
Abstract
Purpose:
Robot-assisted partial nephrectomy (RAPN) is increasingly applied to renal hilar tumors. The present study aims to introduce our vessel and tension-free reconstruction technique and discuss the perioperative, functional, and midterm oncologic outcomes of RAPN for hilar tumors in a large cohort.
Materials and Methods:
We retrospectively reviewed clinical data of 286 consecutive patients with hilar tumors who underwent RAPN from June 2013 to December 2016 in our center. Our anatomy-based “Garland” technique specialized in protecting the large hilar vessels and minimizing the tension of suturing the defect via trans/retroperitoneal approaches for anterior/posterior lip hilar tumors, respectively.
Results:
“Garland” technique was effectively applied in 286 patients, and the warm ischemia time was 18.2 ± 4.1 minutes. Median estimated blood loss for RAPN was 100 mL (interquartile range [IQR]: 50–200 mL). Median operative time was 120 minutes (IQR: 90–150 minutes). No patient was converted to open surgery. Postoperative stay was 4.0 days (IQR: 4.0–5.0 days). Three patients (1.1%) had positive surgical margin. Two patients (0.7%) received blood transfusion. Complications occurred in 20 patients (7.0%), in which 18 patients were Clavien 1 and 2. Three patients (1.1%) had local recurrence. All patients were alive at a 48-month median follow-up (range: 24–66 months).
Conclusions:
“Garland” technique is safe and feasible for hilar tumor resection and kidney reconstruction. The trans/retroperitoneal approaches are options for anterior/posterior hilar tumors. Longer follow-up involving more patients is required.
Introduction
Partial nephrectomy (PN) has a comparative advantage in oncologic and quality-of-life outcomes for clinical T1 tumors over radical nephrectomy (RN), irrespective of the surgical approach and the tumor size. 1 Compared with open PN, robot-assisted partial nephrectomy (RAPN) provides similar long-term oncologic outcomes, with decreased blood loss and quick recovery for localized tumors. 2
Hilar tumors were first described by Gill and colleagues and now defined as renal masses located in the region of renal hilum and physically contacted with renal artery and/or vein. 3 This particular location is challenging due to the adjacency to renal vessels and collecting system. With accumulated experiences and technical advances, multiple studies have reported that laparoscopic PN or RAPN is effective and safe for hilar tumors with excellent perioperative and oncologic outcomes. 3,4 Furthermore, several articles depicted the detailed steps of tumor resection and kidney reconstrunction. 5 –7 However, a lack of understanding of the anatomy of renal hilum may mislead the surgical procedures and cause adverse outcomes. Our primary objective was to describe a renal sinus anatomy-based novel technique and its perioperative and postoperative oncologic and surgical outcomes in patients undergoing RAPN for hilar tumors.
Materials and Methods
Study population
The local ethics committee approved the data collection and assessment. Individual informed consent was obtained from all patients. Preoperative CT or MRI was used to obtain tumor parameters, including tumor location, tumor size, and tumor complexity according to the radius, exophytic or endophytic, nearness to renal sinus or collecting system, anterior/posterior, polar (R.E.N.A.L.) nephrometry score raised by Kutikov and colleagues. 8 Scores were given by two separate radiologists. An associate chief physician rechecked if the results were controversial. We retrospectively reviewed 286 patients with hilar tumors who underwent RAPN with complete imaging data between June 2013 and December 2016 in our single center. Baseline demographic variables that included age, gender, body mass index (BMI), R.E.N.A.L. score, American Society of Anesthesiologists score, Charlson comorbidity index, or tumor size were collected. The postoperative complication outcomes were assessed according to the Clavien–Dindo classification. 9 The Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation was used to calculate the estimated glomerular filtration rate (eGFR).
Preoperative assessment and surgical indication
Multifocal tumors, those with off-clamp PN, or cold ischemia hilar tumors were excluded. A total of 286 patients were enrolled into the study either transperitoneally or retroperitoneally. Three experienced surgeons performed all the cases.
