
Abstract
Purpose:
To assess the impact of individual operator case volume on shock wave lithotripsy (SWL) treatment outcomes in more than 9000 stone cases over a 20-year period in New Zealand.
Materials and Methods:
Stone cases treated with SWL on the Mobile Medical Technology (MMT) vehicle between June 19, 1995, and December 1, 2014, were identified. Data collection was undertaken prospectively for patient, stone, and treatment characteristics, and retrospectively for treatment outcomes. Multivariate analysis using binary logistic regression was undertaken to assess whether radiographer stone case volume (stones/year) was an independent predictor of SWL success (stone free or clinically insignificant residual fragments ≤4 mm at follow-up).
Results:
Sixteen radiographers delivered treatment to the included cohort (9039 stone cases), with a median case volume (stones/year) of 73 (range: 37–197) and median total of 425 stones treated (range: 71–1721). The two radiographers with highest case volumes achieved the highest success rates. Radiographer case volume (stones/year) was independently associated with SWL success (odds ratio [OR]: 1.004, 95% confidence interval [CI]: 1.003–1.005, p < 0.0001) and reduced need for post-SWL hospital admission (OR: 0.997, 95% CI: 0.994–1.000, p = 0.028), but there was no associated decrease in post-SWL urosepsis (OR: 0.999, 95% CI: 0.974–1.025, p = 0.941), perinephric hematoma (OR: 1.003, 95% CI: 0.985–1.020, p = 0.778), or need for auxiliary procedures (OR: 1.000, 95% CI: 0.998–1.002, p = 0.871).
Conclusions:
SWL success rates can be improved by increasing the frequency of cases performed by individual operators. In this multicenter cohort of more than 9000 stone cases treated over a 20-year period, the best outcomes were seen for those radiographers performing >150 cases per year.
Introduction
Shock wave lithotripsy (SWL) is a well-established treatment option for urolithiasis associated with low patient morbidity. 1,2 Current international guidelines recommend SWL as an equivalent first-line management option to endourology for stones <20 mm in the renal pelvis, upper and middle calices, and for proximal and distal ureteral stones <10 mm. 3 Data from the Hospital Episode Statistics (HES) in the United Kingdom have shown that, while the gap between frequency of ureterorenoscopy (URS) and SWL continues to narrow, SWL remains the most frequently performed treatment option for urolithiasis. 4
In recent decades there has been increasing evidence to suggest that higher volume centers and operators are associated with improved surgical patient outcomes. 5 This has led to the reorganization of clinical services, including the centralization of cancer care in the United Kingdom, and the “Volume Pledge” by major U.S. centers to limit certain procedures to operators meeting defined volume criteria. 6 The Clinical Research Office of the Endourological Society (CROES) has also described improved outcomes with higher volume centers in the context of percutaneous nephrolithotomy and URS as part of a multicenter prospective study. 7,8 While previous studies have observed variation in SWL outcomes by operator experience, they have not looked to assess for an independent association between case volume and outcomes using multivariate analysis. 9,10 This study aimed to assess the impact of individual operator case volume on SWL treatment outcomes in more than 9000 stone cases over a 20-year period in New Zealand.
Materials and Methods
In this retrospective study, an electronic search of the New Zealand Mobile Medical Technology (MMT) database was undertaken to identify stone cases that were treated with SWL on the MMT vehicle between June 19, 1995, and December 1, 2014. Adult stone cases (≥18 years) with renal or ureteral stone(s) were included where they underwent first SWL treatment (i.e., not repeat SWL for previously failed treatment). Stone cases were excluded where they were lost to follow-up with no confirmation of post-SWL stone status, were defined as staghorn, parenchymal, or diverticular, and where they were undertaken by radiographers not employed on a permanent contract with the MMT SWL service.
Data collection was undertaken prospectively for patient demographics, stone and treatment characteristics, and entered into the MMT national SWL database (Microsoft Access, Redmond, WA) by the treating radiographer. Data collection for SWL treatment outcomes and complications was undertaken retrospectively by a data nurse by contacting the radiology department at the center at which follow-up imaging was undertaken. Follow-up imaging across the 20-year study period varied by local treatment protocols and included computed tomography, abdominal X-ray kidney ureter bladder, or intravenous urography, with the MMT SWL service recommending imaging at 1 and 3 months post-SWL.
