Abstract

Abstracts
MICRO-COST ANALYSIS DEMONSTRATES COMPARABLE COSTS FOR LithovueTM VERSUS REUSABLE FLEXIBLE URETEROSCOPE USE
Department of Urology, University of California, San Francisco
Department of Urology, Montefiore Medical Center, Albert Einstein College of Medicine, Bronx, NY 10467, United States

Icahn School of Medicine at Mount Sinai
University of Illinois at Chicago, College of Medicine Department of Urology
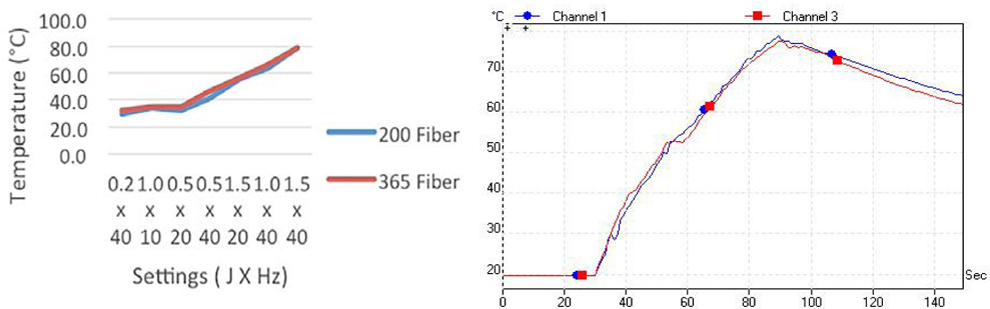
Department of Physics and Optical Science, University of North Carolina at Charlotte
Brady Urological Institute,
Sanador Hospital, Bucharest, Romania
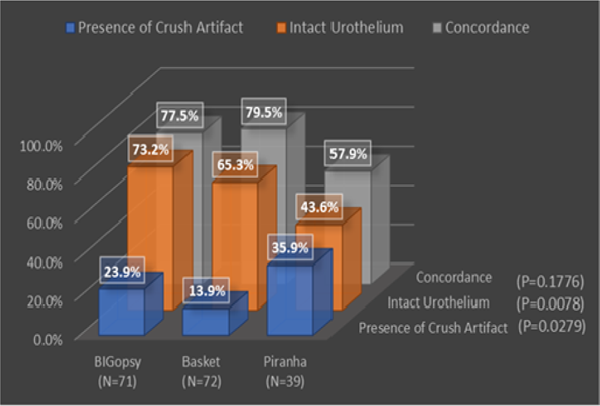
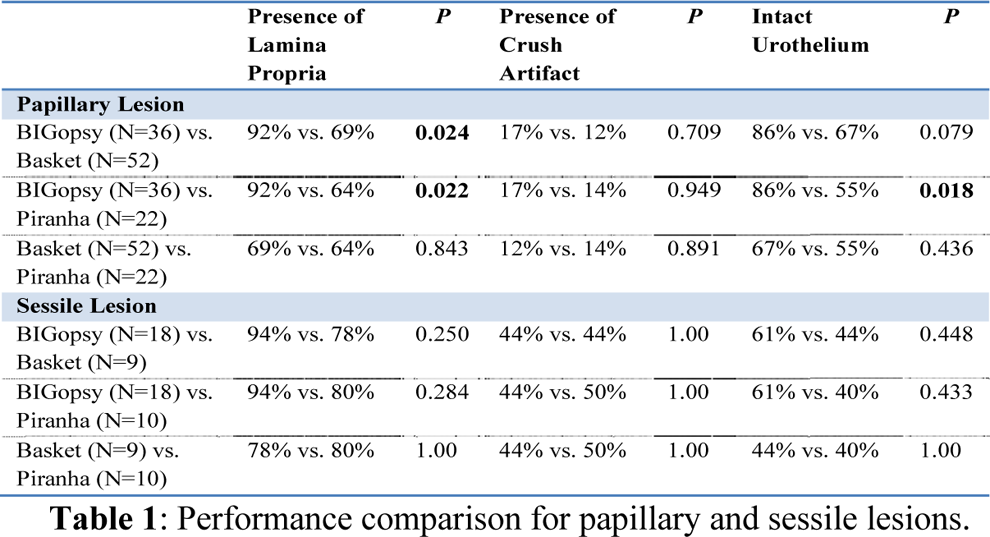
MULTI-INSTITUTIONAL EVALUATION OF QUALITY OF UPPER URINARY TRACT BIOPSY USING BIGOPSY FORCEPS, 2.4F NITINOL BASKET, OR PIRANHA FORCEPS
University of California, Irvine Medical Center, Orange, CA
Department of Urology, The Ohio State University Wexner Medical Center, Columbus, Ohio

Department of Urology, Stanford University School of Medicine, Stanford, CA 94305, USA.
