
Abstract
Objectives:
To determine which flexible ureterorenoscopy program would be most cost-efficient in our center, a cost efficiency analysis and a formula to assess cost efficiency feasibility of a hybrid model were performed.
Methods:
Total cost per case of reusable flexible ureterorenoscopes (rfURS) was retrospectively calculated and compared with two single-use flexible ureterorenoscopes (sufURS) marketed. A mathematical formula was developed from our data to identify the necessary increase of use of rfURS (NIU-rfURS) to be cost-efficient in a hybrid system utilizing sufURS for only high-risk-of-breakage cases.
Results:
In 57 months, 983 procedures were performed using 4 digital rfURS (Flex-XC; Storz), necessitating 45 repairs, with a total repair cost of €256.809. Including the capital investment of €24.000 per scope and €60 per sterilization cycle, the cost per case averaged €419 after 983 cases. Consistently using sufURS would have cost 55% to 127% more (respectively, Uscope PU3022® and Lithovue® at €650 and €950 manufacturer suggested retail price). On a per case analysis, the cost was initially extremely high, but declined to reach a plateau around €480 after ∼400 cases. After 155 or 274 procedures, a rfURS program appeared more cost-efficient than consistently using Lithovue or Uscope PU3022, respectively. Based on our data and formula, if we would hypothetically use Uscope PU3022 or Lithovue for 15% of the cases, the NIU-rfURS is, respectively, 28% or 74% (∼6 or 16 cases). The NIU-rfURS increases exponentially with an increased use of sufURS.
Conclusion:
Consistently using rfURS is more cost-efficient than the constant use of sufURS after 155 to 274 cases. We describe the first mathematical formula that allows a calculation and feasibility assessment of using both reusable and disposable fURS. To identify whether a hybrid system may be a feasible cost-efficient alternative to a rfURS-only program, any center can calculate the NIU-rfURS by entering center-specific data in the formula.
Introduction
The use of ureterorenoscopy (URS) for urinary stone disease has dramatically increased in the last few decades. 1 In parallel, a plethora of technologic advancements has allowed this procedure to evolve significantly. 2
Modern reusable flexible ureterorenoscopes (rfURS) provide excellent image quality together with good maneuverability. Despite improvements over the years, rfURS remain fragile instruments frequently needing repairs. 3 Not only the use in high-risk-of-breakage cases but also the sterilization process influences the lifespan of a rfURS. 4 Borofsky et al. demonstrated that the majority of expenses in a rfURS program are due to repair costs, accounting for 70% to 75% of total costs after only 100 cases. 5 Additional to the fragility and perceived high cost per case of rfURS, the possible contamination of reprocessed rfURS and sterility of single-use flexible ureterorenoscopes (sufURS) are definite arguments driving the market toward sufURS. 6,7
Current generation sufURS appear to compare favorably to rfURS in most aspects. Multiple in vitro studies found comparable mechanical, optical, and irrigation characteristics. 8 –14 In a systematic review by Davis et al., sufURS demonstrated no statistically significant difference in clinical outcomes such as perioperative complications and stone-free rates. 15
To identify which flexible URS program is most cost-efficient, a cost efficiency analysis needs to be performed. In contrast to sufURS, where there is a fixed cost per procedure, rfURS are characterized by fluctuating costs. After a high initial investment, the maintenance cost is determined by cost for repairs and sterilization. Systematic reviews of cost efficiency analyses already performed suggest that rfURS is cost-efficient in centers performing a high volume of procedures or performing a reasonable number of cases before scope repair is necessary. 15 –17 A hybrid system, in which sufURS are used for only high-risk-of-breakage cases has been hypothesized to extend the lifespan of the rfURS and to reduce overall cost per case. 18,19 These data, however, are all specific to each reporting center and may therefore not be applicable to other centers across the globe, where different repair and reprocessing costs as well as different prices for rfURS and sufURS may exist.
The aim of the study is to determine which flexible URS program would be most cost-efficient in our center. This includes the development of a mathematical formula, including easily obtainable variables that would allow its use by any other center globally, to assess the influence of sufURS use on rfURS lifespan.
