate of balloon dilatation management after a mean follow-up period of 6–12 months. Of these studies, six were published before 2000. Meta-analysis using a random-effects model showed a long-term success rate of 54% ± 14% (Fig. 4).
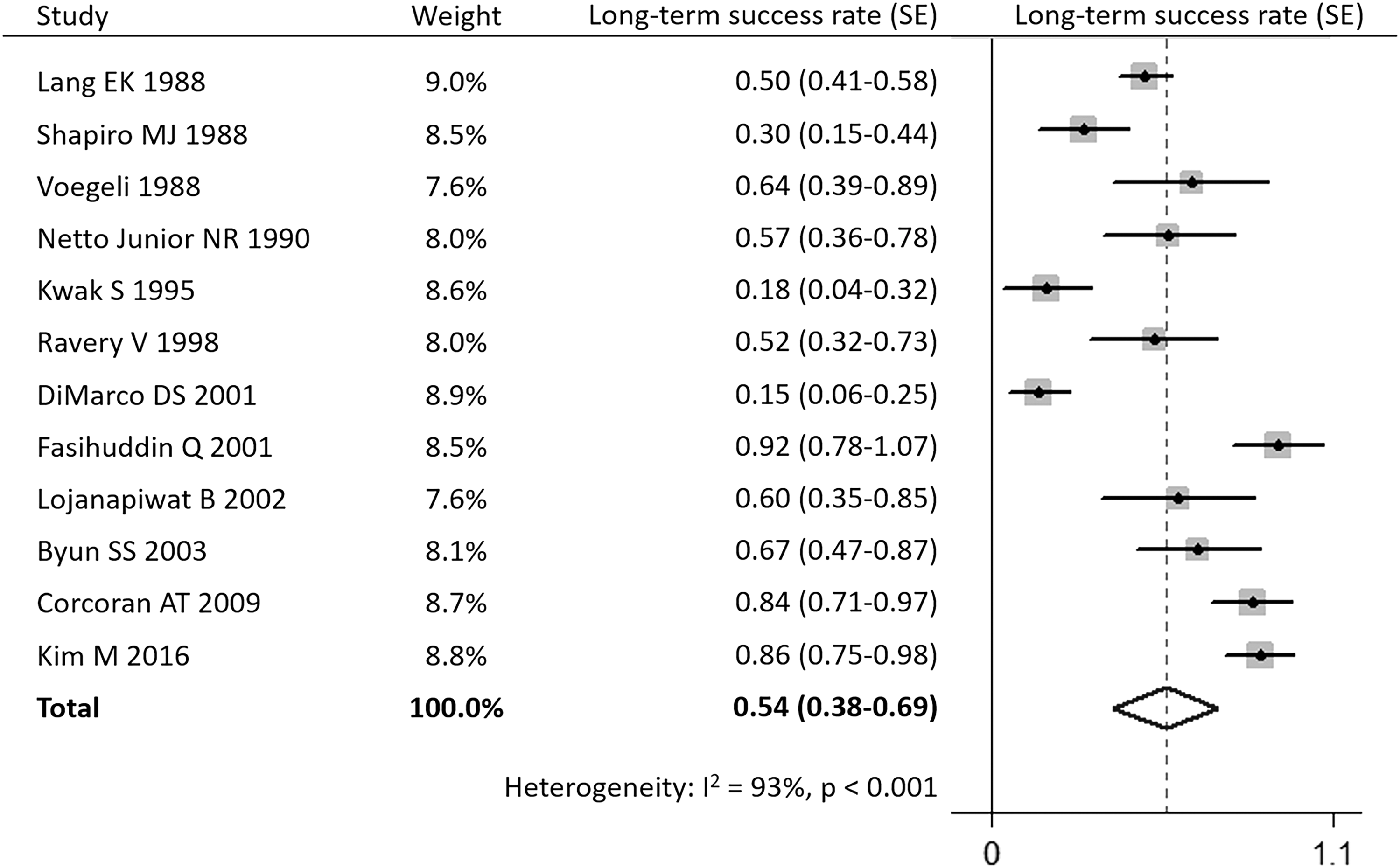
Forest chart for the long-term success rate.