During the study period, the MMT SWL service delivered treatment at 21 centers across 14 cities in New Zealand, accounting for a patient population of 4.4 million. The fixed Dornier DoLi-S1 lithotripter and its sister model Dornier DoLi-S2 were used from June 19, 1995, to September 15, 2005, and from September 27, 2005, to December 1, 2014, respectively.
The SWL service is delivered by radiographers and supervising urologists. The radiographers are responsible for checking all equipment before each case, use of the picture archiving and communication system, arranging the position of the patient and lithotripter, delivery of fluoroscopy, and postprocedure documentation. The process of stone identification, monitoring of target points, and confirmation of power and total shock waves are supervised by the urologist, and performed by the radiographers. Urologists are also responsible for coordinating the safety brief “Time Out” process, reviewing the patient's clinical details, discussing treatment, and consenting the patient.
Prerequisites for employment of radiographers by the MMT service were that they had completed a BA in Medical Imaging and held a scope of practice, as governed by the New Zealand Institute of Medical Radiation Technology (NZIMRT). Radiographers were not required to have previous experience in SWL although this was considered desirable. Training of new MMT radiographers in SWL lasted ∼4 weeks with direct supervision provided by the lead radiographer. Twenty observed stone cases were considered a minimum requirement, but the decision for independent radiographer practice was at the discretion of the lead radiographer based on individual radiographer performance. An MMT SWL user manual outlining key protocols and clinical responsibilities was delivered to radiographers with the purpose of ensuring consistency across practice. During the study period, there were four radiographers employed by the MMT service at any one time, and they shared a 4- to 5-week visiting circuit of the 21 NZ hospitals at which the SWL service was delivered.
The type of anesthetic or sedation delivered during SWL was selected on the basis of individual preference of the responsible anesthetist and the patient. The delivery of prophylactic antibiotics, ultrasound imaging, need for auxiliary procedures, including ureteral stenting or nephrostomy placement, were overseen by a total cohort of 82 urologists. The diagnoses of acute urinary tract infection, abdominal aortic aneurysm, pregnancy, uncorrected coagulopathy, pelviureteric junction obstruction and ureteral stricture, or cardiac pacemaker were considered contraindications for SWL.
Treatment success was defined as complete stone clearance (stone free) or clinically insignificant residual fragments (CIRFS) of ≤4 mm on radiologic imaging at the time of follow-up. Multivariate analysis using binary logistic regression was undertaken to assess whether radiographer stone case volume (stones/year) was an independent predictor of SWL success, postoperative complications or auxiliary procedures, or need for hospital admission. Statistical analysis was performed using SPSS software, version 24 (SPSS, Inc., Chicago, IL). Simple linear regression was undertaken to model the relationship between operator case volume and success rate (Excel 2016; Microsoft, WA).
Results
The electronic search identified 11,481 first treatment stone cases treated with SWL over the 20-year study period. Of these, 2442 (21.3%) were excluded from the analysis: 17.1% (n = 1962) due to loss to follow-up, 3.0% (n = 341) because they were defined as staghorn, diverticular, or parenchymal, and 1.2% (n = 139) because they were undertaken by radiographers not employed on a permanent contract with the MMT SWL service.
Table 1 describes the patient characteristics of included stone cases. The mean stone size was 9.9mm (SD: 4.9), and the majority of cases were undertaken under general anesthesia (87.4%), in the supine position (98.9%) with fluoroscopy imaging alone (91.0%) (Table 2). The overall treatment success rate was 49.2% (35.9% stone free, 13.3% CIRFS), with 6.7% (n = 627) of cases requiring post-SWL hospital admission and 9.5% (n = 891) requiring post-SWL auxiliary procedure (Table 2).
Patient and Stone Characteristics
Shock Wave Lithotripsy Treatment Characteristics and Postoperative Complications
SWL = shock wave lithotripsy.
During the 20-year study period, a total of 16 radiographers delivered treatment to the included cohort, with a median case volume (stones/year) of 73 (range: 37–197) and median total of 425 stones treated (range: 71–1721) (Table 3). SWL treatment success rates varied by stone case volume; the two radiographers associated with best overall success rates of 62.1% (radiographer O) and 66.4% (radiographer P) had case volumes of 132 and 171 stones per year, respectively (Table 3) (Fig. 1). The included cases were supervised by 81 urologists, with a median supervised case volume of 16 (range: 1–33).