Surgical technique
Approach selection, patient positioning, and port placement
For right-side anterior lip tumors
For right-side anterior lip tumors, patients were positioned in a modified left lateral decubitus position via the transperitoneal approach. A 12-mm port was placed at about 2 to 3 cm to the upper right of the umbilicus for the camera. Three 8-mm robotic ports for the first, second, and third robot arm were placed at about 3 cm medial to the right midclavicular line under the costal margin, at about 3 cm lateral to the right midclavicular line near McBurney's point, and at 6 to 8 cm lateral to the second arm, respectively. Two assistant ports were used. A 12-mm assistant port is placed medially between the camera and first robotic port in the midline for the aspirator. A 5-mm port is placed below the xiphoid for the retraction of liver (Fig. 1A–C). 10
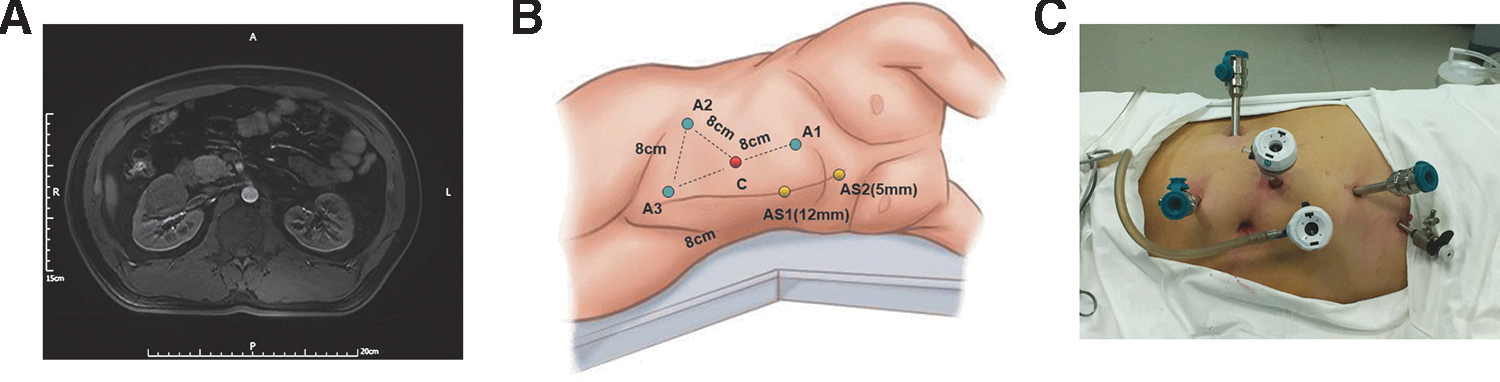
MRI, patient positioning, and port placement for anterior lip tumor.
For the posterior lip tumors
For the posterior lip tumors, the retroperitoneal approach was adopted. Patients were placed in a full flank decubitus position with the ipsilateral side up relative to the renal tumor. One to 2 cm above the iliac crest in the midaxillary line for the 12-mm camera trocar, and the two 8 mm trocars were placed at the intersection of the posterior axillary line and the middle line of the costal margin and iliac crest. Last, the assistant 12-mm trocar is in the middle line of camera trocar and the anterior 8-mm trocar above the anterior superior spine. The trocar configuration for the retroperitoneal approach is illustrated in Figure 2A–C.
