
Abstract
Introduction:
Flexible ureteroscopy (fURS) is a one-person surgical technique, limiting trainees' ability to practice intraoperatively. Although well suited for simulation training, few existing fURS simulators can accurately reproduce complex renal collecting system anatomies. We developed an anatomically accurate fURS simulator using three-dimensional (3D) reconstruction of CT urograms and 3D printing technology to address this need.
Materials and Methods:
Patient-specific CT urograms were used to create 3D reconstruction of the renal collecting system using Slicer™. 3D models were modified using Blender™. Hollow, elastomer kidney models were created using an Objet 3D™ printer. To test and evaluate the new fURS simulator, 25 volunteers were recruited (5 novices, 13 residents, and 7 urologists). Participants were asked to explore the model with fURS and were evaluated on their ability to deduce its 3D anatomy, their ability to navigate to prespecified calices, and their time to task completion. Furthermore, participants were asked to compare the anatomical model with existing fURS benchtop models (Cook Medical™ and Limbs & Things™) on several criteria, including internal visualization, tactile feedback, and overall functional and teaching fidelity, in a survey.
Results:
We were able to create a fURS simulator that accurately replicates anatomically complex renal collecting systems. In exploring the model, we noted that unlike staff urologists, novices and residents often completely missed lower pole calices. A survey comparison between our simulator and comparable benchtop simulators revealed consistently better ratings of our simulator on all criteria (p < 0.05).
Conclusions:
We were able to create an anatomically accurate fURS simulator that provides a more realistic scoping experience. Preliminary testing revealed that trainees will benefit from this simulator, particularly with respect to learning how to navigate challenging collecting systems.
Introduction
Flexible ureteroscopy (fURS) has become the treatment of choice for small kidney stones since its technological advancement and refinement in the past two decades. 1 To utilize the full potential of fURS, a surgeon completes a large number of procedures during which he/she gains competence and comfort in precise and efficient maneuvering of the ureteroscope. 2,3 Given that fURS is usually performed by one surgeon, integrating trainee practice can be challenging during difficult cases. Furthermore, pressure to reduce surgical time, resident work hour restrictions, and an increasing number of trainees can potentially lead to inadequate direct surgical exposure to fURS to gain competency by the end of residency training. 4 Surgical simulation promises to address these shortcomings and can add value to training, particularly for the most junior residents as they are first exposed to fURS. 5
Several types of fURS simulation platforms are available, including benchtop, animal, cadaveric, and virtual reality (VR) systems. Benchtop models are inexpensive, but typically have the disadvantage of being less realistic. 1,2 Animal and cadaveric models are mainly limited by cost, reusability, and personnel requirements. While VR is a promising field, VR simulators continue to lack tactile feedback and tend to have high purchase costs. 3,6
Three-dimensional (3D) printing technology has been recently utilized in surgical simulation and model design. 7 When combined with 3D reconstruction of axial imaging, it provides an alternative, inexpensive, and reproducible method for capturing various patient-specific anatomical features that can significantly improve simulation platforms. The objective of our study was to create a high-fidelity and easily accessible, 3D, benchtop fURS model that can reproduce realistic challenging anatomies of the renal collecting system (such as sharp infundibulopelvic angles and spidery complex collecting systems) at a reasonable cost. Our focus was on providing a complex and realistic anatomy that allows trainees to advance their skills in collecting system navigation and flexible ureteroscope handling. Using this technique, we created various CT-based models that can be easily interchanged to allow residents to practice on a wide variety of renal anatomies.
Materials and Methods
Development of the 3D anatomical model
After informed consent, patient-specific CT urograms were utilized to reconstruct 3D renal collecting system anatomies using Slicer™. 3D models were then modified using Blender™. Hollow elastomer kidney models for fURS were created using an Objet 3D™ printer. Our model uses a rubber-like polyjet material, Agilus30™, which is distensible, durable, and allows smooth manipulation of the flexible ureteroscope. Multiple kidney models with varying anatomies were created using this method. These models can be mounted and interchanged on a custom-made simulation platform and can be navigated with the use of any flexible ureteroscope. One model with complex anatomy (multiple out-of-plane upper, inter, and lower pole calices, as well as a sharp takeoff to the lower pole) was chosen for further testing of the simulation platform, as described below.
Setup of the 3D benchtop model
The renal model was housed and submerged in a waterproof 3D printed enclosure to hide the appearance of the collecting system (Fig. 1). The model included the renal internal anatomy, ureteropelvic junction, and upper ureter. The upper ureter was connected to a ureteral access sheath as the ureterovesical junction and bladder were not simulated in the current model. Pressurized irrigation was simulated using a peristaltic pump with dampening to mimic intraoperative pressurized IV bags.