Department of Urology, The Icahn School of Medicine at Mount Sinai, New York, NY
Department of Urology, School of Medicine, University of California - Irvine


Department of Urology, University of California, Irvine, Orange, CA
University of California Irvine, Orange, CA
Hacettepe University Faculty of Medicine, Department of Urology, Turkey

University of Minnesota Mech. Engineering,
Department of Urology, Stanford University, Stanford, CA
Kesem Health, Melbourne, Australia
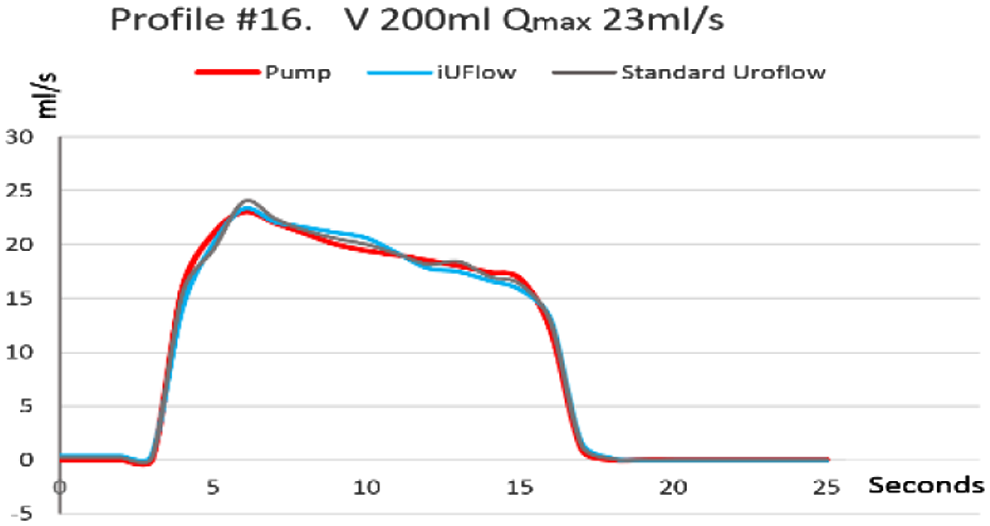
The iUFlow is a compact bladder-monitoring device that placed over the toilet bowl and connects to the patient's smartphone, enabling automated capturing and recording of frequency, volumes as well as uroflowmetry data at home. This is done by an arrangement of sensors under a urine container producing acoustic signals that can be recorded, processed and analyzed via the patient's mobile device. We examined the uroflowmetry capability of the iUFlow and validated it in laboratory settings using different bladder profiles, patterns and scenarios.
HOSPITAL ALEMÃO OSWALDO CRUZ, Prostate Institute - São Paulo SP Brazil

Department of Urology, University of Michigan, Ann Arbor, MI, USA.