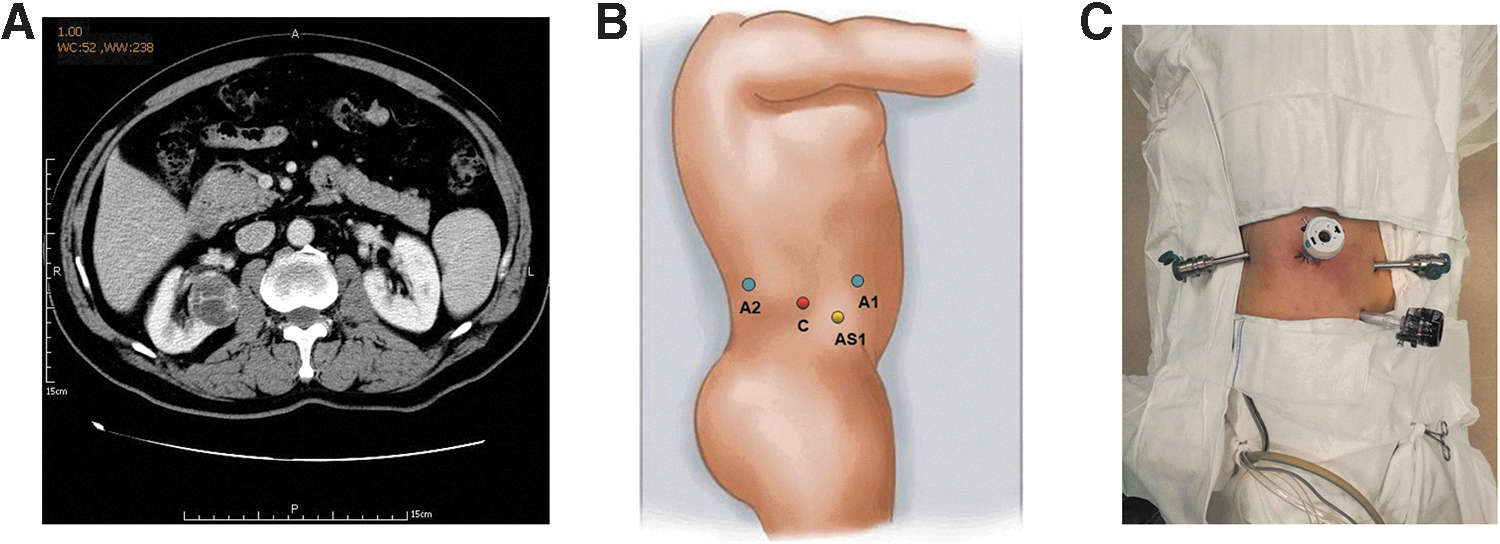
MRI, patient positioning, and port placement for posterior lip tumor.
Renal sinus anatomy-based hilar tumor dissection
Since hilar tumor is close to large vessels, the exposure of the tumor boundary is imperative at the initial stage. Renal sinus fat is anatomically surrounded by a layer of membrane that covers the renal capsule and the large vessels. As Figure 3 and Supplementary Video S1 show, after the membrane and the related loose connective tissue were carefully incised, the vessel-free plane between the renal mass capsule and the large renal vessels (artery and vein) can be well exposed (Fig. 3A, B). The third robotic arm of prograsp forceps was applied to hold the tumor with tension to expose the boundary of tumor prior the tumor dissection. Starting dissection from the lateral side of the tumor is required for the small possibility of causing vascular injury. If possible, enucleate the tumor along the pseudocapsule so as to save more nephrons and decrease the defect to the utmost limit. As for tumors without pseudocapsule or endophytic type, intraoperative ultrasonography is usually used, and an extended dissection range is required to guarantee a negative surgical margin.
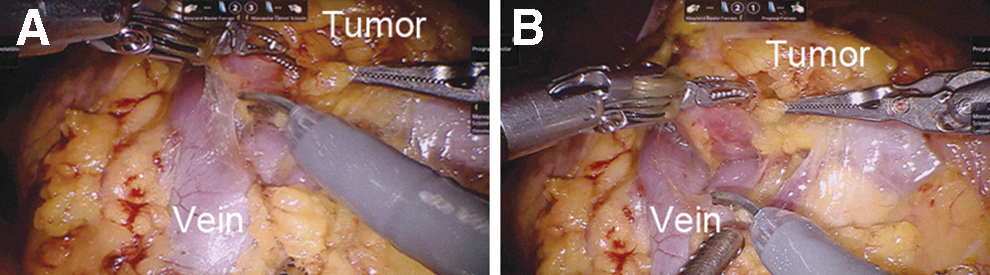
The vessel-free plane between the renal mass capsule and the large renal vein.