Methods
All URS procedures, using flexible ureterorenoscopes between March 2016 and November 2020 were identified. Diagnostic as well as therapeutic cases, including treatment of calculi, upper tract urothelial carcinoma, and ureteral strictures, were included. The scope was used by the supervising surgeon (T.T.) and by his residents and fellows. Ethical approval was obtained from the Institutional Ethics Committee (IRB approval numbers are B670201733819 and B670201733724). No patient data or procedural details were collected.
During the study period, four rfURS (Flex-XC; Storz) were used. After each procedure, damage assessment and leak test were performed by the surgeon. During each reprocessing cycle, another assessment was performed. In the event of apparent damage or leakage, the scope was sent for repair by the original manufacturer. According to the maintenance contract with the company, a refurbished new scope was introduced as a replacement for each defective scope. Repair costs were dependent on the level of damage as assessed by the manufacturer. A distinction was made between major, minor, and minimal damage with accompanying repair cost of €10357.5, €2.711, and €909, respectively.
The scope reprocessing is performed in the central sterilization unit of the hospital using the STERRAD® system. The cost associated with reprocessing was calculated as the sum of the average cost of the various components of the sterilization cycle, including labor time.
Number of procedures and repairs per scope were logged during the study period. Average uses before repair and total cost per case were calculated. Total cost associated with the use of rfURS was compared with two sufURS marketed, Uscope PU3022® (Zhuhai Pusen Medical Technology Co, Ltd., Zhuhai) and Lithovue® (Boston Scientific, Marlborough, MA) at €650 and €950 as the manufacturer's suggested retail price (MSRP), respectively.
The total cost per case for rfURS was calculated according to the following formula:
Total cost per case rfURS = ((Purchase price × 4)/n) + reprocessing cost + (total repair cost/n) where n is the total number of cases performed at each given point in time.
The adaptable variables in the developed Hybrid fURS Formula include the average rfURS repair cost, the average rfURS sterilization cost, the average rfURS usage before repair, the sufURS purchase cost and the sufURS percentage used. The formula intends to predict the necessary increase of use of rfURS (NIU-rfURS) before needing a repair to be cost-efficient in a hybrid model (Fig. 1).

Hybrid fURS Formula. Necessary increase of use of rfURS to stay cost-efficient in a hybrid model. fURS = flexible ureterorenoscopy; rfURS = reusable flexible ureterorenoscope; ΔRepCost = average reusable ureterorenoscope repair cost; %sufURS = single-use flexible ureterorenoscope percentage used; sufURSCost = single-use ureterorenoscope purchase cost; SterCost = reusable ureterorenoscope sterilization cost; ΔrfURSCost = average cost per case of a reusable ureterorenoscope, calculated as the sterilization cost plus the repair cost per case; ΔrfURSUse = average reusable ureterorenoscope usage before repair in a rfURS-only program.
Results
During the study period of 57 months, 983 procedures using rfURS were performed. The capital investment for the four digital rfURS was €24.000 per scope.
During the study period, 45 repairs were necessary, with a total repair cost of €256.809. Of the 45 repairs, 22 were categorized as major cost (€10357.5), 9 as minor cost (€2.711), and 5 as minimal cost (€909). Nine repairs were under warranty, of which six were covered by the insurance of the sterilization department and three by the company (Table 1). The average repair cost was €5.707.
Number of Repairs Per Scope
The average rfURS usage before repair was 21.8 cases (range 1–60). The total cost per case after 983 procedures, including the capital investment €96.000, the cost of €60 per sterilization cycle, and the average repair cost of €261 per case, was €418.9.
On a per case analysis, the cost per case was initially extremely high, but declined to reach a plateau around €480 after ∼400 cases. After 155 and 274 procedures, a complete rfURS program appeared more cost-efficient than consistently using Lithovue or Uscope PU3022, respectively (Fig. 2). After 983 cases, consistently using Uscope PU3022 would have cost 55% more than consistently using a rfURS, which corresponds to a price difference of €231.1 per case. Consistently using Lithovue would have cost 127% more, which corresponds to a price difference of €531.1 per case.
