
Abstract
Introduction:
To evaluate the efficacy and safety of performing extracorporeal physical vibrational lithecbole (EPVL) through greater sciatic foramen (GSF) for distal ureteral calculi (DUC) treatment.
Materials and Methods:
All patients with a diagnosis of DUC (6–10 mm in diameter) were enrolled in this study from October 2018 to May 2020. Patients were randomly divided into three groups receiving EPVL through GSF (Group A, n = 58), or abdominal (Group B, n = 60), or combined with oral use of tamsulosin at 0.4 mg daily (Group C, n = 63).
Results:
There was no significant difference observed in terms of demographic characteristics or size of stones among the three groups (p > 0.05). Compared with the Groups B and C, patients of the Group A displayed a significantly higher score of comfort, with a significantly decreased number of renal colic attacks or analgesics required (p < 0.01). The stone-free rate also significantly increased after 1 and 2 weeks of treatment (p < 0.01), despite such a significant difference among these groups vanishing after 4 weeks of treatment.
Conclusion:
EPVL in the prone position uses the GSF as the path and is a safe and effective approach to treat the distal ureteral calculi.
Introduction
Urolithiasis is one of the most common urologic diseases, in which ureteral stones account for ∼20%. 1,2 The probability of obstruction of ureteral stone is higher, and so, it needs to be removed as soon as possible. 3 Failure to treat ureteral stones timely will lead to complications such as urinary tract infections, hydroureter, and renal colic. 4 Distal ureteral stones account for 70% of ureteral stones, 1 and treatment methods include surgical treatment, extracorporeal shock wave lithotripsy (SWL), and medical expulsive therapy (MET). Clinically, most of the distal ureteral stone patients have stone size of <10 mm. The European Association Urology (EAU) guidelines recommend SWL and MET as the first-line of treatment for this disease. 5
It has been shown that the greater sciatic foramen (GSF) represents a safe and effective treatment path for SWL to treat distal ureteral calculi (DUC). In 2010, Lu et al. 6 reported that the use of SWL with sciaticum majus foramen or sciaticum minus foramen as a path to treat DUC led to 81.5% of stone-free rate (SFR). Anatomically, sciaticum majus foramen or sciaticum minus foramen refers to a bone gap of bony pelvis, in which part of the distal ureteral can be easily visualized. Moreover, extracorporeal physical vibrational lithecbole (EPVL) has recently emerged as a new technology, which can efficiently generate multidirectional simple resonant motion waves to push stones out of the body. EPVL has also been shown to be safe and effective without causing obvious complications. Several randomized controlled trial (RCT) experiments have further validated that EPVL can significantly promote expulsion of stones after SWL or retrograde intrarenal surgery (RIRS). For example, Liu et al. 3 used EPVL to treat DUC with stone size less than 1 cm and found that the SFR in the EPVL group after 2 weeks was comparable with the one with use of tamsulosin. In some previously published studies on EPVL, the harmonic vibration generated by the main oscillator mainly acted on the stones through the abdomen to facilitate the rapid discharge of the stones. However, in practice, we need to apply a certain amount of pressure to the main vibrator to reduce the skin-to-stone distance (SSD). However, this will also cause discomfort for the patient, such as abdominal pain and urgency to urinate. Therefore, we wish to find a safer and more effective path for EPVL to expel the stone. Based on the above, we used the GSF as the transmission path of EPVL and found that this method is better tolerated by patients, and the rate of stone removal is also faster. To further verify this method, we designed this study and divided the patients into three groups, EPVL through GSF, EPVL through abdomen, and MET to compare the safety and effectiveness among them.
In this study, we sought to design this RCT approach to assess the safety and effectiveness of EPVL treatment of DUC through GSF.
Materials and Methods
Patients
From October 2018 to May 2020, a total of 195 patients diagnosed with distal ureteral stones (6–10 mm) were admitted to our hospital for treatment and enrolled in this study (Fig. 1). All patients underwent routine preoperative evaluation, including medical history investigation, physical examination, and urine, blood, and renal function tests. All procedures performed in the study are in full compliance with the ethical standards of the Affiliated Jiangning Hospital of Nanjing Medical University and the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. This study was approved by the Ethics Committee of the Affiliated Jiangning Hospital of Nanjing Medical University.
