
Abstract
Introduction:
Radical cystectomy (RC) is the mainstay of treatment for muscle-invasive bladder cancer. In 2003, the first robot-assisted radical cystectomy (RARC) was performed and since then many studies, mainly observational, were conducted to compare robotic and open methods. This study aims to assess perioperative outcomes between the two methods based on pooled data from existing literature.
Methods:
A literature search of articles in English and French languages was performed in three databases (Medline, Embase, and Cochrane) until 30th of June 2018, as well as in urology conference programs and reference lists of included studies. The study protocol was registered at PROSPERO (CRD42018103063). Terms such as “robotic,” “open,” and “radical cystectomy” and synonyms were used for the searching algorithm. The primary outcome was the number of minor and major postoperative complications (Clavien grading system). Risk of bias was assessed with the Cochrane tool and Newcastle–Ottawa scale. Comparison of continuous outcomes was performed with weighted mean differences, while for dichotomous outcomes, odds ratios (ORs) were used. Review Manager 5.3 was used.
Results:
Fifty-four studies (5 randomized trials and 49 observational) were eligible, including 29,697 patients (6500 in the RARC group and 23,197 in the open radical cystectomy group). Minor complications (grade 1–2) in pooled data of 29 studies were fewer in the RARC group (OR = 0.54, 95% confidence interval [CI]: 0.38–0.76, p < 0.001), a difference persisting after sensitivity analysis for 30 and 90 days. Major complications (grade 3–5) in 31 studies were fewer in the RARC group (OR = 0.78, 95% CI: 0.65–0.94, p = 0.009), but this difference disappeared in the 30-day subanalysis. RARC was associated with lower blood transfusion rates (p < 0.001), lower length of stay (p < 0.001), faster return to regular diet (p < 0.001), and lower postoperative mortality rates (p < 0.001), but longer operating time.
Conclusions:
RARC appears to be associated with fewer complications and favoring perioperative outcomes in comparison with the open method. Due to the observational nature of most studies, larger randomized trials are needed to confirm these findings.
Introduction
Bladder cancer is the ninth more frequent cancer worldwide, with the highest incidence in southwestern Europe, North America, North Africa, and West Asia, whereas it ranks in the 13th position in terms of death rates. 1 Despite its increased incidence, the bladder cancer mortality rate is decreasing in most Western countries, 2 a fact which underlies that disease management is of paramount importance. Currently, open radical cystectomy (ORC) remains the mainstay of treatment for muscle-invasive and high-risk nonmuscle-invasive bladder cancer (MIBC), 3 but with the cost of a relatively increased mortality rate of 1.2% to 8% at 90 days postoperatively. 4 Decreasing complication rates was the main goal of development of minimally invasive alternative techniques such as robotic radical cystectomy (RC). Robotic cystectomy was first reported by Menon and coworkers 5 and was implemented by many other surgeons, transforming it into a safe and efficient alternative to the open gold standard procedure. 6 Nevertheless, superiority of one of the two techniques over the other is yet to be demonstrated. The goal of our meta-analysis (MA), which to our knowledge is the largest in the literature, is to compare complication rates between open and robotic RC to determine the safety superiority, if any, of one of the two procedures.
Methods
The protocol of this systematic review (SR) and meta-analysis was based on Meta-analysis of Observational Studies in Epidemiology (MOOSE) guidelines 7 and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 8
Data sources and selection
Two authors (T.L. [Tzelves Lazaros] and M.D. [Manatakis Dimitrios]) performed an SR of literature to identify studies, in English and French languages, published in Medline, EMBASE, and Cochrane Central Register of Controlled Trials and Cochrane Database of Systematic Reviews from inception to 30th of June 2018. Each database was searched independently and duplicates were removed. Reference lists from included studies, previous SRs, and MAs were also screened. Randomized controlled trials (RCTs) and prospective or retrospective observational studies were eligible for inclusion in contrast with case reports/series and comments. Conference abstracts were not included due to insufficient reported data. Discrepancies between two authors were resolved after review by a third author (L.L.).
Types of interventions and outcomes
The population of interest was patients with MIBC of any histological type and who were eligible for RC with either the open or robotic procedure. The primary outcome of interest was the overall complication rate between ORC and robot-assisted radical cystectomy (RARC), graded with the Clavien-Dindo system into minor (grade 1–2) and major (grade 3–5) complications. 9 Secondary outcomes were operative time in minutes, estimated blood loss (EBL) in mL, blood transfusion rates (intra- and postoperatively), length of stay (LOS) in days, readmission rates, return to regular diet in days, and mortality rate.
Data extraction
Two authors (T.L. and M.D.) independently performed extraction of baseline characteristics (age, body mass index, proportion of male patients, neoadjuvant chemotherapy and pelvic radiation history, ASA score, and pathological staging) as well as primary and secondary outcome data whenever they were reported. Disagreements were resolved after further review by two authors (L.L. and N.K.).