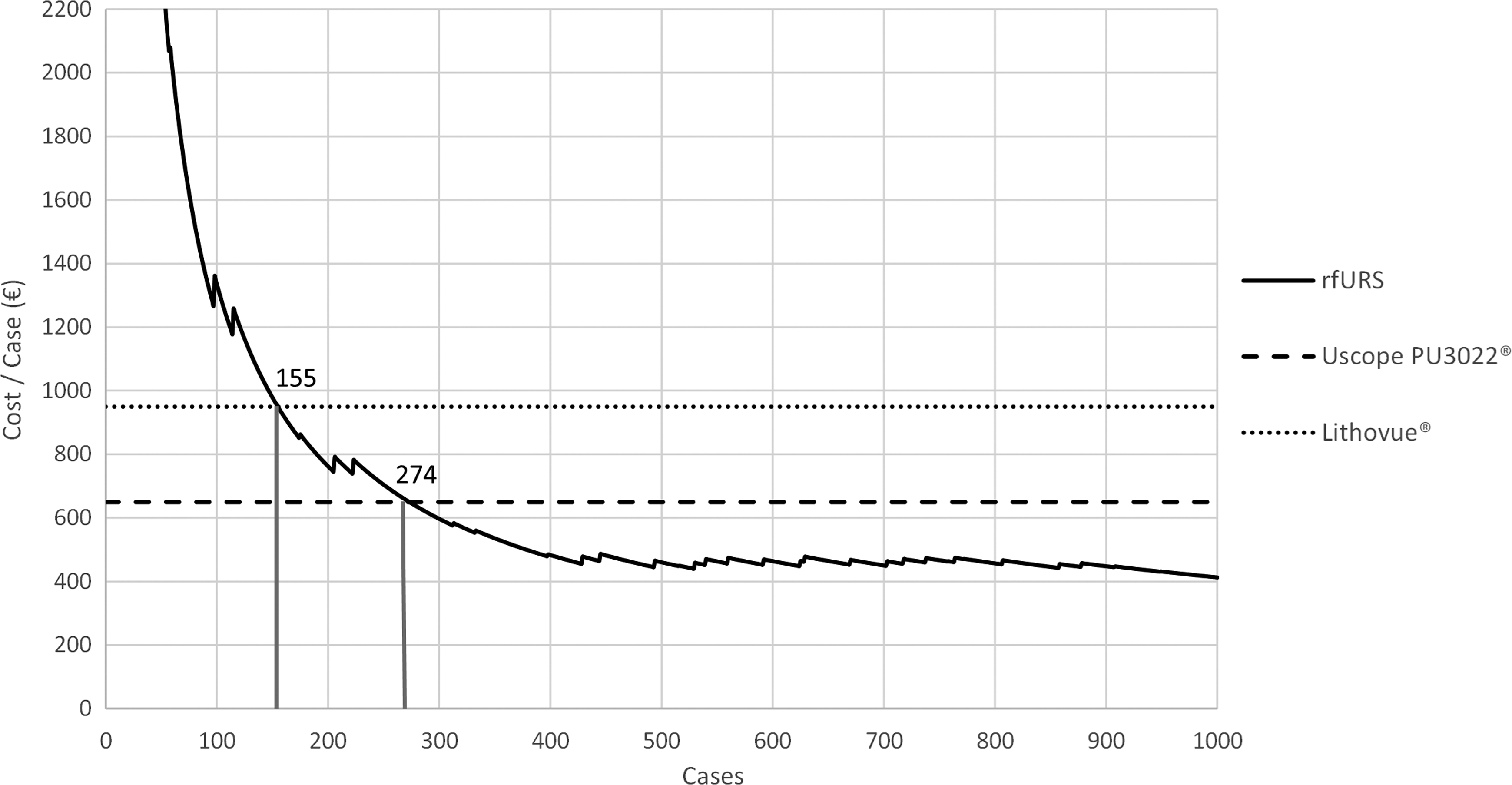
Total cost per case analysis of rfURS compared to sufURS. After 155 or 274 procedures, a rfURS program appeared more cost-efficient than consistently using Lithovue® or Uscope PU3022®, respectively.
Based on the average costs derived from our data (rounded average repair cost of €5.700, sterilization cost of €60, and average usage before repair of 21.8 cases), the NIU-rfURS can be calculated considering the sufURS percentage used in a hybrid model. If we would hypothetically use Uscope PU3022 or Lithovue for 15% of the cases, the NIU-rfURS would be 28% or 74%, respectively. This translates into an average rfURS usage before repair of, respectively, 28.0 or 37.9 cases, or an increase of ∼6 or 16 cases, to be cost-efficient in comparison to consistently using rfURS. At a 25% Uscope PU3022 or Lithovue use, the NIU-rfURS would be 72% or 403%, or an increase of ∼16 or 88 cases, respectively. The NIU-rfURS increases exponentially with an increased usage of sufURS (Fig. 3).
