
Abstract
Introduction:
Robotic retroperitoneal lymph node dissection (R-RPLND) is a challenging procedure. We hypothesized that surgical times and operative complications would decrease as surgeons became more facile with R-RPLND.
Materials and Methods:
We retrospectively reviewed 121 consecutive R-RPLNDs performed at Naval Medical Center San Diego and Mayo Clinic Arizona by 4 fellowship trained robotic surgeons between 2008 and 2018. Linear regression was used to analyze independent predictors of setup time, operative time, and lymph node counts. Logistic regression was used to analyze open conversions, overall complications, and high-grade complications. Variables included as independent predictors were: sequential case number, surgeon, clinical stage, chemotherapy status, RPLND template, and body mass index. Univariate and multivariate analyses were conducted. Statistical significance was established at α = 0.05.
Results:
There was no change in setup time with case number (p = 0.317), but differences were noted between surgeons. Operative times decreased with increasing case number (p < 0.001) but were negatively affected by clinical stage III testis cancer (p = 0.029) and history of chemotherapy exposure (p = 0.050). Surgical times are predicted to decrease by 1 hour after 44 cases. Lymph node counts were dependent only on the surgeon. No factors were predictive of open conversions. Fewer overall complications occurred as experience was gained (p = 0.001), but high-grade complications could not be predicted.
Conclusions:
Consistent with the learning curves shown for other technologically advanced surgical techniques, experience appears to improve surgical times and lower complication rates for R-RPLND.
Introduction
Since the da Vinci™ surgical robot (Intuitive Surgical, Sunnyvale, CA) was approved in 2000 by the United States Food and Drug Administration, robotic-assisted laparoscopic procedures have rapidly evolved and continue to reshape the conventional surgical approach. The benefits of this technology and its adoption within urology are well established. 1,2 Retroperitoneal lymph node dissection (RPLND) may represent another opportunity for infusion of robotic technology into patient care.
Robotic-assisted technology was first applied to RPLND in 2006. 3 Since that time, use of this minimally invasive technique has largely been limited to experienced surgeons in high-volume centers; however, retrospective studies comparing the safety of this procedure with its open and laparoscopic alternative have been favorable. 3 –7 In a review article by Schwen and colleagues, primary robotic-retroperitoneal lymph node dissection (R-RPLND) for low-stage non-seminomatous germ cell tumor was reported to have decreased intraoperative blood loss and decreased length of hospital stay compared with the conventional open approach. 8 In addition, both complication rates and short-term oncologic outcomes were comparable.
As robotic surgery expands, there has been greater consideration of the learning curve associated with transition to this new technology. The term “learning curve,” first described by Herman Ebbinghaus in 1885, uses graphical means to display how a piece of knowledge or a skill is obtained through repetition. 9 Performance outcomes typically examined include operative time, estimated blood loss, perioperative complications, and oncologic efficacy such as surgical margin status, lymph node yield (LNY), and recurrence of disease. Overall, studies have demonstrated improvement of these measures with experience; however, there has been significant variation between procedures.
To date, there is no literature examining the learning curve of R-RPLND. We hypothesized that an improvement of surgical time and operative complications would be present as surgeons gained experience with this procedure. The focus of this question was directed at the immediate 30-day perioperative outcomes associated with the learning curve for this procedure, and not at its long-term effects and oncologic outcomes, which are debated elsewhere in the literature.