Risk of bias assessment
Two authors (T.L. and M.D.) independently assessed risk of bias using the Newcastle–Ottawa scale 10 for observational studies. Whenever seven or more of nine stars were received, the study was considered to be of high quality. RCTs were evaluated using the Cochrane Collaboration Risk of Bias Tool. 11
Heterogeneity and publication bias assessment
We evaluated the presence of publication bias regarding report of primary outcomes by visual inspection of funnel plots. Heterogeneity between studies was assessed with the chi-squared (χ 2 ) test and I2 statistic of quantification.
Data synthesis and analysis
Review Manager 5.3 software (Cochrane Collaboration, 2014; the Nordic Cochrane Centre, Copenhagen, Denmark) was used for conducting the meta-analysis. Dichotomous baseline characteristics are described as proportions, while continuous characteristics are described as means ± standard deviations (SDs). Continuous variables were compared using mean differences (MDs), while dichotomized variables were compared with odds ratios (ORs) and 95% confidence intervals (CIs). In studies where median (interquartile range) was reported instead of mean and SD, data were transformed using formulas given by Hozo and colleagues 12 and Wan and colleagues. 13 A random-effects model was used for all comparisons.
Results
Study selection and characteristics
We identified 805 studies from initial literature search. After removal of 33 duplicates, we screened 772 titles and abstracts, reviewed 102 full-text articles, and finally analyzed 54 of them. 14 –66 Basic characteristics of patients involved in these studies are shown in Table 1, whereas basic characteristics of the studies are shown in Table 2. The flow diagram of our analysis is shown in Figure 1.
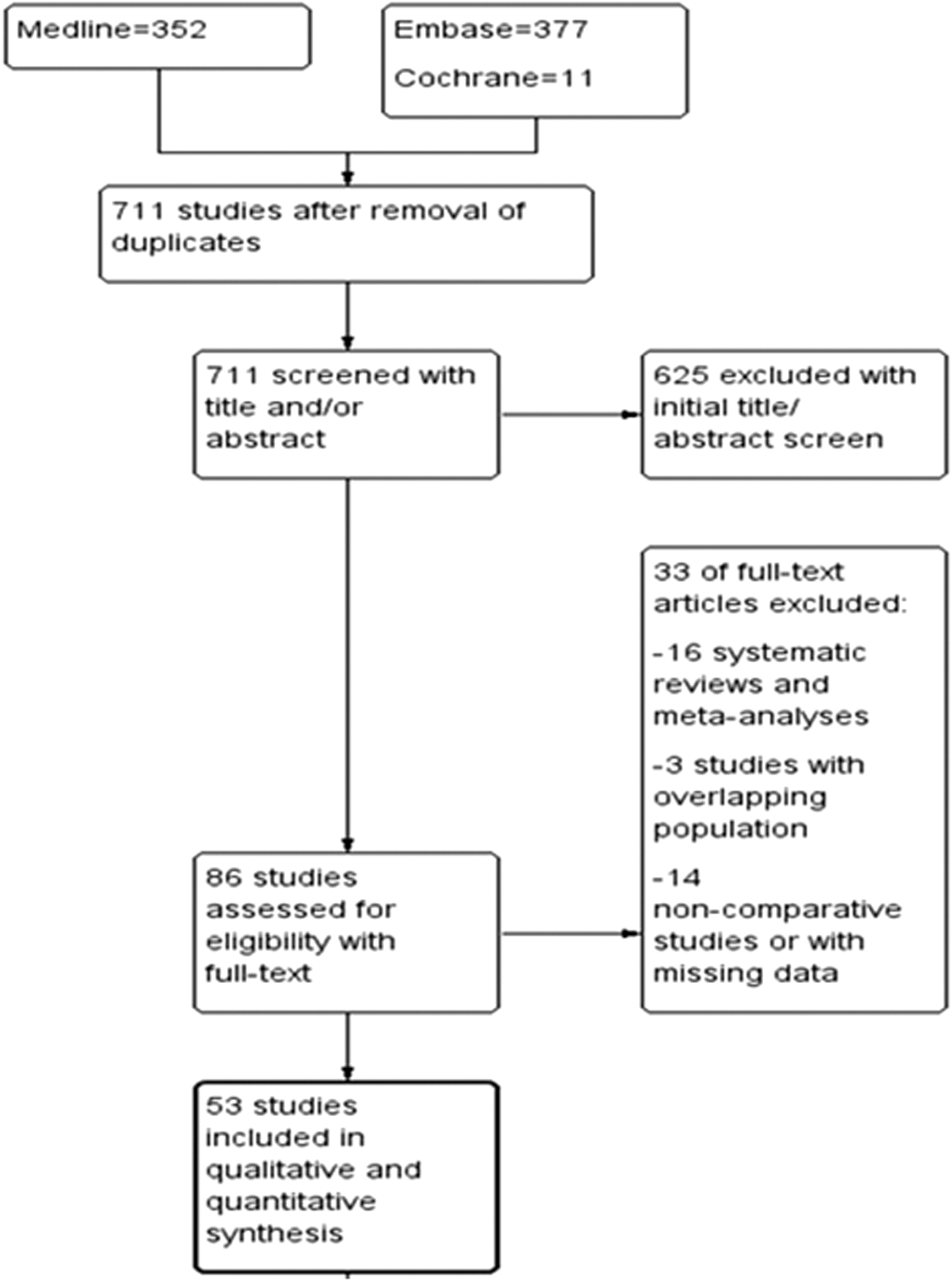
Flow diagram.