Vanderbilt University Medical Center, Department of Urologic Surgery
Institute of Urology, Dhule, Maharashtra, India
Mayo Clinic Florida, Jacksonville Florida
Department of Urology, University of California, San Francisco (UCSF)
Department of Urology, Tokai University Hachioji Hospital
Department of Urology, University of California, Irvine, Orange, CA
Glickman Urological & Kidney Institute, Cleveland Clinic, Cleveland, Ohio
*
3B's Research Group – Biomaterials, Biodegradables and Biomimetics, University of Minho, Headquarters of the European Institute of Excellence on Tissue Engineering and Regenerative Medicine, AvePark, 4805-017 Barco, Guimarães, Portugal
Department of Urology, Tokai University Hachioji Hospital
Department of Physics and Optical Science, University of North Carolina at Charlotte
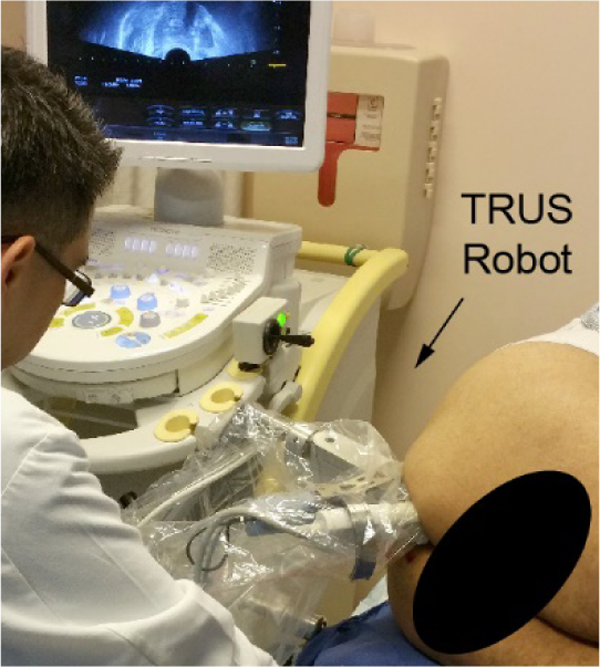
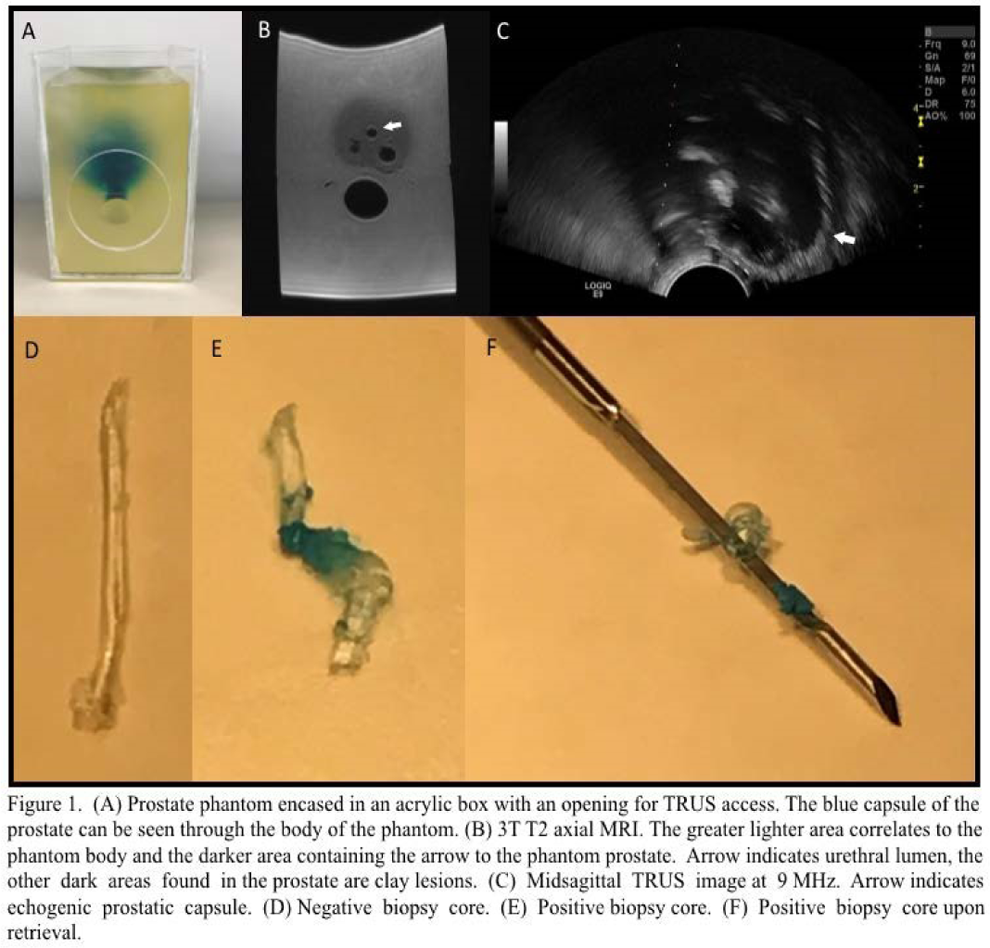