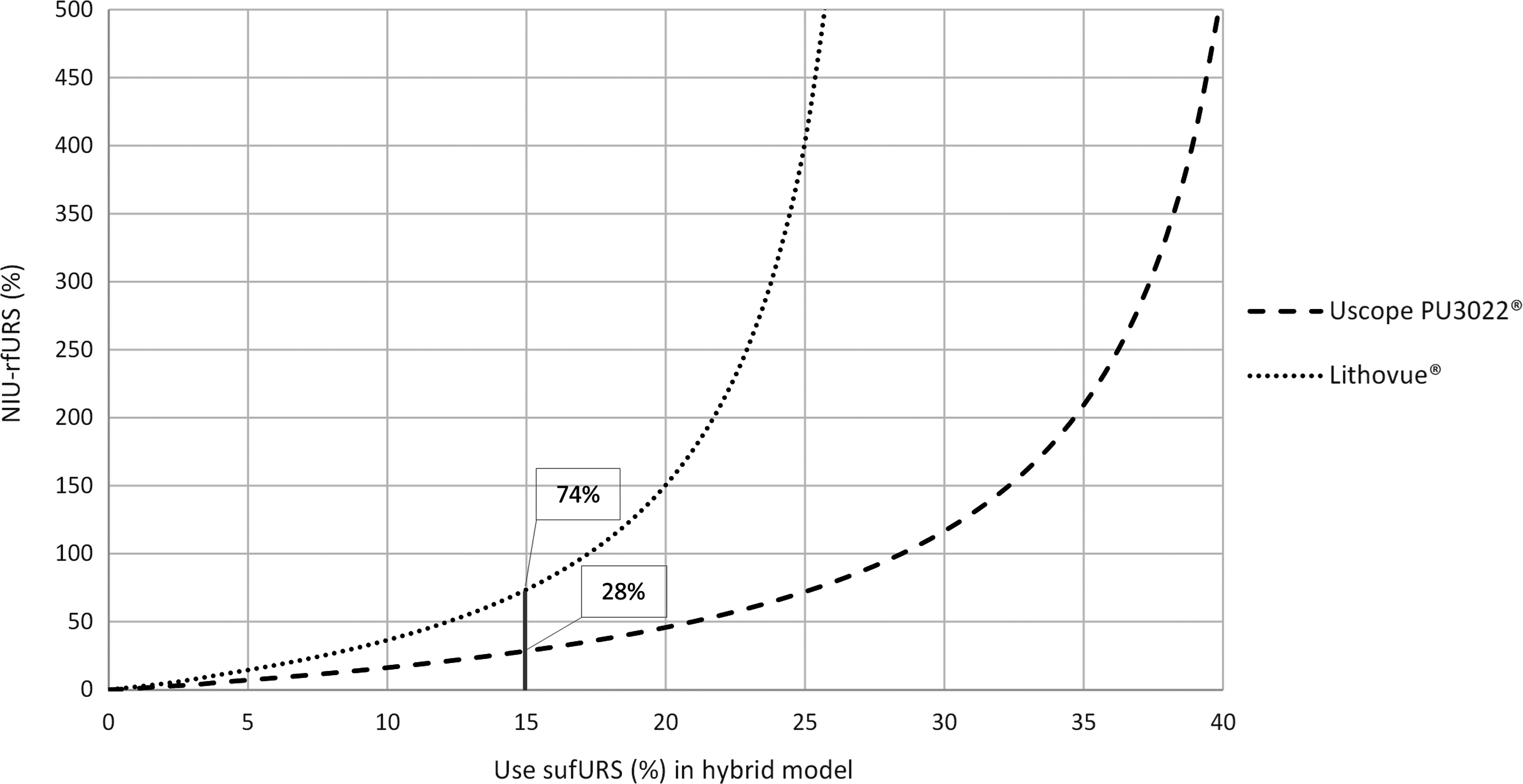
Necessary increase of use of rfURS in function of use of sufURS. With a hypothetically 15% use of Uscope PU3022 or Lithovue, the NIU-rfURS is, respectively, 28% or 74%. The NIU-rfURS increases exponentially with an increased usage of sufURS. NIU-rfURS = necessary increase of use of rfURS.