Success rate distinguished by stricture length
Five studies reported the influence of different stricture lengths on efficacy of balloon dilatation treatment. In the subgroup of patients with ≤2-cm ureteral strictures, the average success rate was 69% ± 16%, whereas that in patients with >2-cm ureteral strictures was 19% ± 29%. All studies except one by O'Brien et al. showed that balloon dilatation could achieve better efficacy for shorter stenosis. 22 Meta-analysis using a fixed-effects model demonstrated that the success rate of endoscopic balloon dilatation for ≤2-cm benign ureteral strictures was significantly higher than that for >2-cm ones (OR: 0.13; 95% CI: 0.05–0.35) (Fig. 5A).
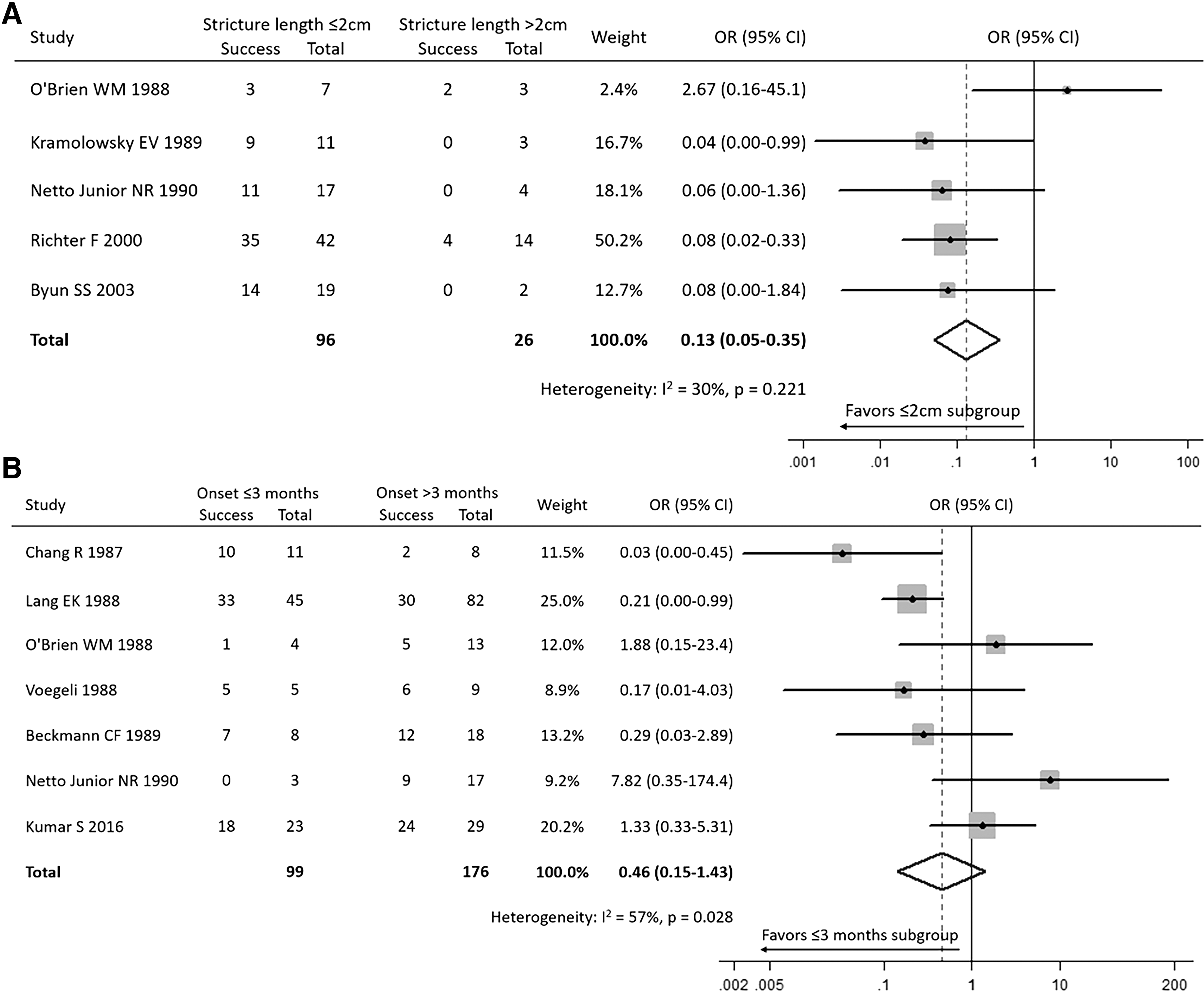
Forest chart showing subgroup analysis of the success rate
Success rate distinguished by stricture onset timing
Seven studies reported the influence of stricture onset timing on the efficacy of balloon dilatation treatment. In the subgroup of patients with stricture onset timing ≤3 months, the average success rate was 65% ± 37%, whereas that in patients with stricture onset timing >3 months was 52% ± 20%. Two studies reported better efficacy with earlier treatment. 20,21 However, the remaining five studies failed to demonstrate a significant influence of onset timing of stricture on treatment outcomes. Meta-analysis using a random-effects model demonstrated that the success rate of endoscopic balloon dilatation for patients with stricture onset timing ≤3 months was relatively higher than that for patients with stricture onset timing >3 months (OR: 0.46; 95% CI: 0.15–1.43) (Fig. 5B).