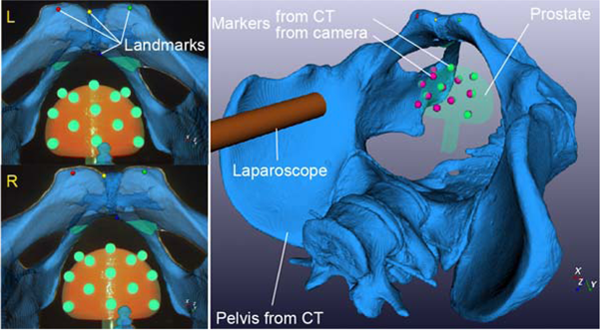
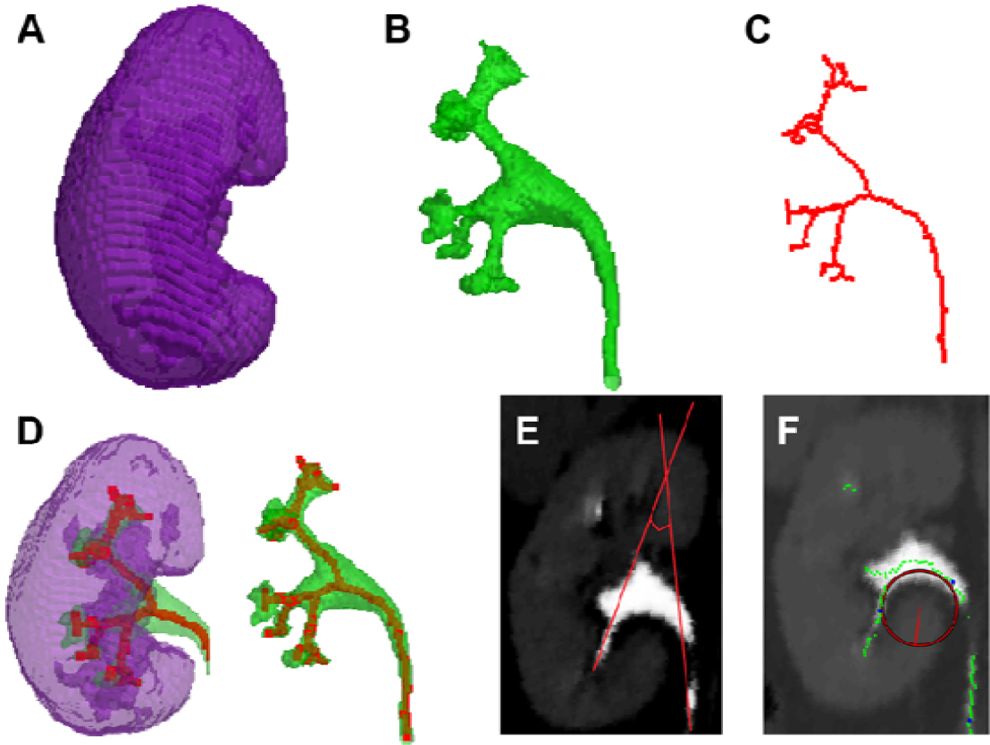
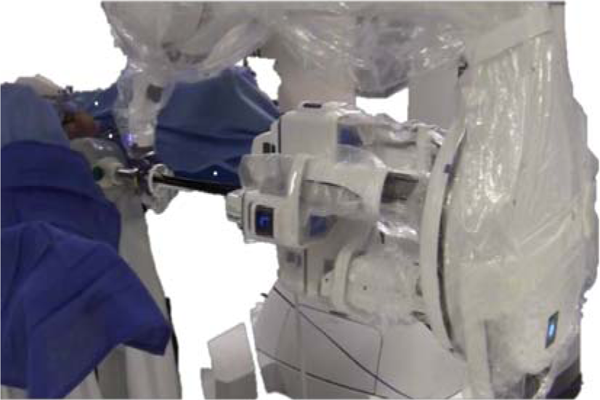
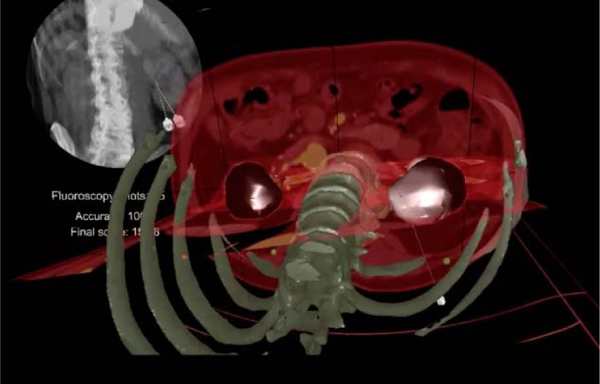
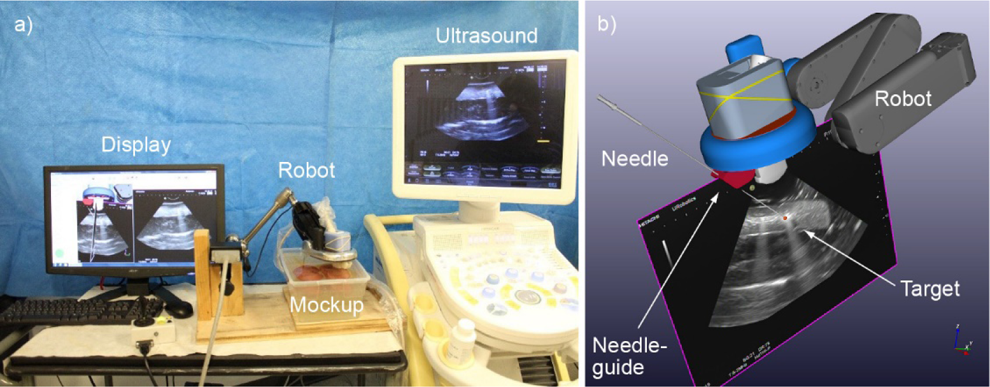
The robot is supported by an arm attached to the procedure table. A standard end-fire TRUS probe (Hitachi-Aloka EUP-V53W) with a needle-guide was attached to the robot. With the patient in a lateral decubitus position, after local anesthesia, the TRUS probe together with the robot was manually placed and positioned to image the prostate, Then, the support arm was locked in place to hold the position (Figure 1). An image scan was performed first. The robot automatically rotated the probe and acquired 2D ultrasound images and their respective positions. The software reconstructed the 3D image of the prostate and surrounding tissues [PMCID:23358940]. The urologist defined the 