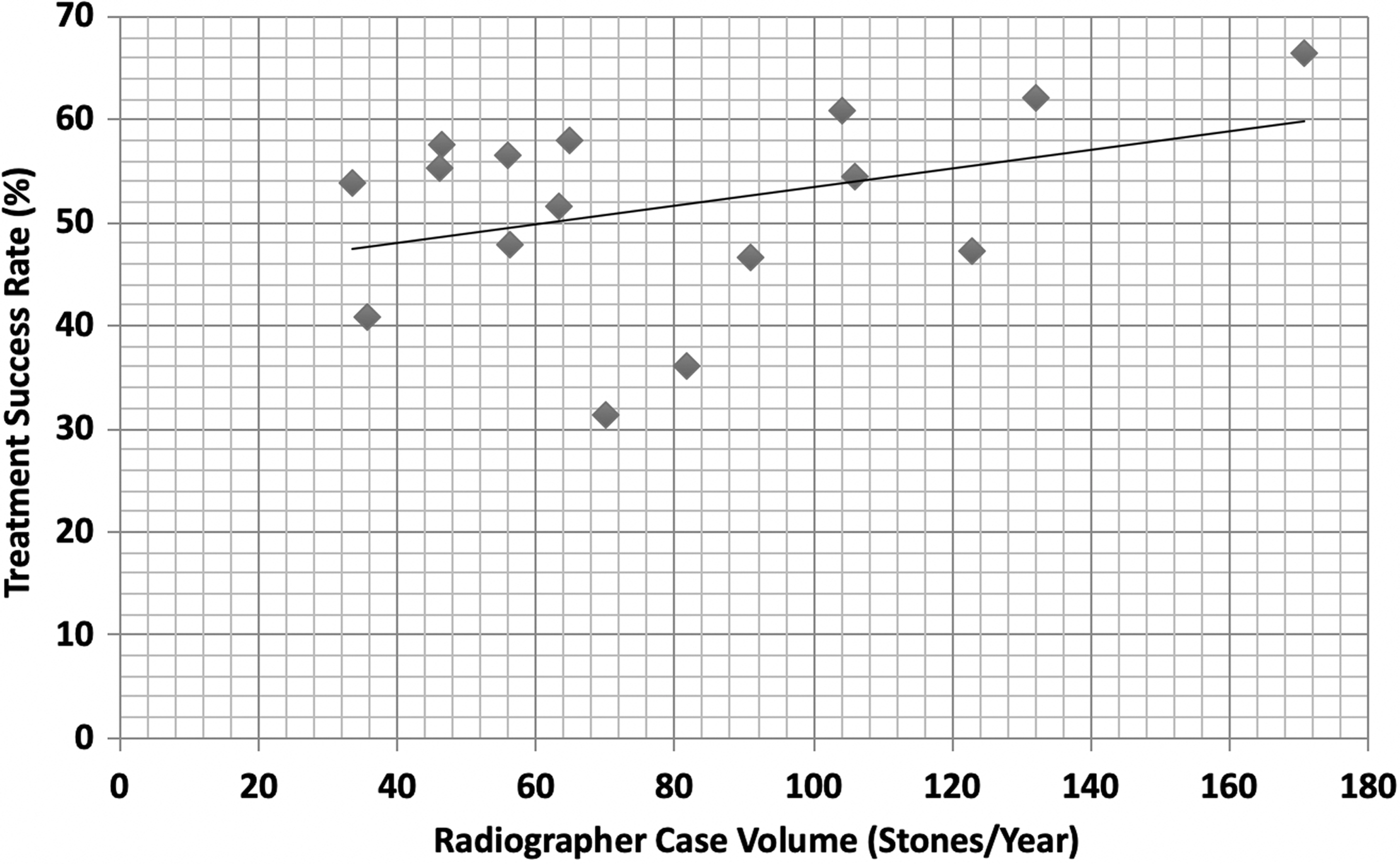
Shock wave lithotripsy treatment success rates by radiographer case load (stones/year).
Shock Wave Lithotripsy Treatment Success Rate by Radiographer Case Load (Stones/Year)
Success rate (%): <40 in italic; 40–50 in bold; 51–60 in bold italic; >60 in underline.
MMT = Mobile Medical Technology.