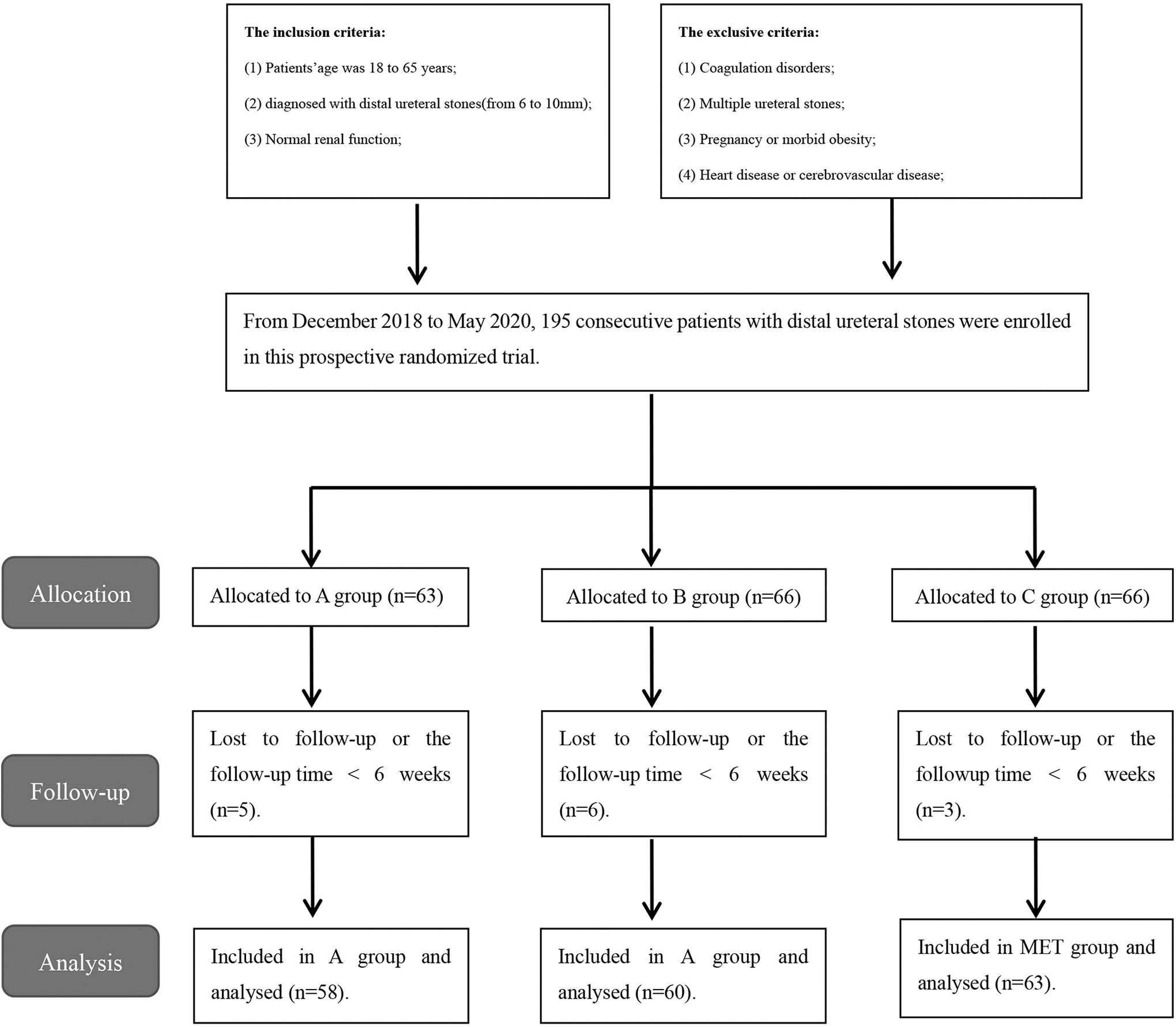
Flowchart for case selection.
After signing an informed consent, patients were randomly assigned to one of the three treatment groups by our research staff. Randomization was concealed sealed envelopes with a 1:1:1 allocation ratio. Patients in Group A received EPVL treatment through GSF; Group B patients received EPVL treatment through the abdomen; and patients in Group C received MET treatment. A diagnosis of distal ureteral stones was based on patient's clinical presentations and findings of plain radiographs, ultrasonography, and CT. The maximum diameter of the stone was measured on a plain abdominal film and CT and recorded. All procedures were performed by the same urologist.