12-core biopsy plan based on the images. Then, the robot calculated the best approach to each target while optimizing the sequence of the cores. The Max-Core 18Ga x 20cm needle (Bard Biopsy Systems) was used to obtain biopsy cores. The software used the specific needle information to calculate the depth of needle insertion, so that the planned core would be centered on the sample magazine after firing the needle.
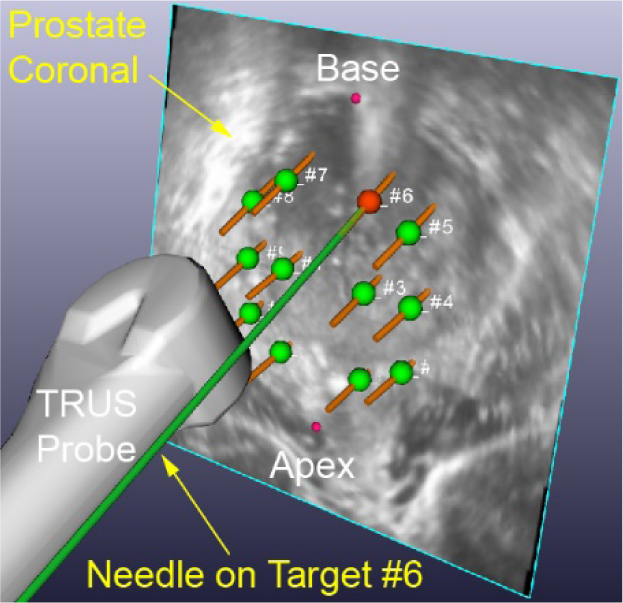
The robot automatically oriented the needle-guide on each target for biopsy. The urologist simply inserted the needle through the needle-guide up to the depth that is marked on the real-time ultrasound image, and fired the biopsy device. For the purpose of the study, images of the fired biopsy needle were acquired before retracting the needle, so that their position could be documented and targeting errors could be calculated.