Discussion
Ureteral strictures mainly develop due to benign, malignant, iatrogenic, or idiopathic causes, with benign and iatrogenic causes accounting for >1/3rd of cases. 1 The incidence of iatrogenic ureteral strictures is reported to be 0.3%–1.5%, of which as much as 58% can be accounted for by endoscopic surgery. 35 Notably, postoperative ureteral strictures rarely occurred before the introduction of ureteroscopy. Since then, however, the incidence rate of postoperative ureteral strictures has increased to 4% 36 and that for incarcerated calculi is as high as 7.8%–26.2%. 2 –4 Ureteral stricture incidence rates after various other procedures are as follows: pelvic radiotherapy, 2%–3% 37 ; ileal ureteral diversion, 1.4%–15% (more likely if the antireflux technique is used for anastomosis) 5 ; and renal transplantation, 3%–8% 6 (upper, middle, and lower strictures are 15%, 12%, and 73%, respectively 38 ). Malignant ureteral strictures can be caused by inner growth of a ureteral tumor or compression by an adjacent organ tumor. In these cases, direct tumor invasion mainly occurs from the genitourinary system and lower digestive tract tumors, mostly affecting the lower ureter. 1
For patients with benign ureteral strictures, the goals of management are to preserve renal function and relieve symptoms while minimizing surgical trauma. Before the development of endoscopic techniques, open surgery was the only treatment option for benign ureteral strictures and local obstruction. However, open surgery can be associated with greater trauma, higher costs, and even patient death. 12 Thus, endoscopic balloon dilatation, stricture incision, or ureteral stent placement should be the preferred management option if a guidewire can be passed through the ureteral stricture. 7
Our meta-analysis found that literature published before 2000 mainly focused on the technical feasibility of endoscopic balloon dilatation. The pooled technical success rate was 89%, indicating that it is technically feasible to treat benign ureteral strictures using this minimally invasive approach. In addition, the pooled short-term (i.e., at 3 months postoperation) success rate was 60%, while the pooled long-term (i.e., at 6–12 months postoperation) success rate was slightly lower at 54%. It is worth noting that long-term success rates reported by most studies after 2000 were better than the pooled long-term success rate, with the highest one being 86%, 32 suggesting that with continuous development of minimally invasive devices and accumulation of practical experience, the endoscopic balloon dilatation technique has become more refined and can now achieve satisfactory treatment outcomes at reasonably high rates. However, among the included studies, the definitions of success varied in terms of follow-up time and assessing approach.