Working mechanism of device
EPVL (VT300 Mechanical Percussion Lithecbole Couch [Shenzhen WIKKON Medical Apparatus Co., Ltd., Shenzhen, China]; Fig. 2) is a new device recently developed in China and has been used at our institute. Its structure is simple: a main oscillator held by hand and a suboscillator placed in the treatment bed, loaded with a multidirectional harmonic motion technology. The lateral acceleration can be achieved by a physical vibration device in the base using a harmonic vibration wave in the horizontal direction mode (vibration frequency: 30–80 Hz, amplitude: 7 mm). An axial effect is then produced to induce the detachment of distal ureteral stone from the ureter. The moving space is expanded by a physical vibration device in the handle through a harmonic vibration wave in the multidirection mode (vibration frequency: 5–30 Hz, amplitude: 9 mm). Finally, following position change, under the direction of extracorporeal physical vibration machine, distal ureteral stones will be actively expelled from the ureter.
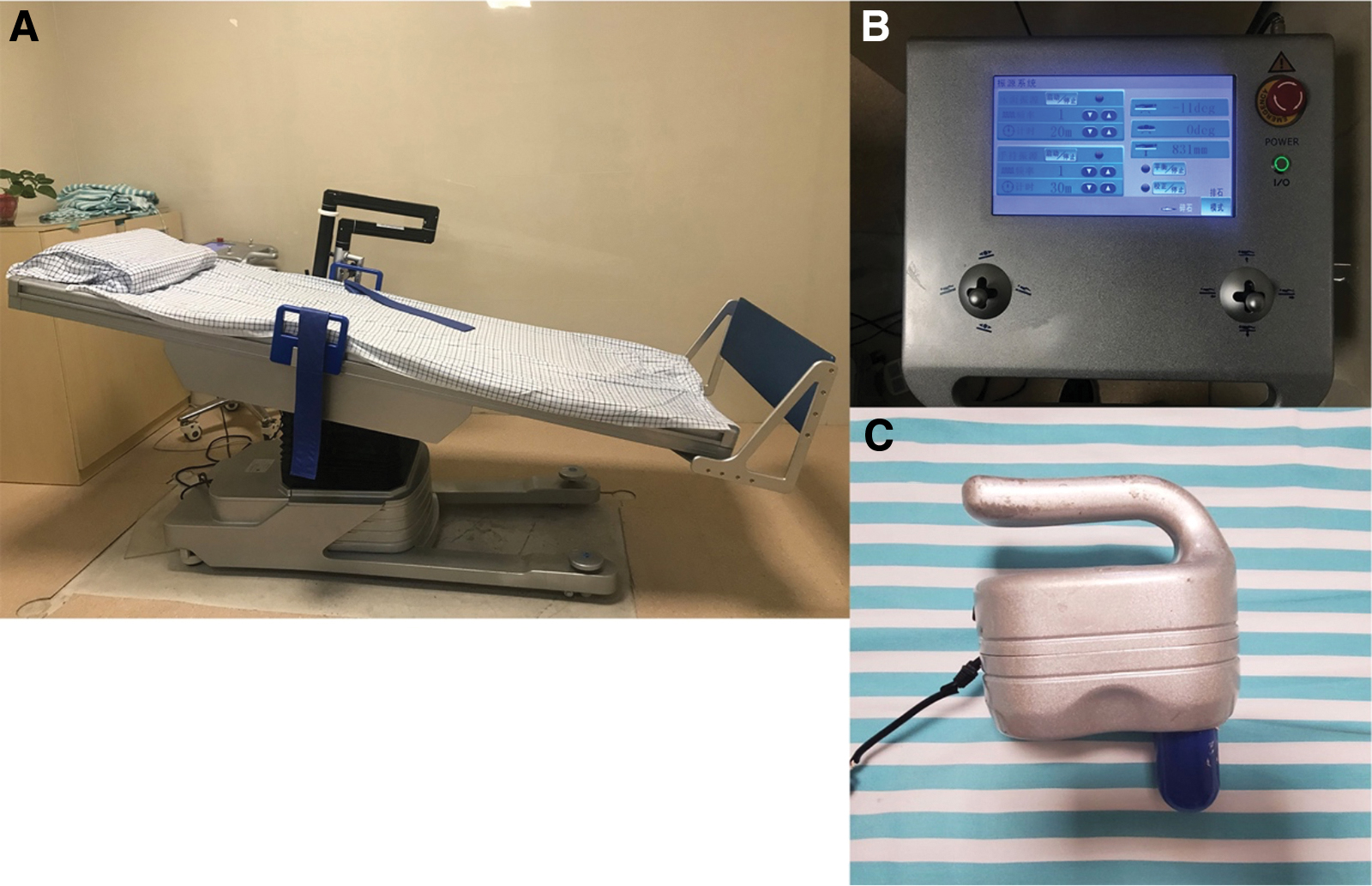
Prototype of VT300 Mechanical Percussion Lithecbole Couch:
Study procedure