Vessel and tension-free reconstruction technique
After the tumor dissection is completed, 0-QUILL is used in suturing the defect. The challenge is to avoid the “cheese-cutting” effect in extensive wound closure and large vessel injury, based on which we developed a novel “Garland” technique that signifies vessel and tension-free reconstruction. The all-layer flow suture using barbed thread (0-QUILL) was applied retrogradely starting from the hilum to parenchyma; each suture is adhered to the surface of large vessels and is fixed by clips on the renal capsule, and finally, the garland shape of the closed wound was formed (Fig. 4). With the above key notes, most of the nephron-sparing surgery for hilar tumors can be effectively executed.
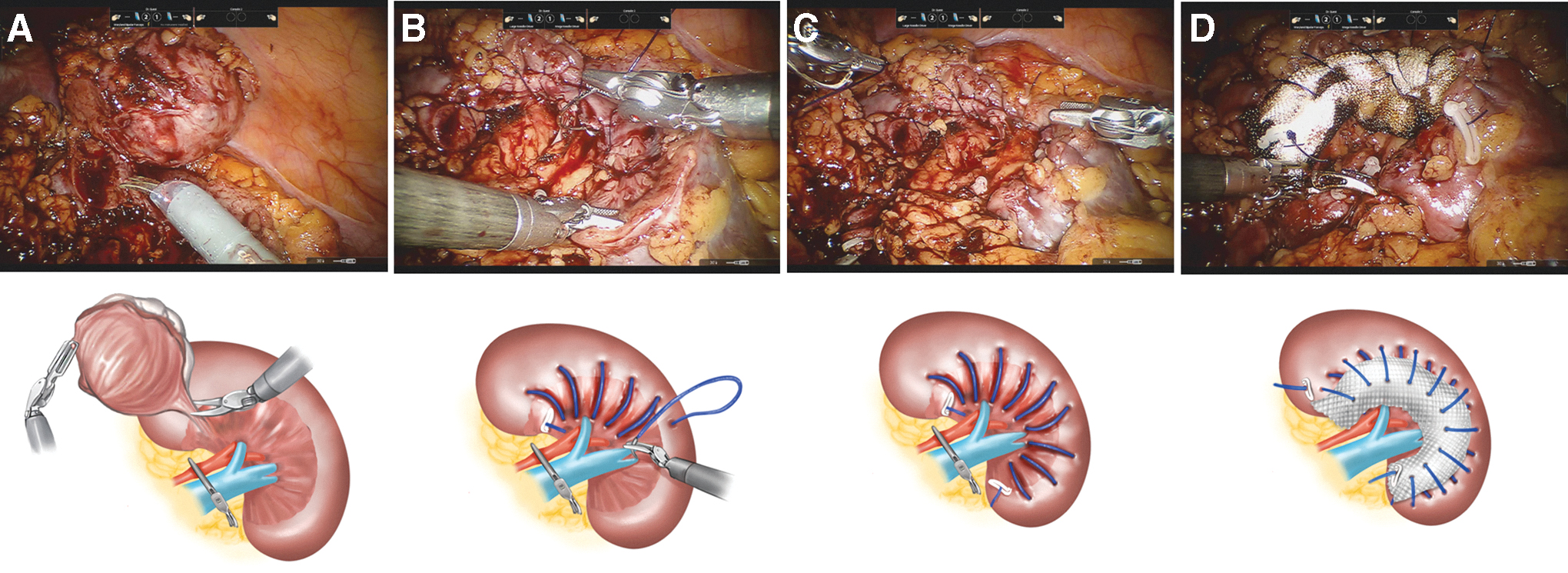
Sketch map for anterior tumor dissection and vessel and tension-free technique.