Discussion
Despite a high initial capital investment and the considerable repair costs, we have demonstrated that after a certain amount of cases, a complete rfURS program is less costly than a complete sufURS program, dependent on the cost of sufURS. As the capital investment is divided by increasing more cases and the reprocessing cost is steady, the cost per case will decrease as the number of cases increases. By consequence and as demonstrated by Borofsky and colleagues., the repair cost will eventually account for most of the cost in a rfURS program. 5
While previous studies have reported that a certain annual caseload would be needed to be cost-efficient, 20,21 the total number of cases performed may be more important than the time within which they are performed. As demonstrated by Figure 2, total cost per case decreases by case, reaching a plateau after ∼400 cases. In our study, we performed a cost per case analysis rather than a cumulative cost analysis to compare cost efficiency between a rfURS and a sufURS program.
Mager and colleagues compared cost of rfURS (Storz Flex X2S/Flex-XC) with Lithovue ($1300) in 68 matched procedures and found that the total investment for sufURS exceeded the costs of rfURS after 61 to 118 procedures, depending on the market price or MSRP of rfURS, respectively. 20 In a study by Martin and colleagues, total cost after 150 performed rfURS (Storz Flex-XC) cases was compared with the hypothetical cost of Lithovue ($1500). After 99 procedures, the rfURS program was cost-efficient compared to systematically using Lithovue. 21 Our estimated cost efficiency after 155 rfURS cases in comparison to Lithovue is somewhat higher than those previously reported, which may be due to the higher initial purchasing cost in our calculations, including 4 rfURS. However, our total cost per case after initial investment of €321 compares favorably to the previously reported $436 to $848. 19,20 Ozimek and coworkers calculated the average total cost after 423 rfURS (Storz Flex X2/Olympus URF-V) procedures at €503 per case, which was more cost-efficient than the potential cost of Lithovue (€1000). 22 This is supported by our own data that demonstrate an average total cost per case around €480 after 400 cases.
The average repair cost after 15 repairs of 7 new digital scopes (Olympus URF-V) used for 234 procedures was calculated by Hennessey and coworkers as A$695 (Australian dollars) per case, 23 which was remarkably higher than our €261 average repair cost per case. In their cost efficiency analysis, they compared the estimated total cumulative cost after only 28 cases (A$50,000) with the hypothetical cost of Lithovue and stated that a sufURS program would be cost-efficient if the sufURS would be priced at <A$1.200. As we have demonstrated that the cost per case decreases considerably by each extra case, the suggested price to reach cost-efficiency would likely have been lower with a cost efficiency analysis, including >28 cases.
In a microcosting analysis, Taguchi et al. prospectively compared total cost per case of 14 cases with rfURS (URF-P6) to 9 cases with Lithovue. The total cost per case was calculated to be comparable, mainly due to the 20 minutes reduction in overall operative time and absent costs for recycling and reprocessing with sufURS. 24 It should be noted, however, that sufURS in this study was compared to fiberoptic rfURS, which has been demonstrated to account for an increase of mean operation time by 10 minutes in comparison to digital rfURS. 25,26 Although in our analysis, all used rfURS were digital scopes, the average cost per case after 983 cases attributable to the initial investment was €97.7, which is comparable to the $116 reported by Taguchi and colleagues.