In Groups A and B, patients were required to drink 1000 mL of water to fill the bladder before receiving EPVL treatment. During the procedure, we first changed the angle of the treatment bed (head high and foot low), and then applied pressure to the main oscillator for 15 to 20 minutes at the ureter with stones. Group A patients were in the prone position, and the main vibrator was placed at the patient's GSF, which served as the path for the vibrator to generate simple harmonic waves (Figs. 3 and 4). Group B patients were placed in a supine position, and the main vibrator was placed at the patient's ureteral stones on the abdomen (Fig. 5). The frequency of the main oscillator and suboscillator was 5 and 30 Hz, respectively. After EPVL, we used ultrasound to observe location and movement of stones, and at the same time, decided when to proceed for the next treatment. Patients of Group C orally received 0.4 mg of tamsulosin PO qd for 4 weeks. All patients were also given the nonsteroidal anti-inflammatory drug indomethacin 100 mg whenever needed and required to drink at least 2 L of water daily. Pain descriptions were recorded by the patients using the visual analog scale (VAS).
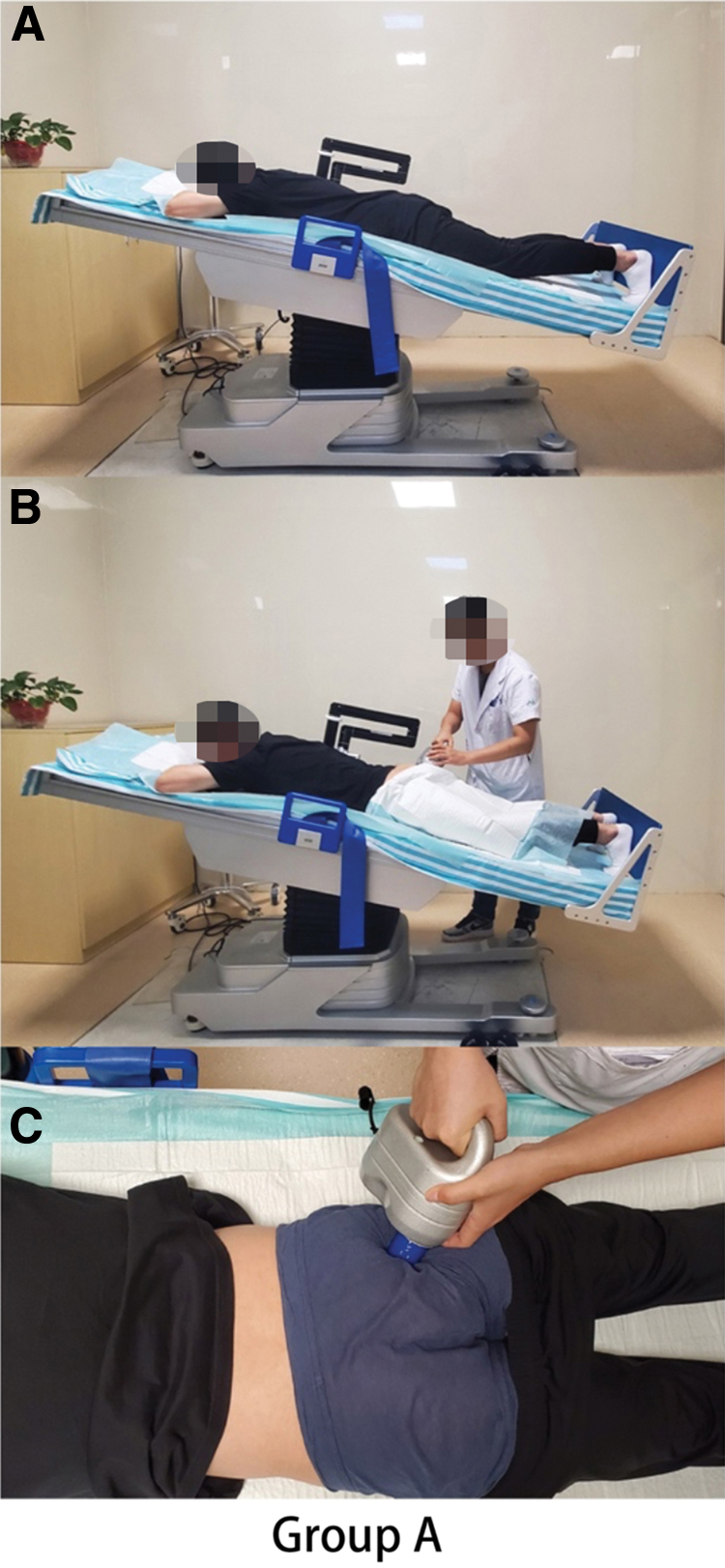
Patients in Group A.