Patient Characteristics
BMI = body mass index; ORC = open radical cystectomy; RARC = robot-assisted radical cystectomy; SD = standard deviation.
Study Characteristics
EUD = extracorporeal urinary diversion; IUD = intracorporeal urinary diversion; NOS = Newcastle-Otawa Scale; RCT = randomized controlled trial.
Three studies were excluded due to overlapping populations, while in one case, studies from the same center were included 23,44 since different outcomes or subpopulations were reported. There were 5 RCTs 60 –64 and 49 observational studies in total, including 29,697 patients (23,197 in the ORC group and 6500 in the RARC group). RARC was regarded as the experimental arm. We grouped complications into minor (Clavien grade 1–2) and major (Clavien grade 3–5) complications.
Complications
Minor (Clavien grade 1–2) complications
Pooled data from 29 studies analyzing minor overall complications within 30 or 90 days in 1802 patients in the RARC group and 1961 patients in the ORC group revealed significantly fewer complications in the RARC group (OR = 0.54, 95% CI: 0.38–0.76, p < 0.001). This difference persisted when sensitivity analysis was performed for both 30 days (OR = 0.30, 95% CI: 0.14–0.66, p = 0.003) and 90 days (OR = 0.71, 95% CI: 0.51–0.99, p = 0.04) (Fig. 2a–c). Nevertheless, this difference did not sustain when only RCTs were analyzed (OR = 0.68, 95% CI: 0.38–1.23, p = 0.2) (Fig. 2d). The funnel plot indicates a low risk of publication bias (Fig. 2e).
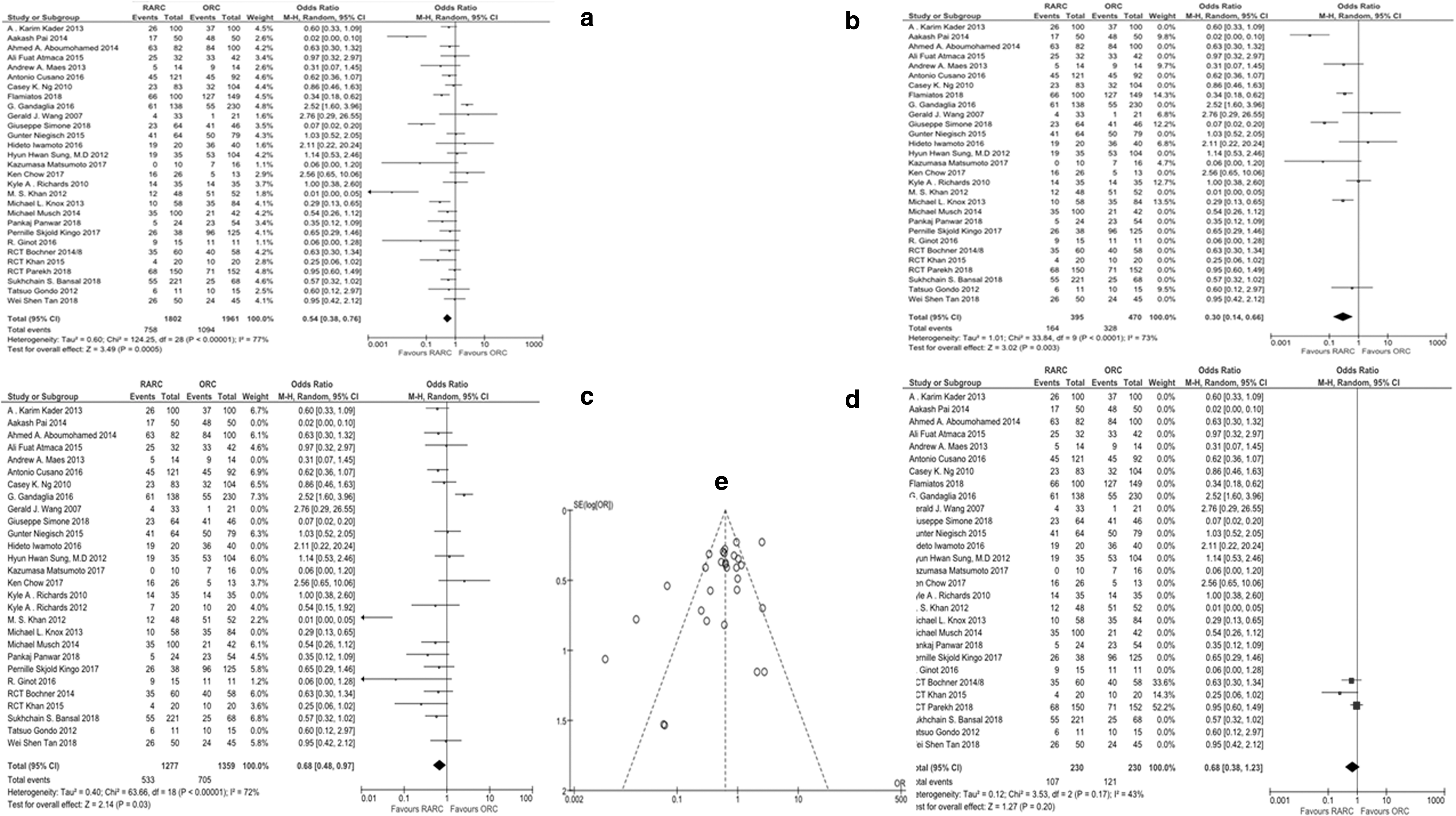
A subgroup analysis for RARC facilitating extracorporeal urinary diversion (EUD) vs ORC, using data from 20 studies (1030 vs 1200 patients, respectively), revealed results in favor of RARC with OR = 0.46 (95% CI: 0.30–0.69, p < 0.05). Even though the same subgroup analysis for RARC with intracorporeal urinary diversion (IUD) vs ORC using data from 4 studies (361 vs 172 patients, respectively) revealed results in favor of RARC, they did not reach statistical significance (OR = 0.54, 95% CI: 016–1.79, p = 0.31).
