
Abstract
Objective:
To define current trends in the utilization of renal thermal ablation by urologists in the United States.
Material and Methods:
A six-month case log data for renal procedures submitted by certifying and recertifying American urologists from 2003 to 2018 were obtained from the American Board of Urology and stratified by current procedural terminology code. The utilization of thermal ablative techniques was examined with respect to overall trends, surgeon, and practice characteristics associated with its use.
Results:
Six thousand two hundred eleven unique urologists performed 54,075 renal procedures, including 1916 (3.5%) thermal ablations, 630 (1.2%) renal biopsies, 17,361 (32.1%) partial nephrectomies, 20,403 (37.8%) radical nephrectomies, and 7957 (14.7%) nephroureterectomies. Eight hundred twenty-five (13.3%) unique urologists performed renal ablations, including 1344 (70.2%), 418 (21.8%), and 154 (8.0%) laparoscopic, percutaneous, and open ablation procedures, respectively. The annual volume of ablation was highest in 2008, followed by 2010 and 2009. On multivariate modeling of those performing renal interventions, the first decade of practice, self-declared endourologist, urologist who completed an endourology fellowship, urologist who practices in the Mid Atlantic, North Central, South Central, and South Eastern United States (compared with New England) were more likely to perform thermal ablation for renal masses. Urologists who perform renal biopsies and partial nephrectomies are also more likely to perform ablation of renal masses.
Conclusions:
Thermal ablation accounted for a small percentage of renal interventions performed by urologists in the last 1.5 decades with definable associations to practice characteristics. Renal ablation was most commonly performed laparoscopically, with declining use in recent years.
Introduction
In the last two decades, the increased use of cross-sectional abdominal imaging has led to a progressive increase in newly detected renal tumors with a corresponding migration to lower-stage disease at diagnosis. 1,2 In addition, the cardiovascular benefits and oncologic noninferiority of partial nephrectomy has become firmly established gradually making it the preferred surgical approach when technically feasible. 3
More recently, there has been increased academic and clinical interest in the use of minimally invasive ablative modalities in the management of small renal tumors, particularly in older and nonsurgical candidates. Recent data suggest a modest but progressive increase in the use of thermal ablation for small renal masses. 3 Traditionally, laparoscopic and open ablations have been performed by urologists while the percutaneous approach has been the domain of interventional radiologists. 4
To date, there has been no assessment of surgeon and practice characteristics associated with the use of renal thermal ablative techniques by urologists in the United States. We reviewed certifying case logs from the American Board of Urology (ABU) to define urologist-level trends and identify physician factors that impact the choice of renal interventions.
Materials and Methods
Study population and design
The ABU is the governing body of urology in the United States and serves to ensure high-quality practice by maintaining standards of certification. To become board certified, candidates must complete an approved residency training program or its equivalent, pass written and oral examinations, and provide 6-month case log data of independent practice. 5 To maintain certification, practicing urologists must demonstrate continued competence and reasonable practices through knowledge examinations and a 6-month case log submission once every 10 years. 6
After Institutional Review Board exemption, the ABU database was queried for the current procedural terminology (CPT) codes (Appendix Table A1) from 2003 to 2018. Patients from 2018 were excluded and given complete data for the year were not available. It is worth noting that the most common thermal modalities of cryoablation and radiofrequency are variably reflected in the CPT code terminology, thus the technique, rather than the ablative modality, was the focus of the analysis. Patient, tumor characteristics, and outcome data were not reported to the ABU, hence were unknown in this dataset. Case logs received from the ABU were reported in 6-month periods representing individual surgeon practice volume.