Materials and Methods
A retrospective review of consecutive R-RPLNDs performed at Naval Medical Center San Diego and Mayo Clinic Arizona by four fellowship trained robotic surgeons between 2008 and 2018 was conducted. The participating surgeons began their experience with R-RPLND after fellowship training. Although each had extensive laparoscopic skills commensurate with their fellowship training, performance of laparoscopic RPLND before adoption of the robotic technique was not common among the group. These data represent their initial experiences with this robotic-assisted laparoscopic procedure. This retrospective review was approved by the Institutional Review Board, including the appropriate data sharing agreement between Naval Medical Center San Diego and Mayo Clinic Arizona. R-RPLND was completed in a manner previously described by Santomauro and colleagues and Cheney and colleagues. 4,10 All cases were performed by using a supine, low-abdominal, transperitoneal approach. Data were collected for patient characteristics, operative details, pathology results, and postoperative course. Descriptive statistics were calculated. Setup time was defined as time between wheels-in-room time and surgical cut time. Surgical time was measured from cut time until completion of wound closure. Complications were graded according to the Clavien-Dindo classification system. 11
Linear regression was used to analyze independent predictors of setup time, operative time, and lymph node counts. Logistic regression was used to analyze open conversions, overall complications, and high-grade complications. Variables included as independent predictors were: sequential case number, surgeon, clinical stage, chemotherapy status, RPLND template, and body mass index (BMI). Univariate and multivariate analyses were conducted. Statistical significance was established at α = 0.05. STATA®12 (College Station, TX) was used for the analysis.
Results
From 2008 to 2018, 121 R-RPLNDs were performed at 2 institutions, Naval Medical Center San Diego (57 cases, 47.1%) and Mayo Clinic Arizona (64 cases, 52.9%). All four surgeons were fellowship trained in programs with a strong emphasis on robotic and other minimally invasive operating techniques. The average age of the patients was 30.3 ± 10.7 years with an average BMI of 26.6 ± 4.3. With reference to clinical stage, 60 out of 121 (49.6%) cases were Stage I at the time of surgery, 30 out of 121 (24.8%) were Stage II, 18 out of 121 (14.9%) were Stage III, and 3 out of 121 (2.5%) were Stage IS. Primary malignancies that were not of testicular origin made up 8.3% (10/121) of the cohort and included three rhabdomyosarcomas, three mesotheliomas, two Leydig cell tumors, one desmoplastic round cell tumor, and one undefined mass. Ninety-nine (81.8%) of the surgeries used a bilateral template whereas the remainder were unilateral (10 right template, 12 left template). Finally, 65 (53.7%) of the cases were primary and 56 (46.3%) were post-chemotherapy. Median (interquartile range) follow-up for the cohort was 26 (3–60) months.
The mean setup time was 68 ± 27 minutes (median 61) with operative times of 341 ± 117 minutes (median 339). There were conversions to an open approach in 5.8% (7/121). Reasons for conversion included: three for brisk bleeding, two for poor exposure, one for robotic malfunction, and one for discovery of a mass encasing the duodenum that required open excision. Two of the bleeds involved the renal artery. Lymph node counts averaged 26 ± 16 (median 24). Median length of stay was 2 days. Complications were encountered in a total of 27.3% (33/121). These included 14.0% (17/121), 8.3% (10/121), 0.8% (1/121), 3.3% (4/121), and 0.8% (1/121) with Clavien I, II, IIIa, IIIb, and IVa, respectively. The IIIa complication was a lymphocele that required percutaneous aspiration. The IIIb complications were for two ureteral injuries that required repair, one nephrectomy due to injury of the right renal artery, and one fasciotomy in a patient who developed compartment syndrome. One patient with a history of prior bleomycin exposure had acute hypoxic respiratory failure (Clavien IVa).
Over the study period, room setup time did not decrease with respect to case sequence number (Table 1). In contrast, operative time decreased significantly on both univariate (p = 0.020) and multivariate analysis (p < 0.001) as surgeons gained experience (Fig. 1). Other factors were found that significantly affected operative time; specifically, prior chemotherapy exposure (p = 0.050) and malignancies of testicular origin with preoperative clinical Stage III (p = 0.029) increased operative time (Table 2). The coefficient (95% confidence interval) for case number (on multivariate analysis) was −1.369 (−1.969 to −0.770), suggesting that after 44 cases, operative times would be reduced by 1 hour. Lymph node counts did not change as surgeon experience grew (p = 0.600) (Table 3).