Major (Clavien grade 3–5) complications
Pooled data from 31 studies analyzing major overall complications within 30 or 90 days in 1834 patients in the RARC group and 2018 patients in the ORC group showed less risk in the RARC group (OR = 0.78, 95% CI: 0.65–0.94, p = 0.009). This difference persisted for subgroup analysis of the 90-day complication rate (OR = 0.78, 95% CI: 0.62–0.99, p = 0.04), but not for the 30-day complication rate (OR = 0.78, 95% CI: 0.54–1.14, p = 0.20) (Fig. 3a–c) and RCT subgroup analysis (OR = 1.02, 95% CI: 0.66–1.59, p = 0.92) (Fig. 3d). Based on visual assessment, there seems to be no publication bias for grade 3 to 5 complications (Fig. 3e).
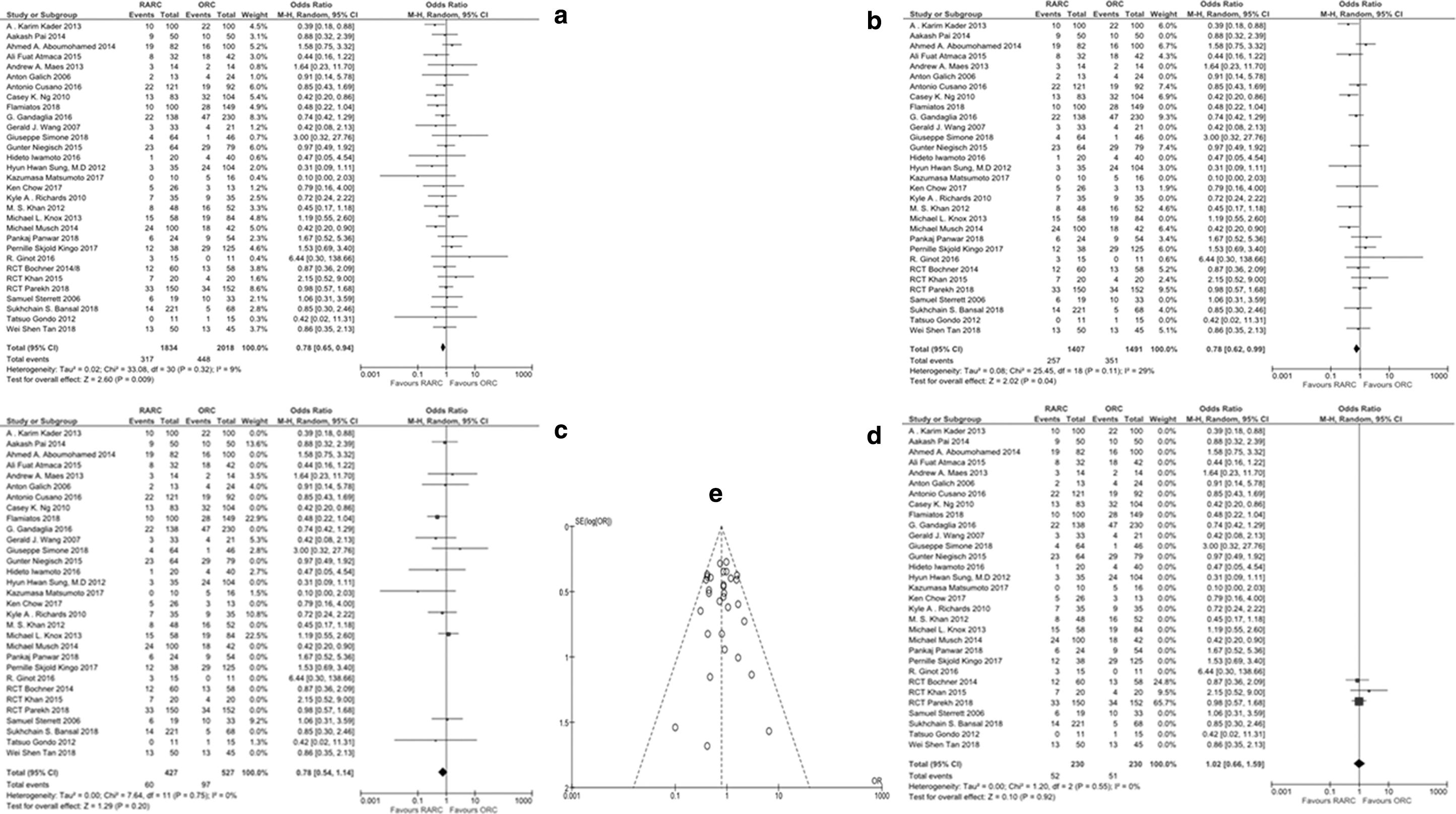
A subgroup analysis for RARC with EUD vs ORC revealed persistent results (in favor of the former) using data from 21 studies (1043 vs 1224 patients, respectively) with OR = 0.70 (95% CI: 0.55–0.89, p < 0.05). The same subgroup analysis for RARC with IUD vs ORC using data from 4 studies (361 vs 172 patients, respectively) failed to prove any significant difference between the 2 modalities (OR = 0.93, 95% CI: 0.51–1.71, p = 0.82).