Variables
Variables obtained from the ABU were CPT codes (Appendix Table A1), surgeon's age (years), log date (mm/dd/yyyy), log year (2003–2017), number of defined procedures performed, cycle (first certification attempt, first time in maintenance of certification [MOC] level 4, third time in MOC level 4, first time in recertification, second time in recertification, third time in recertification, etc), surgeon gender (male/female), self-reported surgeon specialty (oncology, endourology, urolithiasis, female, andrology, infertility, pediatric, general, unknown), region (Mid Atlantic, New England, North Central, North Eastern, South Central, South Eastern, Western, International), surrounding population of urological practice (<100 k, 100–250 k, 250–500 k, 500 k–1 million, >1 million), practice type (different iterations of private practice, academic, part-time academic), fellowship organization and fellowship type (different iterations of oncology, endourology, andrology, female urology, pediatric urology, minimally invasive surgery, and infertility).
Surgeon's year in practice was calculated from cycle data. Surgeons were classified as “no renal ablation” if they did not perform at least one ablation procedure through any approach. Surgeon age was aggregated by mean for each unique surgeon identifier. For practice location, practice population of the greater area of practice and practice type, the most recent record was used for urologists certifying more than once in the 15-year period.
Statistical analyses
R 3.5.1 for RStudio 1.1.456 was used for statistical analyses. Medians and their interquartile range were used to summarize continuous variables, whereas categorical variables were summarized with counts and percentages. Associations among surgeon characteristics and the use of a renal ablation approach were assessed using a chi-square test, Fisher's exact test, Student t-test, and logistic regression where appropriate. Exploratory multivariate logistic regression was used to assess potential predictors of ablative modality use, and all patient factors that were statistically significant on univariate analysis was included into the multivariate model. Only renal ablation was analyzed given no tumor, and patient outcome information was available in the ABU dataset and indications for radical and partial nephrectomy are logically based of tumor and patient characteristics. For all statistical analyses, p < 0.05 was considered statistically significant.
Results
Six thousand two hundred eleven unique urologists performed 54,075 renal procedures, including 1916 (3.5%) thermal ablations, 630 (1.2%) renal biopsies, 17,361 (32.1%) partial nephrectomies, 20,403 (37.8%) radical nephrectomies, and 7957 (14.7%) nephroureterectomies. Eight hundred twenty-five (13.3%) urologists performed renal ablations, including 1344 (70.2%), 418 (21.8%), and 154 (8.0%) laparoscopic, percutaneous, and open procedures, respectively. Annual case volumes across the study period are reflected in Figure 1 and the annual volume of ablation was highest in 2008, followed by 2010 and 2009. Over the course of 15 years, the total number of partial nephrectomy cases gradually increased from 14.6% in 2003 to 41.4% in 2017. Similarly, the number of radical nephrectomy cases decreased from 84% in 2003 to 55.8% in 2017 (Fig. 2). Surgeons who perform renal ablation perform a median of 24 renal ablations within 6 months (1st quartile: 12, 3rd quartile: 48). A total of 611 of 825 (74.1%) performed 5 of fewer renal ablations within 6 months.