The transition to a hybrid model may help to increase the average usage of rfURS before needing repair. 18,19 –27 A study by Munver and associates showed a 2-year cost saving of 44% by reducing the number of repairs after introducing Lithovue in their flexible URS program. 19 They used sufURS in 28.8% of cases and indications for sufURS use were large stone burden (>1.5 cm), >3 lower pole stones, extensive laser use with expected operative duration >1 hour, bilateral URS, stones within complex renal anatomy, and placement of the ureterorenoscope through a trocar or nephroscope sheath. In addition, Al-Balushi and colleagues highlighted that the addition of sufURS eliminated the 15% procedure cancellations in the program without sufURS. 28
With a hypothetical 15% sufURS use, the lifespan of a rfURS in our center would have to increase by 6 or 16 cases, considering the lowest or highest cost of sufURS. Whereas an additional 6 cases seems attainable, 16 cases may be a high reach, as the lifespan of an rfURS is partly influenced by the reprocessing technique. 4 The formula is adaptable to different situations, depending on the hospital-specific variables as previously reported. When we compare for example, two hypothetical centers (HC1 and HC2) with an average repair cost of €6.000, a sterilization cost of €60, and differing only in average usage before repair of 15 vs 35 cases, respectively, the NIU-rfURS differs considerably (Fig. 4). For HC1, a 15% sufURS use at MSRP of €650 vs €950, would suggest a NIU-rfURS of 9% vs 28%. This corresponds to an average rfURS usage before repair of 16.4 vs 19.2 cases or an absolute increase of 1.4 vs 4.2 cases per scope to maintain cost efficiency. For HC2, a 15% sufURS use would suggest a NIU-rfURS of 76% vs 284%, which corresponds to an average rfURS usage before repair of 61.6 vs 134.4 cases or an absolute increase of 26.6 vs 99.4 cases per scope. This demonstrates that the lower the usage before repair in the rfURS program, the more likely a hybrid system can be cost-efficient. Entering hospital-specific data in the formula can help an institution decide if a hybrid system may be a feasible alternative to their rfURS program. This formula of course needs to be prospectively validated.
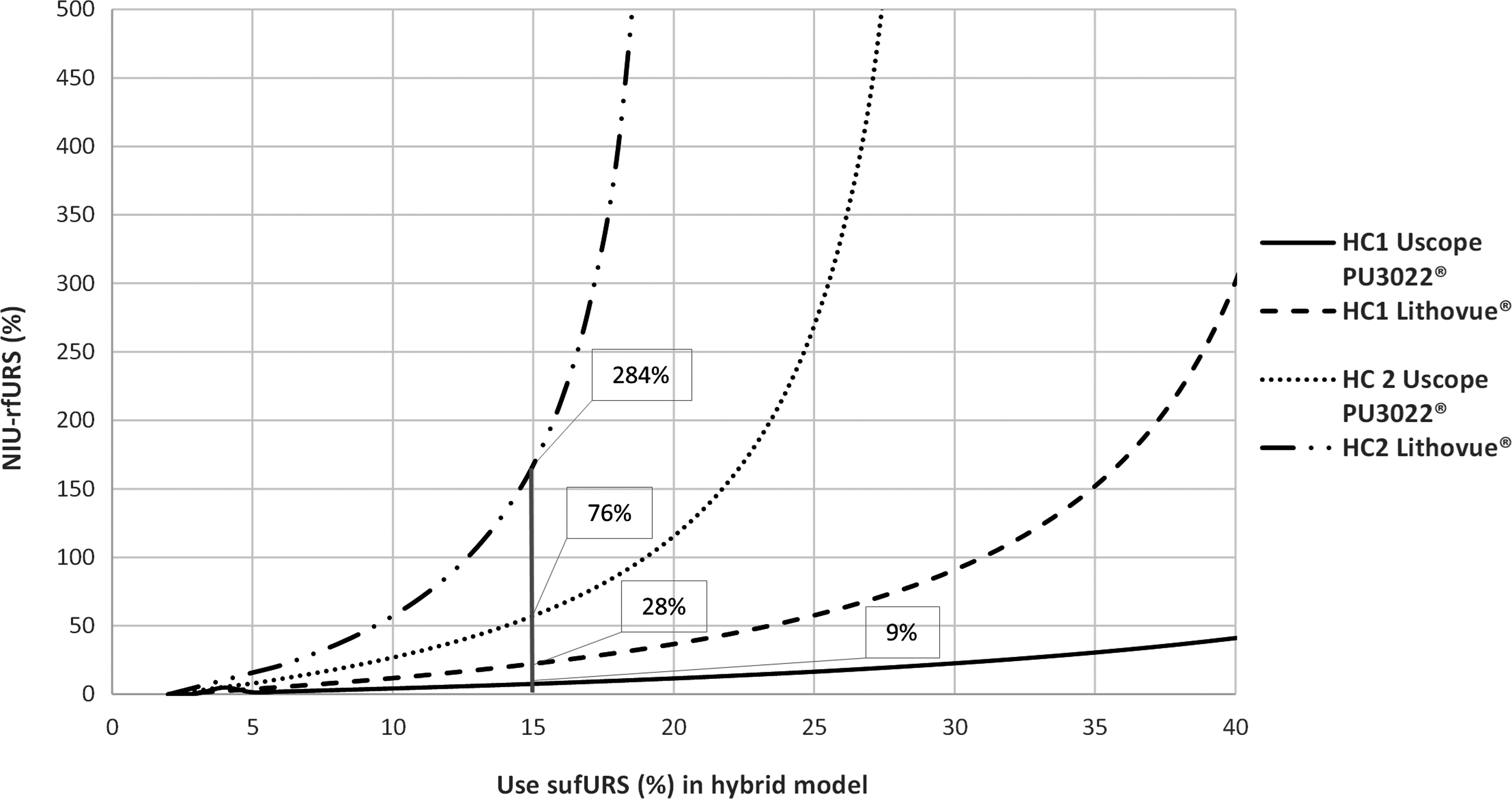
Adaptability of the NIU-rfURS formula. When two HC1 and HC2 with an average repair cost of €6.000 and a sterilization cost of €60 differ only in average usage before repair of 15 (HC1) vs 35 (HC2) cases, the NIU-rfURS differs considerably. The lower the usage before repair in the reusable ureterorenoscopy program, the more likely a hybrid system can be cost-efficient. HC = hypothetical center.
Steward and colleagues suggest that disposable equipment may decrease the risk of contamination by equipment especially now in times of COVID-19. 29 Although some viral RNA has indeed been detected in 3% to 4% of urine samples from COVID-19 patients, only one case has been reported on the identification of an infectious virus in a urine sample and the likelihood of contamination through equipment is low. 30,31 It would, however, be cautious to use sufURS in a confirmed COVID-19 patient.