The GSF and ureter

Patients in Group B.
Follow-up
The stone-free status (SFS) was defined as negative for stones on CT and kidney, ureter, and bladder radiograph (KUB). Follow-up was conducted within 4 weeks following treatment. To test whether stones were discharged, doctors required all patients to filter their urine. During follow-up, the patient's stones were reexamined using ultrasound, plain radiograph, or CT. The SFR, stone clearance time, VAS during EPVL, VAS before treatment and 1.2 weeks after treatment in the three groups, and complications related to EPVL were recorded. In addition, analgesic requirements were recorded, and the number of patients with renal colic was also reported to the doctor. Patients with stones not discharged after 4 weeks would receive ureteroscopy.
Study outcomes
The primary outcome was the SFR at 1, 2, and 4 weeks after the first treatment. Secondary outcome was the complication rate at 1, 2, and 4 weeks after the first treatment.
Statistical analysis
The statistical software program SPSS 26.0 (IBM, Armonk, NY) was used in this study. Data are expressed as mean ± standard deviation. One-way analysis of variance (ANOVA), chi-square test, or Fisher's test was used for statistical analysis wherever applicable. Statistical significance was set at p < 0.05.
Results
A total of 181 patients were enrolled in this study and randomly assigned to the three groups: Groups A (n = 58), B (n = 60), and C (n = 63). There were 113 men and 68 women in the study. The patients' demographics and clinical characteristics are shown in Table 1. There was no statistical difference in terms of age, body mass index, gender, hypertension history, diabetes history, hydronephrosis, stone size, HU, and laterality among the three groups (p > 0.05).
Patients' Demographics and Clinical Characteristics
Group A = EPVL through the GSF; Group B = EPVL through the abdomen; Group C = MET; p < 0.05 is considered statistically significant.
BMI = body mass index; GSF = greater sciatic foramen; MET = medical expulsive therapy; SD = standard deviation.
Table 2 summarizes the results of treatment. The frequencies of renal colic and doses required for analgesics following treatment in Group A were 2.29 ± 0.99 or 182.76 ± 108.50 mg, respectively, which were significantly reduced compared with Group B (3.48 ± 1.16 and 236.67 ± 121.78 mg, respectively) or Group C (3.57 ± 1.17 and 304.76 ± 126.62 mg, respectively, p < 0.05). The VAS was 7.19 ± 1.08 for Group A, 7.35 ± 1.02 for Group B, and 7.22 ± 1.02 for Group C (p = 0.675) before treatment, 4.71 ± 1.46, 5.45 ± 1.44, and 6.78 ± 1.16 after 1 week of treatment (p < 0.001), and 2.41 ± 0.97, 3.08 ± 1.15, 6.41 ± 1.34 (p < 0.001) after 2 weeks of treatment, respectively. The VAS of Groups A and B when receiving treatment was 1.69 ± 0.81 and 2.87 ± 1.32, respectively (p < 0.001). In addition, we observed that the achieved SFR in Group A was significantly higher than that of Group B or C after 1 or 2 weeks of treatment (p < 0.001), despite such a significant difference vanishing after 4 weeks of treatment. The mean stone expulsion time of the three groups was 6.70 ± 3.87, 10.82 ± 6.84, and 11.17 ± 7.18 (p < 0.001). A total of 14 patients who were not stone free after 4 weeks of follow-up were treated with ureteroscopy. Ureteroscopic findings revealed a moderate-to-severe stone-induced mucosal inflammatory reaction with polypoid change. However, there was no statistical difference in terms of complications among these three groups, including dizziness, headache, fatigue, and hematuria.
Clinical Outcomes
Group A = EPVL through the GSF; Group B = EPVL through the abdomen; Group C = MET; p < 0.05 is considered statistically significant.
There is a statistical difference compared with Group A.