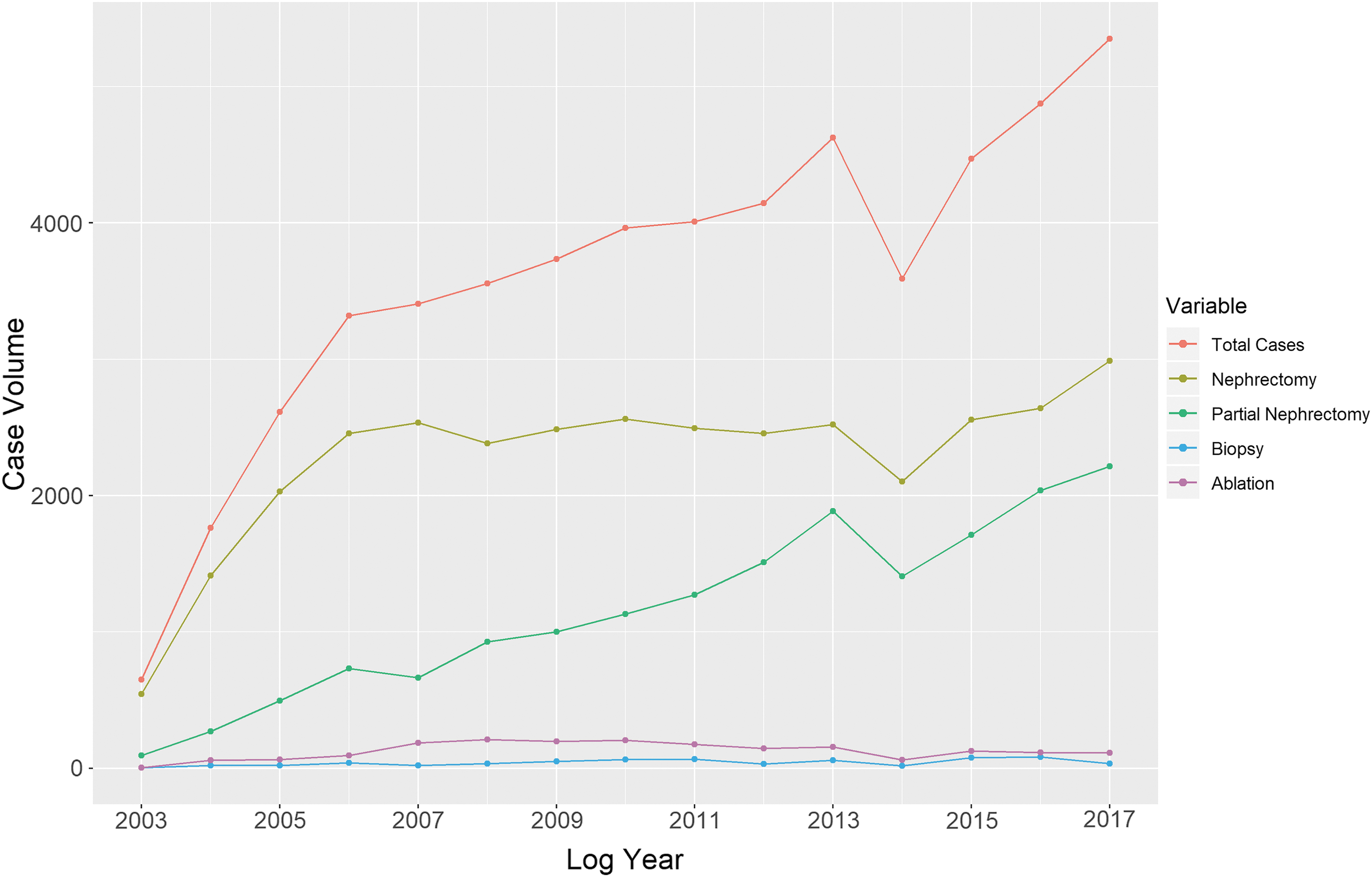
Total annual renal interventions performed by certifying and recertifying American urologists.