As the number of cases is increasing, the suturing differentiation of the anterior lip tumor and posterior lip tumor was observed due to the anatomically different adjacent vessels. The anterior lip tumor location is adjacent to the renal vein and its tributaries, while the posterior lip tumor is near the renal artery and its branches (Fig. 5A, B). For transperitoneally closing the anterior wound, the absorbable hemostat is necessary in compressing the tiny defects of renal venous tributaries, while the posterior lip wound closure is optional (Supplementary Table S1).
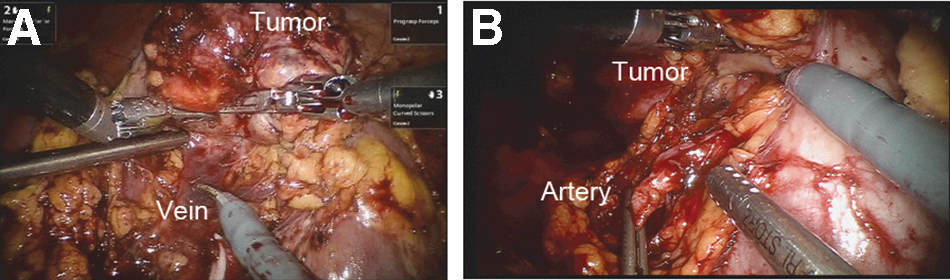
The different adjacent large renal vessels for anterior/posterior lip hilar tumor.
Statistical analyses
Data are given as mean and standard deviation (SD) and median (interquartile range [IQR] or range) or percentage for continuous and categorical variables, respectively. Independent t test or Mann–Whitney U test for continuous data and chi-square or Fisher exact test for categorical data were used. Statistical analyses were performed using SPSS v.19.0 (IBM Corp., Armonk, NY).
Results
Patient and tumor characteristics are summarized in Table 1. The mean age was 56.2 years (SD: 9.2) and the mean BMI was 26.8 kg/m2 (SD: 3.5). The clear cell type was the majority of all cases (91.5%). Mean R.E.N.A.L. nephrometry score was 8.2, and the median tumor size was 2.6 cm. Perioperative outcomes are shown in Table 2. Median operative time was 120 minutes (IQR: 90–150), and median estimated blood loss (EBL) was 100 mL (IQR: 50–200). The mean warm ischemia time (WIT) was 18.2 minutes. Posthospital stay was 4.0 days (IQR: 4.0–5.0 days). No patient was converted to open surgery. There were two transfusion cases and two converted to RN (0.7%), respectively. For the conversion cases, one was observed for multiple tumors intraoperatively, and the other was for uncontrolled bleeding of the renal parenchyma. Positive surgical margin (PSM) was found in three subjects (1.1%) sharing the common characteristic of a relatively large tumor size (>5 cm). Complications after surgery were recorded. Complications of Clavien 1 and 2 occurred in 18 patients. The preoperative eGFR was 84.5 ± 19.6 mL/minute, postoperative day 1 eGFR was 72.6 ± 22.9 mL/minute, and the 6-month postoperative eGFR was 83.2 ± 21.1 mL/minute (Table 3). The eGFR was obtained immediately before surgery, and the last available value was used to calculate the change in renal function. With a median follow-up of 48 months, no metastasis was noted and three patients (1.1%) had local recurrence. All patients were alive at follow-up (range: 24–66 months).
Demographic and Tumor Characteristics
ASA = American Society of Anesthesiologists; BMI = body mass index; CCI = Charlson comorbidity index; R.E.N.A.L. = radius, exophytic or endophytic, nearness to renal sinus or collecting system, anterior/posterior, polar; SD = standard deviation.
Perioperative Outcomes
EBL = estimated blood loss; IQR = interquartile range; SD = standard deviation.
Functional and Oncologic Outcomes
eGFR = estimated glomerular filtration rate.