The images were analyzed after the procedure. Targeting errors were measured as the vector distance between the target point and the center of the biopsy magazine slot on the needle from the images. Targeting accuracy and precision were calculated as the average and standard deviation of the errors.
Sanador Hospital, Bucharest, Romania

Department of Urology, Tan Tock Seng Hospital, Singapore.
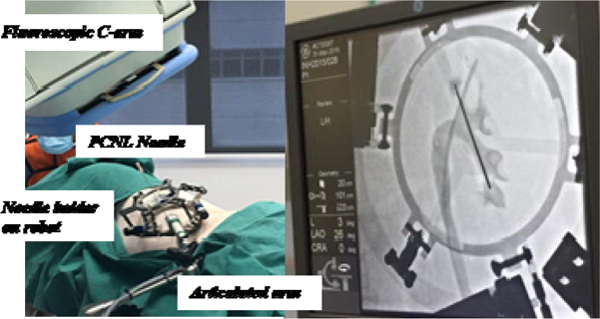
The automated bull's-eye alignment by the software and the stabilization of needle trajectory during puncture enabled the surgeon to attain access more confidently and accurately.
Department of Urology, University of Illinois at Chicago, Chicago, IL.
Department of Urology, The Icahn School of Medicine at Mount Sinai, New York, NY
Urology Institute, University Hospitals Cleveland Medical Center,
San Diego Sexual Medicine
Department of Urology, University of California, Orange, USA,


University of California Irvine, Irvine, CA
This work was partially supported by grant UL1 TR001414 from the National Center for Advancing Translational Sciences, NIH.
Urology Institute, University Hospitals Cleveland Medical Center,
Department of Urology, College of Medicine, University of Florida
University of Washington, Department of Urology, Center of Industrial and Medical Ultrasound
Department of Urology, University of Michigan, Ann Arbor, MI, USA.
Department of Urology, University of Michigan, Ann Arbor, MI, USA.
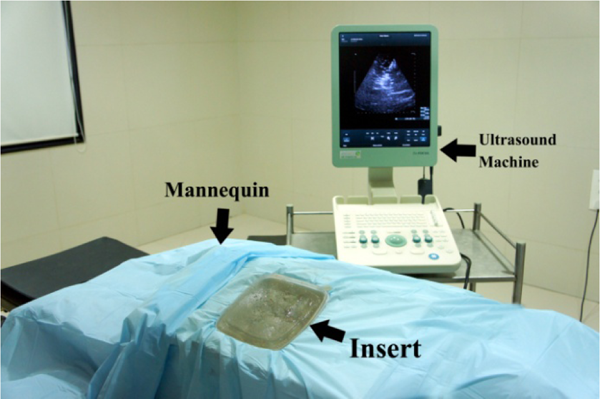
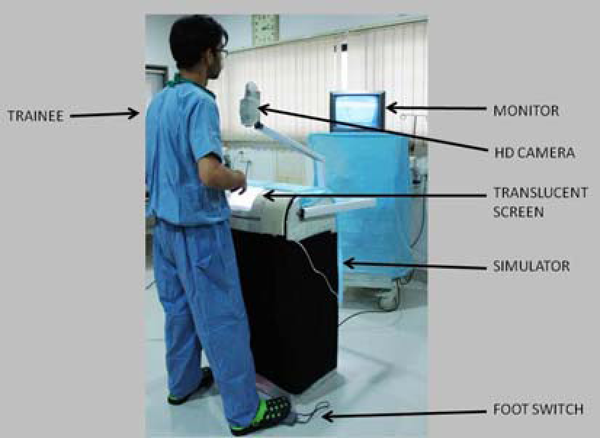
The ultrasound guided perc simulator was then designed, patented and constructed using a designed mix of ultrasound compatible medium, aluminium components, ultrasound compatible organ dummies and a mannequin. The simulator allowed ultrasound guided puncture, saline aspiration for confirmation and wire parking into the kidney/ureter. Evaluation using a 3 step test, GRS score and trainee feedback was analysed using Spearman rank order correlations and paired t test.