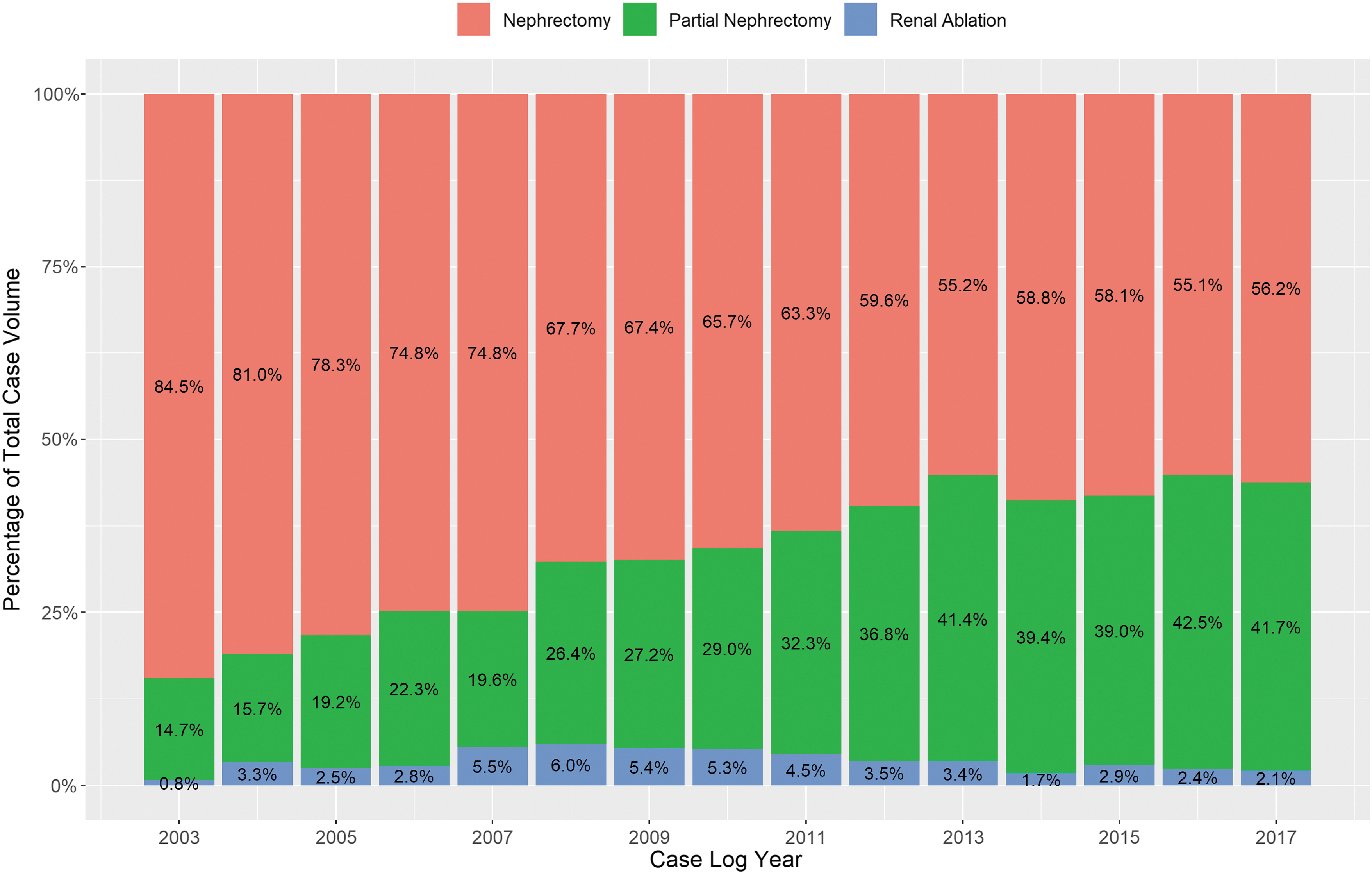
Percentage of renal interventions performed by certifying and recertifying American urologists.
Surgeon and practice characteristics associated with the use of renal thermal ablation (compared with those performing partial, radical nephrectomy, and nephroureterectomy) are defined in Table 1. On univariate analysis, gender, surgeon age, case log submission year, years in practice, region, practice pattern, self-declared specialty, fellowship, surgeons performing renal biopsies, and surgeons performing partial nephrectomies impacted the use of ablation.
Surgeon and Practice Characteristics Associated with Ablation of Renal Masses
Statistical significances. Total percentages may exceed 100% given values were rounded to the nearest decibel.
IQR = interquartile range.