Radiographer case volume (stones/year) was independently associated with SWL success (odds ratio [OR]: 1.004, 95% confidence interval [CI]: 1.003–1.005, p < 0.0001) on adjusting for other factors within the multivariate binary logistic regression model (Table 4). Further multivariate models incorporating the same independent variables demonstrated that a higher radiographer case volume was also associated with reduced need for post-SWL hospital admission (OR: 0.997, 95% CI: 0.994–1.000, p = 0.028), but there was no associated decrease in post-SWL urosepsis (OR: 0.999, 95% CI: 0.974–1.025, p = 0.941), perinephric hematoma (OR: 1.003, 95% CI: 0.985–1.020, p = 0.778), or need for auxiliary procedures (OR: 1.000, 95% CI: 0.998–1.002, p = 0.871). On substituting radiographer case volume (stones/year) for total radiographer stones treated in the multivariate model, no independent association was found with treatment success (OR: 1.0, CI: 1.000–1.000, p = 0.210).
Multivariate Analysis for Factors Predicting Shock Wave Lithotripsy Success
Other = epidural or neuroleptic sedation.
p < 0.05.
CI = confidence interval; OR = odds ratio.
Discussion
This study demonstrated that a higher SWL operator case volume (stones/year) was independently associated with improved treatment success rates and reduced need for post-SWL hospital admission. This analysis was performed in a large cohort of >9000 stone cases treated by 16 radiographers and made use of a national, multicenter database collated over a 20-year period in New Zealand.
The MMT service in New Zealand uses radiographers as the primary operator of SWL, with clinical supervision delivered by the urologist, and for this reason radiographers were chosen as the operators of interest for this study. Urologists and experienced radiographers delivered training of new radiographers over the complete national circuit over 4 to 5 weeks. This facilitated a smaller number of total primary operators dedicated to SWL who would work across multiple centers, and thus potentially also a larger case volume for each radiographer than may be seen in centers where SWL is delivered primarily by urologists with other clinical commitments (the median case volume for radiographers was 73 vs supervised case volume of 16 for urologists in our cohort). While recent reports have outlined significant variation in the models of SWL service utilized across the United Kingdom, 11,12 there is also evidence to demonstrate comparable efficacy and safety outcomes between experienced urologists and radiographer technicians. 13
This study demonstrated wide variation in SWL success rates by operator (range: 31.4%–66.4%), with the two radiographers with the highest case volumes (radiographers O and P) recording the highest success rates (62.1% and 66.4%, respectively). While other studies have observed improved outcomes in higher volume SWL operators, they did not assess if case load was an independent predictor of outcome across all operators in a multivariate model. 9,10 Although there was no evidence to demonstrate an association between case volume and specific complications in this study, this may be due to the relative infrequency of SWL complications compared with other endourologic procedures. Furthermore, the finding that hospital admission was associated with lower case volume may be due to an increased frequency of complication(s) not recorded by this study, such as postoperative pain.
The most common explanation for the positive relationship between case volume and patient outcomes relates to that of “practice making perfect” and that greater experience in a specific procedure leads to greater proficiency. 6 In the context of SWL, this may specifically relate to the improved ability of the operator to identify the stone using fluoroscopy or optimize the use and number of shock waves delivered. 10 However, this study observed that case load (stones/year), but not the total number of stones treated, was important, and therefore, a higher frequency of treatment delivery by the operator is required to maintain a high standard of performance. It may be the case that those operators who performed SWL with the greatest frequency were also able to create a more effective collective team performance, working with the anesthetist, urologist, and nursing staff, to deliver improved SWL outcomes. 7
In many health care systems, increasing the case load of individual operators would likely require that fewer operators and/or centers are able to deliver SWL. In the absence of any obvious survival or complication benefit, it is unclear if the subsequent need to travel further geographically would be acceptable to the patient. 14 Case volume will continue to represent an imperfect proxy for quality with some lower volume operators achieving good outcomes. 6 However, the best SWL outcomes in this study were generally achieved by radiographers who performed >150 cases per year.
The authors acknowledge a number of limitations of this study. This includes that the multivariate analysis did not include all factors that have previously been associated with SWL outcome, including obesity and stone density, due to the lack of prospectively collected data. This study was also unable to account for potential variation in the level of previous SWL experience held by individual radiographers at the time of starting with the MMT service or on the potential impact of supervising urologists on outcomes. However, new MMT SWL radiographers did not typically have prior SWL experience and the use of a standardized training program and service manual would have minimized the impact of any such variation at the time of commencing independent practice. While the majority of patients received follow-up of their postprocedure imaging (82.9%), it is also possible that stone cases lost to follow-up acted as a confounding factor.
Conclusions
SWL success rates can be improved by increasing the frequency of cases performed by individual operators. In this multicenter cohort of >9000 stone cases treated over a 20-year period, the best outcomes were seen for those radiographers performing >150 cases per year.
Footnotes
Author Disclosure Statement
No competing financial interests exist.