Discussion
Nephron-sparing surgery is currently considered the gold standard for the treatment of clinically T1 renal masses when technically feasibly. 11 The oncologic efficacy for PN is comparable with RN while the risk of chronic kidney disease is significantly reduced. 2
Complete oncologic control, as well as protection of the major vessels and collecting system, is the core consideration in our procedures. With the advantage of surgical technology, the number of RAPN of renal hilar tumors increased. 12,13
The resolution in extensive wound closure is another challenging issue. A conventional manner for antegrade dissection and defect folding suture with tension for peripheric renal tumors is not suitable for renal hilar tumors. 14 In addition, certain literature reported the sutureless technique of PN, but only indicated for low nephrometry score masses. 15,16
Inspired from the surgical treatment for complex stone disease, herein we developed a novel technique based on the anatomy of renal hilum. 17 First, we mobilized the kidney and tumor, renal sinus exposure is the substantial key step, and sinus fat is surrounding the renal hilum. 18 As is known, the renal sinus space is anatomically surrounded by a membranous structure that covers the renal capsule and the large vessels. The vessel-free plane between the renal mass capsule and the large renal vessels (artery and vein) can be well revealed after the membrane dissection. “To see and then protect,” it is commonly known that most malignant renal tumors have the pseudocapsule, which is helpful for the dissection of tumors with a negative margin. The space between the major renal vessels and tumor boundary can be found as the initial dissected plane after mobilizing the sinus fat.
The core issues of PN for hilar tumors are the manner of dissection of tumors and suture of renal defects. The visible venous defect can be repaired by Proline stitch for renal vessels and stitch anastomosis applied for renal collection system rupture, respectively. The tension in suturing the extensive wound is a concern due to the potential risk of the “cheese-cutting” strength. 19 Sliding Hem-o-lok and “V” hilar sutures were introduced to close the renal defect, 5,6 and we executed a novel “Garland” technique that signifies the vessel and tension-free reconstruction. Continuous barbed thread all-layer suturing was performed in a retrograde direction starting from the hilum to parenchyma, and finally, the garland shape of the closed wound was formed. For the second-layer suture, the absorbable hemostat gauze was optional for compression of the tiny venous tributaries' bleeding. For anterior lip tumor, this step is necessary due to the thin vascular wall of adjacent veins and the tributaries and certain invisible tiny defects, while for the posterior lip tumor, this step is optional because the vascular walls of the artery and its branches are relatively thick. As for the complex anatomical variation, venous tributaries sometimes are intercross enwinded with the renal artery, and so, a compression step is needed for posterior lip hilar tumor control.
By applying the “Garland” technique, we have effectively performed RAPN since the year 2013 for hilar tumors with a mean R.E.N.A.L. nephrometry score of 8.2 and median tumor size of 2.6 cm. We achieved good median operative time, EBL, and WIT. There were two transfusion cases and another two converted to RN (0.7%), respectively. For the conversion cases, one was for multiple tumors intraoperatively, the other was for uncontrolled bleeding of the renal parenchyma. PSM was found in three patients with a relatively large tumor size (>5 cm), which aroused our attention in the patient selection criterion for PN. Some of the T1 renal hilar tumors might not be feasible for PN, including the diameters larger than 5 cm, irregular tumor margin, discontinuous pseudocapsule, and hematuria.
Careful consideration for indication of PN is needed when encountering tumor with these features. Although our postoperative and oncologic results were good, we have to make the statement that the surgeons are experienced in a high-volume center for renal cancer, they have effectively completed hundreds of minimally invasive complex PN before, and the understanding of the renal sinus anatomy is essential. The limitation of this study is that it is a retrospective single-center research. CKD-EPI was used to estimate the GFR instead of iodine 131, the standard direct GFR measurement.
Conclusions
Our anatomy-based “Garland” technique (vessel and tension-free reconstruction technique) is safe and feasible. To maximize safety and efficacy of PN, a thorough understanding of the renal sinus anatomy and a highly experienced team are essential. Different tumor locations require different approaches. The “Garland” technique can be a valid alternative for hilar tumors.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was financially supported by the People's Republic of China and the National High Technology Research and Development Program (“863” Program) of China (Grant Nos. 2014AA020607 and 2012AA021101).
Supplementary Material
Supplementary Table S1
Supplementary Video S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.