The overall effects and odds ratios from logistic modeling predicting the log odds of using ablation are reflected in Table 2. On multivariate modeling of those performing renal interventions, the first decade of practice ([11–20 years—odds ratio [OR]: 0.6, 95% confidence interval [95% CI]: 0.46–0.78], [21–30 years—OR: 0.57, 95% CI: 0.32–0.98]), self-declared endourologist (OR: 2.81, 95% CI: 1.89–4.13), urologist who completed an endourology fellowship (OR: 1.78, 95% CI: 1.14–2.77), urologist who practices in the Mid Atlantic (OR: 1.72, 95% CI: 1.21–2.46), North Central (OR: 1.64, 95% CI: 1.19–2.26), South Central (OR: 1.81, 95% CI: 1.29–2.53), and South Eastern United States (OR: 1.65, 95% CI: 1.22–2.25) compared with New England is associated with an increased use of thermal ablation for the treatment of renal masses. Urologists who perform renal biopsies (OR: 10.7, 95% CI: 8.25–14.05) and partial nephrectomies (OR: 1.78, 95% CI: 1.50–2.12) are also more likely to offer ablation of renal masses.
Multivariate Logistic Regression Model of Characteristics Associated with Renal Ablation
Statistical significance.
CI = confidence interval; OR = odds ratio.
Appendix Table A2 depicts characteristics associated with a laparoscopic (vs perc/open) ablative approach. On univariate analysis, urologists who submitted case logs earlier in the cohort and urologists who are 1–10 years in practice were more likely to perform laparoscopic ablation of renal masses. On multivariate logistic modeling (Appendix Table A3), every increase in case log submission year between 2003 and 2017 was associated with a lower likelihood of performing laparoscopic renal ablation (OR: 0.85, 95% CI: 0.81–0.89). Physicians who are 11–20 (OR: 0.60, 95% CI: 0.46–0.78) and >30 years (OR: 0.14, 95% CI: 0.06–0.32) from training were also associated with a lower likelihood of performing laparoscopic ablation of renal masses when compared with physicians 1–10 years from training.
Discussion
The impact of nephron loss during the treatment of renal tumors that occasionally results in end-stage renal disease has made renal preservation a critical objective during the recent management of kidney tumors. 7 Partial nephrectomy is now broadly recommended for renal masses ≤4 cm (cT1a) with some guidelines extending this to tumors ≤7 cm (cT1b) when technically feasible. 8 In the last decade, there has been growing interest in the use of thermal ablative techniques as an alternative to partial nephrectomy, particularly in patients with higher surgical risk due to advanced age or medical comorbidities. 9,10 In this article, we aimed to define current trends in the utilization of renal thermal ablation by urologists in the United States. We show that thermal ablation accounted for a small percentage of renal interventions performed by urologists in the last 1.5 decades with definable associations to practice characteristics.
On top of that, this study highlights several important findings. First, the results define the use of the three major renal interventions, including thermal ablation, partial nephrectomy, and radical nephrectomy, performed by certifying and recertifying urologists across the last 1.5 decades. The total number of renal procedures increased progressively, driven primarily by an increase in the use of partial nephrectomy. The relative use of urologist-performed thermal ablation peaked in 2008 comprising 6.0% of renal cases, followed by a decline in the latter decade of the study and renal ablation only accounted for 2.1% of cases in 2017. A similar trend was observed in the analysis of unique urologists who performed thermal ablations. In 2009, 21.6% of certifying and recertifying urologists performed at least one thermal ablation but this declined to 13.2% by 2017. Table 2 shows that renal ablations are performed predominantly by general urologist and endourology trained urologist in private practice. Other factors include urologist in the first decade of practice, those certifying earlier in the study decade and who are practicing in the Mid Atlantic, North Central, South Central, and South Eastern region of the United States.