Nevertheless, the therapeutic effect of balloon dilatation can differ depending on conditions such as stricture length (most important), nature, location, and formation time. When stricture length is >2 cm, satisfactory therapeutic effects are seldom achieved. For example, Richter and colleagues found that the success rates of balloon dilatation in patients with ureteral stricture lengths ≤2 cm and >2 cm were 83.3% (35/42 cases) and 28.6% (4/14 cases), respectively. 28 Similarly, Byun et al. showed that while success rates for strictures ≤2 cm at 12- and 36-month follow-ups were 56% and 47%, respectively, no patients with strictures >2 cm were successfully treated during the same follow-up periods. 30 Our meta-analysis data confirmed that the success rate was much higher in the subgroup of ≤2-cm strictures compared with the subgroup of >2-cm ones (69% vs 19%). Previous infection, urinary extravasation, and vascular compromise may be factors in the formation of long ureteral strictures and their resistance to dilation. Since longer strictures usually are of longer duration, they are less likely to be managed successfully. 20
Another important factor determining therapeutic efficacy is the nature of the ureteral stricture, including benign or malignant and ischemic or nonischemic cases. Regarding the former, Byun and colleagues 30 showed that success rates of benign stricture treatment were 67% and 57% at 12 and 36 months, respectively, while those of malignant stricture treatment were only 18% and 14%, respectively. Regarding the latter, Richter et al. showed that the success rate for nonischemic ureteral stricture treatment was 80% (36/45 cases), while that for ischemic ureteral stricture treatment was only 27% (3/11 cases). 28 However, these results should be interpreted with caution as there is no uniform definition of an ischemic ureteral stricture. In their study, Richter and associates 28 suggested that stricture blood supply should be determined based on the cause of stricture formation, with the following six conditions often indicating the potential for poor blood supply to the stricture: ureteral stricture caused by exfoliation of lymph nodes during hysterectomy, ureter movement during aortic bypass grafting, long-term ureteral abscess, high-speed blast injury of a cavity organ near the ureter, ureteral stricture caused by stone incarceration for more than 2 weeks, and ureteral anastomosis with a history of dilatation or incision failure. 28
In addition, the time between stricture formation and treatment may also impact the treatment success rate. In our meta-analysis, balloon dilatation achieved success rates of 65% in ureteral strictures formed ≤3 months before treatment and 52% in strictures formed >3 months before treatment, suggesting that early treatment of ureteral strictures can achieve better outcomes. An aged stricture tends to become denser and more fibrotic, leading to compression of vessels, thereby reducing the flow rate. Decreased oxygenation causes fibrosis and therefore formation of a dense stricture, forming a vicious cycle. Moreover, damage caused by dilatation of the stricture is repaired by deposition of fibroblasts, which is subject to the same vicious cycle. 21 This emphasizes the importance of early detection and treatment for ureteral strictures. Stricture location may also affect therapeutic efficacy of endoscopic balloon dilatation, although reports in literature are contradictory. While one previous study suggested that balloon dilatation is likely to fail for middle ureteral strictures, 39 others have demonstrated that stricture location has no influence on the treatment success rate. 30
Although the studies included in our analysis provided useful insights, there are shortcomings that limit the information our study can offer. First, most current studies on balloon dilatation for ureteral strictures are small-sample retrospective studies that lack standardization of balloon dilatation parameters, with the choice of procedure parameters greatly depending on the surgeon's preference. For example, Corcoran et al. used F15 UroMax balloons with a pressure of 12–14 atmospheres and an expansion time of 4–10 minutes, 31 while Richter et al. chose a 4- to 6-mm diameter balloon with two atmospheres and an expansion time of 90 seconds. 28 Second, there is no agreement on the type of ureteral stent to be placed after endoscopy to maintain ureteral patency. Although research conducted in experimental pig ureters showed that different postoperative stent models have no effect on ureteral patency, 40 another study reported that ureteral stents larger than 12F were associated with an increased endoscopic management success rate. 17 However, larger stents may cause more urinary tract infections and stricture recurrence. 41 Third, there are almost no perioperative renal function data in existing studies, making it impossible to identify differences in renal function between cases of successful and failed treatments. Therefore, a prospective multicenter study with a large sample is needed to more robustly investigate the procedural details and therapeutic effect of balloon dilatation in the treatment of benign ureteral strictures.
Conclusion
Our study indicates that endoscopic balloon dilatation has a high success rate in the treatment of benign ureteral strictures with length ≤2 cm and onset timing ≤3 months. However, there is still no consensus on balloon type, dilatation pressure, expansion number, postoperative ureteral stent type, and stent retention time for the balloon dilatation technique.
Footnotes
Acknowledgments
This work was sponsored by the Shanghai Sailing Program (18YF1422600, W.Z.) and National Key R&D Program of China (2017YFB1302800, X.G.). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author Disclosure Statement
No competing financial interests exist.
Supplementary Materials
Supplementary Table S1
Supplementary Table S2
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.