Perioperative outcomes
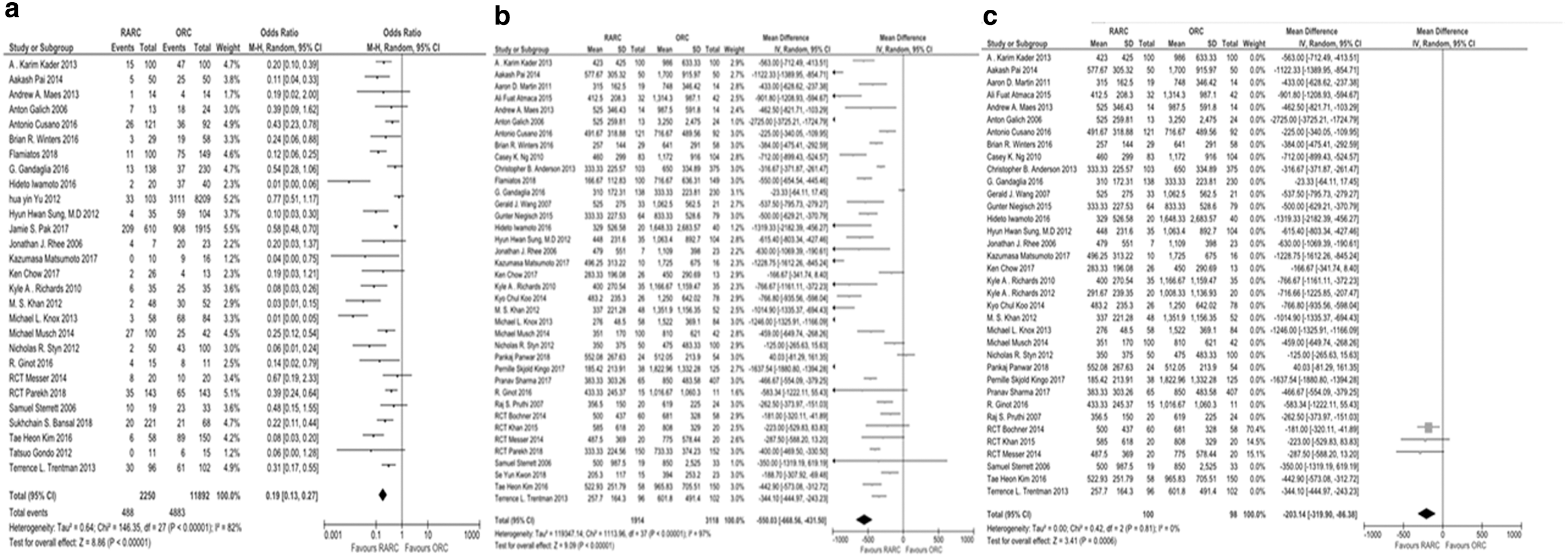
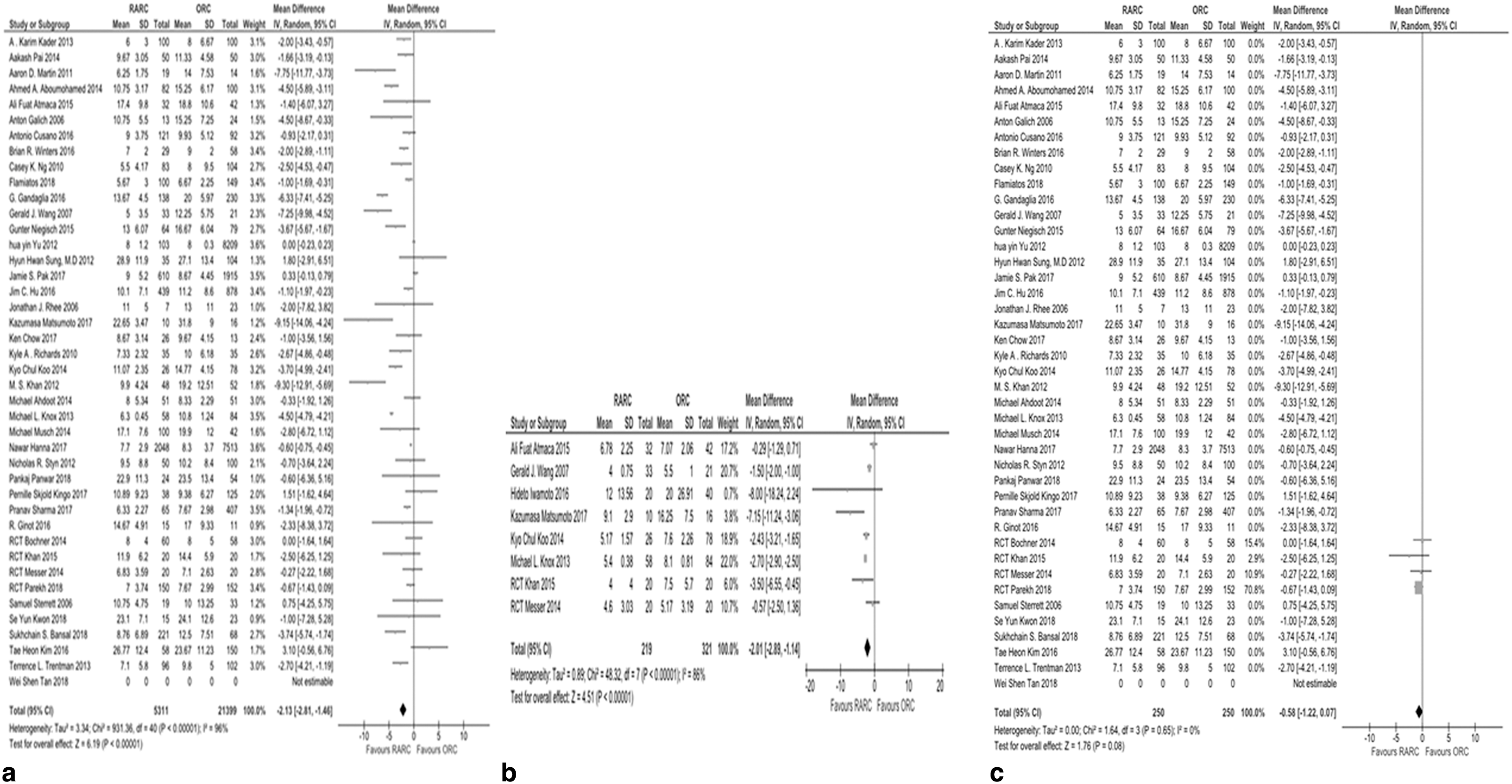
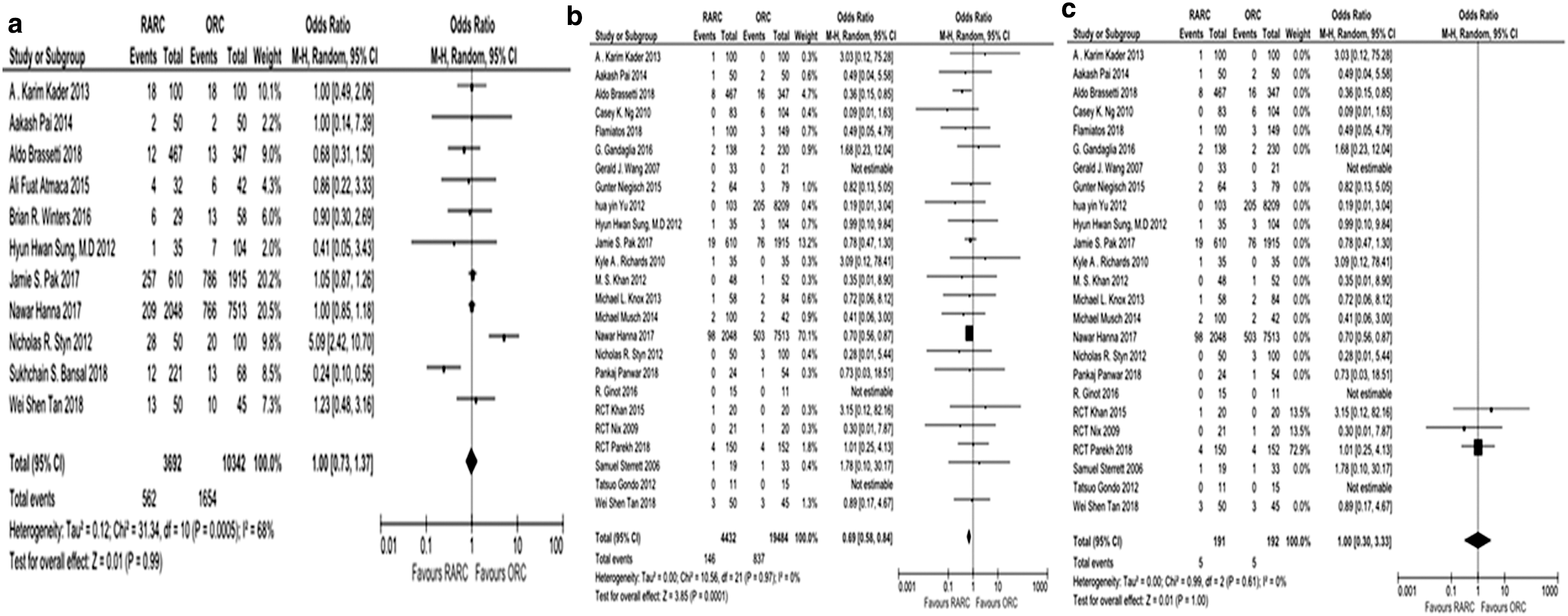
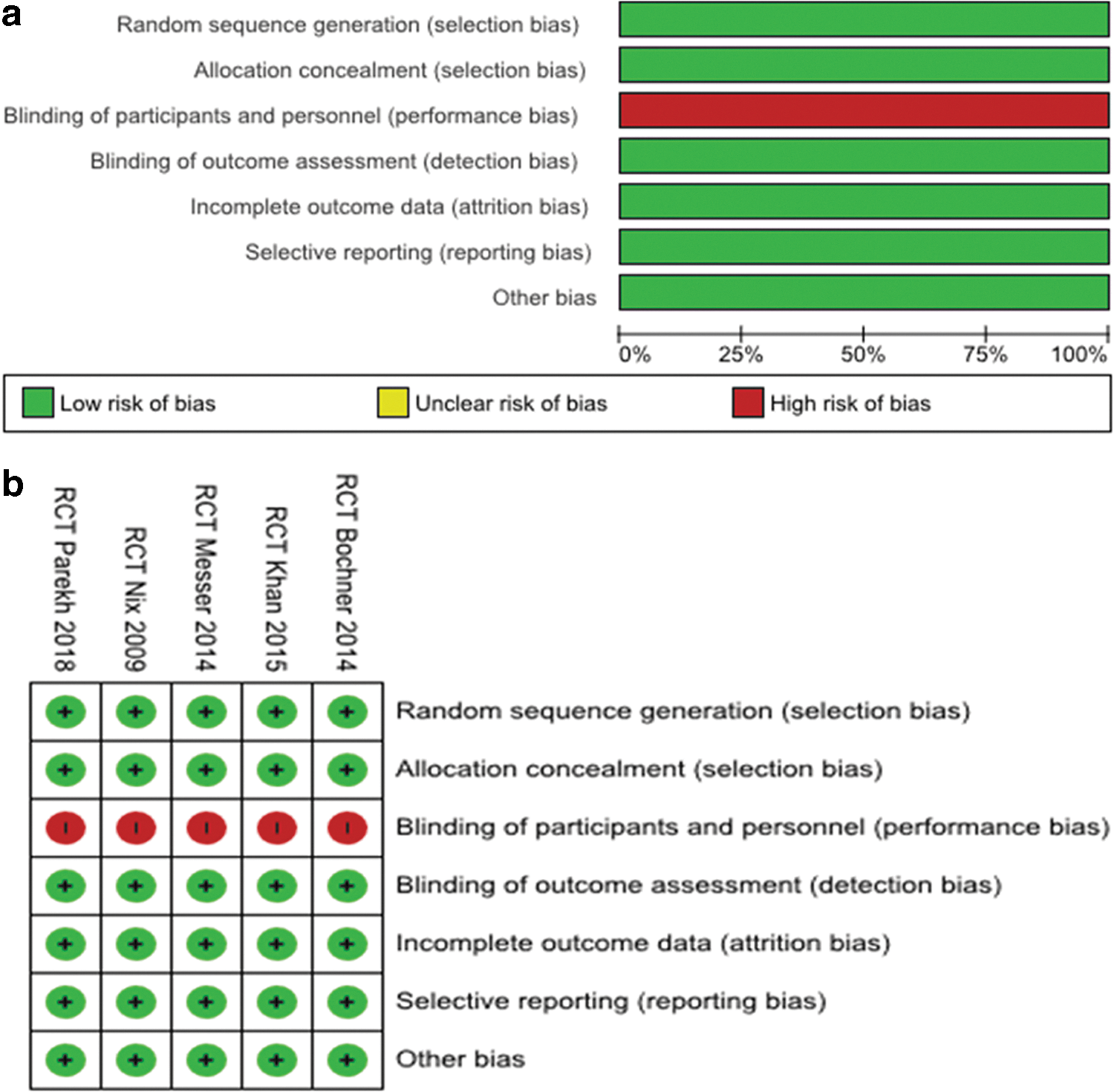
Blood transfusion rates and EBL rates were significantly lower in the RARC group (OR = 0.19, 95% CI: 0.13–0.27, p < 0.001; and MD = −550.03 mL, 95% CI: −668.56 to −431.50, p < 0.001, respectively). The last finding was also reinforced by results of the RCT-only analysis (Fig. 4a–c). Similarly, LOS and time to regular diet favored the RARC group in contrast to operative time. When sensitivity analysis of only RCTs was performed, LOS did not differ significantly between the two groups (Fig. 5a–c). Finally, readmission rates did not differ significantly between the two groups (OR = 1.00, 95% CI: 0.73–1.37, p = 0.99). The postoperative mortality rate was found to be lower in the RARC group (OR = 0.69, 95% CI: 0.58–0.84, p < 0.001), but the difference disappeared in the RCT-only analysis (OR = 1.00, 95% CI: 0.30–3.33, p > 0.99) (Fig. 6a–c). The risk of bias for RCTs is shown in Figure 7a and b, whereas the quality of the other studies is shown (in stars) in Table 2.