Second, this study demonstrates the overall and temporal trends in the use of the various thermal approaches by urologists, including laparoscopic, percutaneous, and open techniques. Thermal ablation was performed primarily by the laparoscopic approach that comprised 70.2% (1344/1916) of cases during the study period. The use of laparoscopic ablation peaked between 2007 and 2009 of the study periods followed by a progressive decline, and was the primary determinant of the overall decrease in the use of thermal ablation by urologists during the overall study period. We hypothesize that the marked decreasing use of laparoscopic ablation by urologists may be explained by conversion of these cases to nonablative management, including active surveillance when appropriate or more commonly minimally invasive partial nephrectomy. A growing body of contemporary literature emphasizes the decreased perioperative morbidity associated with robotic partial nephrectomy, but it is not yet known if patients who were considered nonsurgical candidates and offered ablation in the era of open partial nephrectomy, are now undergoing minimally invasive partial nephrectomy. 11,12 In addition to a shift from laparoscopic ablation to robotic partial nephrectomy, another plausible explanation of decreasing laparoscopic ablations is increased performance of the percutaneous approach, predominantly by interventional radiologists. 9,13
Third, our findings offer insights into the practices of urologists performing renal thermal ablations. Many urologists performing ablation also performed renal biopsies (OR: 10.7, 95% CI: 8.25–14.05) and partial nephrectomies (OR: 1.78, 95% CI: 1.50–2.12). Data also define a cohort of 214/825 (25.9%) high-volume ablationists who performed five or more ablations accounting for the top decile by case volume for the 6-month log period. Higher surgeon volume is associated with better outcomes for partial nephrectomy and it is worth considering whether this relationship is also true for thermal ablation. 14
Several important limitations must be recognized. First, we have examined surgical case logs independent of preoperative disease and patient factors. Thus, we cannot draw conclusions regarding how particular interventions were selected. Second, data highlight urologist procedural patterns rather than overall management strategies for renal masses. We cannot conclude whether the observed decrease in urologist-performed ablation is due to a waning faith in this modality, a shift toward other options such as robotic partial nephrectomy or rather due to increased referrals to interventional radiology. We also could not account for the possible volume of referrals to other specialists. Third, case logs do not account for procedures performed together with other specialists. It is likely that many percutaneous ablations performed by urologists may be done collaboratively with interventional radiologists. Fourth, data do not completely account for type of ablation modality (cryoablation, radiofrequency, etc) used. Also, the case logs are from a self-defined 6-month period and may not truly represent the most accurate surgical volume of each urologist. Specialty designation was also self-reported by the urologist and may not be representative of fellowship training. Missing fellowship information and not having done a fellowship could not be differentiated based on the dataset. Urologists who certified before 1985 are not required to recertify, hence, will not have case logs included in the ABU dataset, thus the data would be skewed toward younger urologists' practices. Cases include both benign and malignant disease, and adult patients given that no patient characteristics were provided.
Despite these limitations, we believe data offer critical and unique insights into surgeon and practice characteristics associated with the use renal thermal ablation. We believe that these data are one of the largest databases of management of renal masses representing the contemporary experience of urologists from all geographic locations and practice types in the United States. These results are important because it shows that the overall number of renal ablations being performed by urologists is declining, indicating that most current and future trainees may have less experience with renal ablation and this procedure may eventually be the domain of interventional radiology.
Conclusions
Thermal ablation accounted for a small percentage of renal interventions performed by urologists in the last 1.5 decades with definable associations with practice characteristics. Ablation was most commonly performed laparoscopically, with declining use in recent years. Further understanding of renal thermal ablation practice patterns may improve its use in clinical practice.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
W.P.T. is supported by the Ruth L. Kirschstein NRSA Institutional Research Training Grant (T32 CA093245).
Abbreviations Used
Appendix
Multivariate Logistic Regression Model of Characteristics Associated with Renal Open/Perc Ablation vs Laparoscopic Ablation
| OR | 95% CI | p | |
|---|---|---|---|
| Case log submission year | 0.85 | 0.81–8.9 | <0.001 |
| Years in practice | |||
| 0–10 | — | — | — |
| 11–20 | 0.60 | 0.46–0.78 | 0.001 a |
| 21–30 | 0.57 | 0.32–0.98 | 0.259 |
| >30 | 0.14 | 0.06–0.32 | <0.001 a |
Statistical significance.
CI = confidence interval; OR = odds ratio.