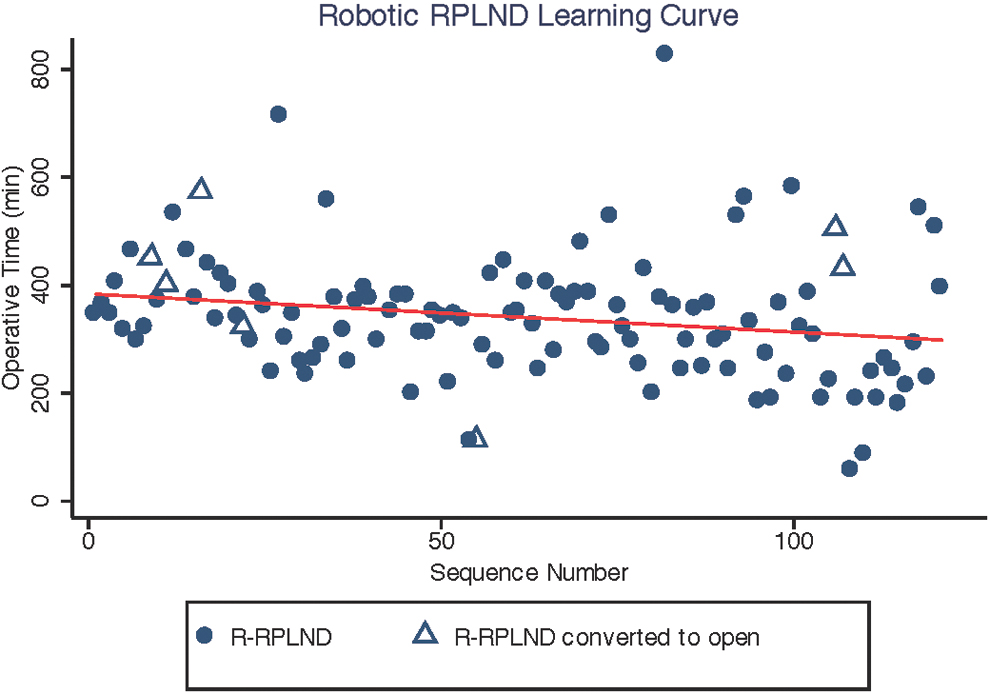
Robotic RPLND learning curve for operative time. A decrease in operative time was seen as more experience was gained. Surgical times are predicted to decrease by 1 hour after 44 cases. RPLND = retroperitoneal lymph node dissection. Color images are available online.
Room Setup Time
Room setup time varied by case number and surgeon on univariate analysis; however, on multivariate analysis, only differences between surgeons were notable.
Relative to surgeon 1.
Relative to clinical stage I testis cancer.
Relative to right-sided template.
BMI = body mass index; CI = confidence interval.
Operative Time
Operative time was related to case number, clinical stage III testis cancer, and a history of prior exposure to chemotherapy, on both univariate and multivariate analysis.
Relative to surgeon 1.
Relative to clinical stage I testis cancer.
Relative to right-sided template.
Lymph Node Count
Lymph node counts varied only in association with surgeon on both univariate and multivariate analysis.
Relative to surgeon 1.
Relative to clinical stage I testis cancer.
Relative to right-sided template.
Conversions and complications were analyzed. No factors associated with conversion were significant on univariate analysis, so the multivariate analysis was not performed. Specifically, case sequence number (p = 0.269), surgeon (p = 0.137), clinical stage (p = 0.614), prior exposure to chemotherapy (p = 0.556), template (p = 0.776), and BMI (p = 0.358) failed to reach significance. Overall complication rates decreased with surgeon experience on univariate and multivariate analysis (p = 0.003 and p = 0.001, respectively), although the number of complications classified as high grade (Clavien-Dindo Grade III, IV, or V) did not change with experience (Table 4).