To the best of our knowledge, this is the largest case series to date analyzing cost efficiency of flexible URS using rfURS. The main limitation of our study is inherent to the retrospective nature of our data. Cost per case was based on purchase, reprocessing, and repair cost. Other equipment such as laser and disposables were not taken into account as they were hypothesized not to differ between groups. The sufURS purchase cost was based on MSRP. Depending on the negotiated sufURS market price, which may be lower, more cases may be needed with rfURS before demonstrating cost efficiency. In addition, if the repair costs for the 9 scopes that were repaired under warranty had been counted toward the total costs, the repair cost per case would have been higher than the reported €261, ranging from €270 to €356 considering 9 times the lowest or highest repair cost, respectively. Furthermore, an evaluation of potential reasons for scope breakage was not performed as this was outside of the scope of this analysis. In real-life validation, identifying high-risk-of-breakage cases will be useful to identify when to use a sufURS. The strength of this study is the large number of consecutive cases included in the analysis. As all cases were performed in a tertiary hospital, the scopes were used by the primary surgeon as well as by fellows and residents, which can possibly increase the repair rate. We feel that this is a strength rather than a weakness as this reflects real-life situations. The NIU-rfURS formula is intended for centers interested in identifying cost efficiency of transitioning from a rfURS only to a hybrid program. At this point, the initial capital investment can be considered a sunk cost and has as such not been included in the formula. Finally, some parameters in our formula are based on the current costs. It is possible that not only the repair rate of rfURS but also the repair cost may decrease with increased use of sufURS. This fixed average repair cost may therefore cause a possible overestimation of the NIU-rfURS.
Conclusion
Based on our data, consistently using reusable digital flexible ureterorenoscopes is more cost-efficient than the consistent use of sufURS after 155 to 274 cases. The average cost per case using a reusable ureterorenoscope reaches a plateau after ∼400 cases to a steady cost of ∼€480 per case.
We have developed a mathematical formula using adaptable center-specific variables that can identify if and how a hybrid system can be cost-efficient considering an increased usage per reusable ureterorenoscope before needing a repair. Although this formula still needs prospective validation, it can help colleagues identify whether or not a hybrid system may be a feasible alternative to reusable ureterorenoscopes in their hospital.
Footnotes
Author Disclosure Statement
T.T. is a consultant for Cook Medical, Boston Scientific, and Storz. No conflicts of interest to disclose for the other authors.
Funding Information
No funding was received for this article.