There is a statistical difference compared with Group B.
EPVL = extracorporeal physical vibrational lithecbole; SD = standard deviation; SFS = stone-free status; VAS = visual analog scale.
Discussion
Although ureteral stones >6 mm are occasionally discharged spontaneously, EAU guidelines recommend active treatment for these stones. 5 Alpha blockers (a-blockers) usually act as a first-line drug for ureteral stones <10 mm, 7 and tamsulosin is one of the most commonly used a-blockers. 8,9 Other auxiliary methods including mechanical percussion, diuresis, and inversion (MPDI) can effectively promote the discharge of stones. 10 –12 At the same time, patients taking MPDI therapy are also well tolerated. 13 However, there is a lack of sufficient evidence supporting effectiveness of these approaches. To promote the rapid discharge of stones, Chinese surgeons have developed EPVL equipment based on the principle of MPDI and put it into clinical use. In this study, we conducted a prospective randomized-controlled trial and showed that EPVL through GSF is safe and effective, which should constitute an excellent option for treatment of DUC.
In this study, we aimed to promote discharge of stones, and in turn improve their caused complications. EPVL has been developed for this purpose and remained as a major method of adjuvant therapy. This device is composed of a fixed vibrator, a hand-held vibrator, and a tiltable bed. The harmonic vibration generated by the two vibrators acts on the stones together, which can reduce the friction between the ureter and the stones and loosen and promote the discharge of stones. The therapeutic effect of EPVL has been verified in a number of RCTs. This technique can significantly improve the SFR after SWL and RIRS, without serious complications reported in the current study. 14 –19
GSF is a bone gap of anatomical window, in which part of the distal ureteral can be easily seen. To this end, we took advantage of this bone gap and used it as a path of shock wave for avoiding interference of sacroiliac joint. The prone position is a safe position and has been widely used in SWL for the treatment of DUC. 20 –22 Meanwhile, patients always have a stronger sense of urination in the prone position than in the supine position, which can further promote discharge of stones. 23
SSD is an important factor that affects the efficacy of EPVL. Longer SSD usually leads to more vibration wave attenuation. SSD of abdomen is usually longer than that of the buttocks, which is more obvious in obese patients. 24,25 Therefore, a use of this bone gap can effectively reduce loss of vibration waves in the transmission process. When patients undergo EPVL, we will apply pressure to the main oscillator to further reduce the distance between the main oscillator and stones to decrease attenuation of the vibration wave and achieve better effects. However, this can also cause patient discomfort, especially when taking transabdominal treatment. In this study, we found that the comfort resulting from these two methods was statistically different and patients were more willing to accept the path through this bone gap.
Renal colic is the most common reason for patients with urinary stones to see a doctor. Obstruction caused by stones can trigger muscle spasm of the ureter, and in turn colic. In addition, it can induce edema of the ureteral mucosa through mechanical stimulation, and this process usually occurs within 24–48 hours of stone obstruction, 26 followed by a significantly reduced expandable area. 27 Therefore, timely treatment of the stones can allow the stones to be discharged as soon as possible. In this study, we also found that Group A had significantly reduced episodes of renal colic as well as the need for analgesics than other groups. Meanwhile, although Group B and Group C have the same number of renal colic, the former has less analgesic needs than the latter. Moreover, the SFS observed in Group A was significantly elevated than that observed either in the Group B or C, although such a gap decreased with a longer period of time.
There are certain limitations in our study. First, we did not follow up all patients with CT, which may cause some errors in the judgment of patients with residual stones. Then, our hospital being a sole study site and limited sample size in this study. In the future, we will seek off-campus collaborators to conduct independent studies to validate our results. Furthermore, a prolonged follow-up is needed to assess long-term effects.
Conclusion
In conclusion, our study shows that EPVL through GSF is a safe and effective approach for treatment of DUC. It is a noninvasive method with a high degree of comfort and easier implementation in clinical applications. Our continued study is to conduct a larger multicenter prospective study to further corroborate our conclusions.
Compliance with Ethical Standards
All procedures conducted in studies with participants involved complied with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards, and with the ethical standards of Nanjing Jiangning Hospital.
Informed Consent
All individual participants involved here provided informed consent.
Footnotes
Author's Contributions
J.-L.L: Project development. S.Z. and C.-P.J.: Data collection. Z.-H.X., Q.-L.T., and H.W.: Data analysis and article writing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No specific grant was received for this study from any commercial or not-for-profit sectors and public funding agency.