Risk of High-Grade Complications
None of the evaluated factors were significantly associated with the risk of high-grade complications.
Relative to surgeon 1.
Relative to clinical stage I testis cancer.
Relative to right-sided template.
There was some variation between operating surgeons with respect to setup time (Table 1), operative time (Table 2), lymph node count (Table 3), and total complication number. This surgeon effects on setup time and lymph node count were identified on both univariate and multivariate analysis. However, there was no difference in the number of high-grade complications between surgeons (Table 4).
Discussion
The landscape of surgical technology is rapidly evolving. The goal of any innovative surgical technique should be its reproducibility and safety. R-RPLND was developed with the goal of matching the oncologic efficacy of open-retroperitoneal lymph node dissection (O-RPLND) while providing the benefits of a minimally invasive approach. Despite reports of comparable perioperative and intermediate-term oncologic outcomes to the conventional open approach, R-RPLND remains limited to a small number of surgeons and thus, a small number of patients. R-RPLND continues to be in the early stages of the diffusion of the innovation cycle (innovators to early adopters). Understanding the learning curve of R-RPLND could benefit experienced robotic surgeons in preparation for the critical surgical steps, which will ensure patient safety and oncologic efficacy.
Our study is the first evaluation of the learning curve with respect to operative time and surgical complications for R-RPLND in the primary and post-chemotherapy testis cancer setting. We found that there was a learning curve associated with operative time but not case setup time. A decrease in operative time as a surgeon becomes more familiar with a new procedure is a phenomenon that has been demonstrated multiple times throughout the recent literature of robotic urologic procedures. Prostatectomy was the first and remains the most commonly performed procedure by a robotic approach. In a meta-analysis of more than 17,000 prostatectomies, Davis and coworkers found surgical time to decrease with surgeon experience and noted that it continued to decrease after a surgeon's 100th case. 12 A similar decrease in operative time with increased experience has been found for robotic nephrectomy with learning curves as short as five cases in a study by Lavery and colleagues. 13 Finally, in a multi-institutional study of 21 surgeons performing robotic radical cystectomy, Hayn and associates found a difference of 115 minutes of operative time (p < 0.0001) between surgeons who performed <30 robotic procedures and surgeons who performed >50. 14 Our model would predict surgical times to decrease by 60 minutes by the 45th case.
Another aspect of the learning curve demonstrated in this study was the decrease of overall complication rate as experience grew. This finding is consistent throughout the research for transition from open to robotic techniques in urology. Davis and coworkers found a decrease in complication rate from 11.75% to 8.93% for 67 surgeons between their first case and their 100th case of robotic prostatectomy. 12 A study by Larcher and colleagues examined perioperative outcomes for robotic partial nephrectomy of two highly experienced surgeons. This study found that the complication rate continued to decrease without a plateau after 300 cases. 15 Importantly in this study, although overall complication rate decreased continually, the rate of complications graded Clavien-Dindo Grade III, IV, or V was stable throughout the study period. This may suggest that although the surgeons are able to better refine their technique as they become more practiced in this operation, the safety of the patients is not compromised during a surgeon's early case sequence numbers for this procedure (in the hands of experienced robotic surgeons).
Historically, LNY has been an important performance measure in oncologic surgery. In primary RPLND for testis cancer, the total number of lymph nodes resected has been shown to have a higher probability of finding a positive lymph node. Total lymph node count has also been shown to be an independent predictor of recurrence in the post-chemotherapy RPLND setting, even in patients with favorable pathology (i.e., only teratoma and fibrosis). However, LNY is often believed to be subjective, dependent on center, processing, and pathologist. In addition, controversies regarding the boundaries of RPLND for testicular cancer persist today as the result of the development of the modified template and nerve-sparing technique. Recent findings demonstrate that mapping studies supporting the modified templates underestimated the incidence of retroperitoneal metastases due to lack of follow-up and liberal use of postoperative chemotherapy in these patients. 16,17 In our study, we demonstrate LNY variation between surgeons on both univariate and multivariate analysis. Despite this variation between surgeons, LNY did not change over time. Others have reported no learning curve associated with LNY in robotic-assisted laparoscopic para-aortic lymphadenectomy combined with oncologic pelvic surgery. 18 This suggests that LNY is probably not impacted in the early adoption of this procedure by an experienced robotic surgeon.