Discussion
RC is a morbid procedure associated with substantial complication rates. Robotic surgeries increased with a rate of 10% (from 0.6% to 12.8%) in the last decade 67 mainly because surgeons were aiming for the theoretical impact of this new minimally invasive technology on complication rates. Nevertheless, the advantage in terms of peri- and postoperative outcomes of this minimally invasive procedure has remained theoretical since many studies have failed to prove so, whereas findings of the majority of SRs and meta-analyses published so far in the literature are contradictory. Our SR of 54 studies involving 29,720 patients resulted in the largest meta-analysis currently published in the literature and the only one that analyzes separately all 5 available RCTs and all available observational studies, updating existing knowledge and providing the best level of evidence so far.
The primary outcome for majority of the published data regarding comparison of open and robotic cystectomy is complication rates. 68 –76 Due to the fact that RC is a procedure with relatively high minor complication rates and also some of them present late in the postoperative course, we conducted a separate analysis for minor and major complication rates and a subanalysis of 30 and 90 days. Literature seems to provide controversial data regarding this important aspect of the procedure. Some studies report favorable overall complication rates for RARC, 70,71 whereas others declare decreased major complications for both 30 and 90 days for RARC. 69,71 On the other hand, there are authors who failed to prove any difference between the two techniques in terms of minor complication rates, but this is not the case for major ones. 68,75,76 Nevertheless, our updated results revealed a more favorable profile for RARC in terms of minor complications in 30 and 90 days and major complications in 90 days, but these results did not sustain in the subgroup analysis of RCTs only. A higher level of evidence is usually extracted by well-designed, randomized control studies, and in this case, all available data 60 –64 seem to agree with our subgroup findings that do not award the robotic procedure any advantage in terms of complication rates when compared with its open counterpart. In our point of view, this contradiction between the meta-analysis of observational studies and RCTs is extremely helpful and important and our study is the first one to include them both. The advantages of good observational studies (the included studies in our analysis were awarded seven stars and above), which include increased number of patients, increased external validity, large number of different centers, and real-life conditions, are not to be disregarded. 77
Secondary outcomes of our analysis consisted of LOS, time to regular diet, mortality rates, EBL, transfusion rates, and readmission rates. RARC is a minimally invasive procedure and so most of the studies agree with our finding of more favorable outcomes in terms of EBL and transfusion rates. 68,70,72,75,76 As expected, the robotic procedure performed well in RCTs also 60 –64 and this performance was maintained in our RCT-only subgroup analysis. It is important though to stress the fact that only two RCTs provided data about transfusion rates, a fact that made subgroup analysis impossible. Nevertheless, this advantage did not seem to influence LOS that was found to be equal for both approaches in most of the published data. 71,73,74 Again, our study resulted in a discrepancy between the outcomes of the analysis of observational studies and the one of RCTs. The first yielded favorable results for the RARC procedure in terms of LOS time, time to regular diet, and mortality rate, whereas the latter found no difference between the two techniques. The number of RCTs included in the secondary outcome analysis is small as is the number of involved patients since most of them did not report most of these outcomes. This may have influenced the results of the RCT-only meta-analysis.
Our meta-analysis has also some limitations. Even though we included all the available data in the literature and all the available RCTs, none of the latter were blinded, which can affect their bias. Second, we did not perform the subanalysis of RCTs only for 30 and 90 days, which could potentially alter our conclusions since the first postoperative month is of paramount importance for this kind of operation. This was mainly due to the fact that the number of patients involved in these studies was relatively small and some of them did not even report outcomes in 30 and 90 days. Another potential limitation is that a minority of the included studies are relatively old (2006–2007) and this could mean that patient recruitment could have been even older. This fact along with the little experience in a relatively new technology (in 2003–2006) could have potentially influenced our results. Nevertheless, there is only one article that includes patients undergoing surgeries before 2003 and its relatively small number of patients probably produces a minor influence in the final outcomes of our meta-analysis. Finally, since RC is a procedure that can potentially exhibit complications many months after the procedure, a long follow-up is required to extract safe results, but unfortunately most of the studies do not report extended follow-up of their patients.
Conclusions
Our analysis reinforces the minimally invasive nature of the robotic procedure and its advantages. In clinical practice, it provides minimal bleeding, especially when requiring blood transfusion, and yields improved outcomes in most of the perioperative and postoperative outcomes, even though randomized control trials do not support these results. Robotic RC is an efficient and safe procedure that can provide an alternative to the open procedure with an equal if not better safety profile.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.