There remains debate regarding the oncologic efficacy of robotic approaches for oncologic procedures when compared with the standard open technique. This topic has been brought to the forefront in the wake of data from gynecologic oncology, suggesting worsened survival for robotic-assisted hysterectomies performed for cervical cancer. Specifically, Ramirez and coworkers performed a randomized control trial comparing minimally invasive (robotic or laparoscopic) vs open hysterectomy for Stage I cervical cancer and found both a decrease in disease-free survival rate (86.0% vs 96.5%) and decreased overall survival (93.8% vs 99.0%) with the minimally invasive approaches. 19 The authors point to increased manipulation and carbon dioxide insufflation as possible sources of increasing the spread of malignant cells at the time of operation. Despite this evidence, the literature does not suggest generalizability of these data to other oncologic operations. Retrospective reviews of robotic approaches for rectal cancer, lung cancer, and endometrial cancer all show similar survival and recurrence rates when compared with the traditional open or laparoscopic approach. 16,20 –23 In addition, Hussein and colleagues analyzed major oncologic endpoints at 10 years from a total of 446 patients who underwent robotic-assisted robotic cystectomy. 24 Recurrence-free survival, disease-specific survival, and overall survival were similar to those reported historically for open cystectomy.
There have been a few studies looking at early oncologic outcomes for R-RPLND. The three largest retrospective studies examining 2 years recurrence-free survival of patients undergoing R-RPLND show rates of 91% to 100%, and all recurrences cited in these studies occurred outside of the original operative field. 5 –7 These rates are similar to the quoted recurrence rate of 92.5% for O-RPLND from a large systematic review performed by Rassweiler and colleagues Although these data are encouraging, a multi-institutional or prospective study would be valuable in further evaluating the oncologic efficacy of R-RPLND. 25
Limitations of this study include its retrospective study design and small case number. Since this procedure is infrequently performed at most institutions, additional multi-institutional studies would help to corroborate our findings. In addition, this study involved four experienced surgeons with many years of practice. To further identify how these learning curves affect training requirements for residents and fellows, a study examining more junior staff would be necessary to further answer these questions. In addition, the surgeons may have shown a tendency to tackle more challenging cases with this approach as their comfort level with the procedure grew with experience, representing a different patient selection criterion for the procedure at the end of the series compared with the beginning. This limitation, however, would only strengthen the notion that there is a learning curve. This study may have also benefited from additional longitudinal follow-up, principally for oncologic outcomes. Overall, this article is intended to focus on the perioperative safety data and technical learning curve and so additional follow-up was not felt critical for this study, but is being tracked by both institutions. Further, in this study, operative time continued to decrease in a linear fashion throughout the entire study period, but a longer study may be able to better identify whether there is point at which the curve plateaus, thus concluding the operative time-learning curve.
Conclusions
Consistent with the learning curves shown for other technologically advanced surgical techniques, experience appears to improve surgical times and lower complication rates. Attention to variations in individual surgeons' techniques for R-RPLND may provide opportunities to improve setup time and LNY, improving the overall quality of care for these patients. Disease characteristics play a role in operative times, but they do not predict the likelihood of a perioperative complication. These findings suggest that this procedure can be successfully adopted, safely performed, and continually improved by experienced robotic surgeons.
Footnotes
Acknowledgments
The views expressed in this article are those of the authors and do not reflect the official policy or position of the Department of the Navy, Department of Defense, or the U.S. Government.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this project.