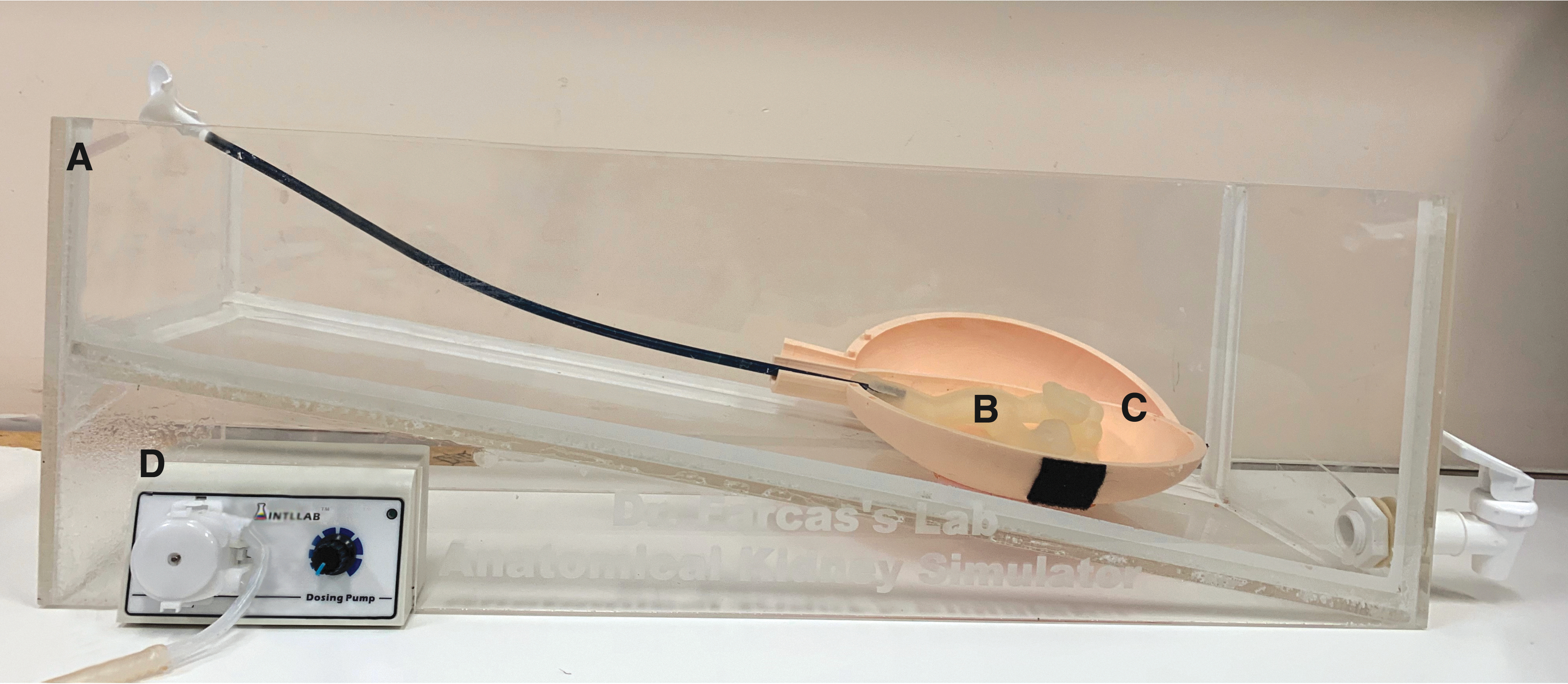
Preliminary platform used to test the anatomical model.
Evaluation of the anatomical fURS model
Twenty-five participants were recruited to test the device (5 novices, 13 urology residents, and 7 urologists). Novices were either medical students or technicians who may have had exposure to fURS through observation but had never performed fURS. The intermediate group consisted of current University of Toronto urology residents (PGY 1–4) with variable fURS hands-on experience (self-reported 1–20 fURS procedures). The expert group consisted of seven urologists who were either attending staff urologists or endourology fellows at St. Michael's Hospital (self-reported fURS cases >50). All data collected were deidentified, and blinded analysis was performed by two endourology staff experts. Video collection of the endoscopic view only (without any view of the participants and without voice recording) was also used to aid in analysis. Participants were asked to navigate the model and perform three tasks: draw the collecting system anatomy from memory, accurately navigate to predefined calices and fill out a comparison survey between the new model and a benchtop model (Cook Medical™).
Task 1—Exploration of the model and drawing of its internal anatomy
Participants who did not have prior knowledge of the model's structure were asked to freely explore the model using a flexible ureteroscope (Storz™ Flex-X2, Tuttlingen, Germany) and then draw the anatomy of the collecting system from memory. During this task, the external form of the 3D model was not visible and there was no access to fluoroscopy. Participants were not restricted in the time taken for both the exploration of the model and drawing of the anatomy. However, they were limited to one trial. Participants could use any schematic they wished to delineate the number of upper poles, interpolar, and lower pole calices, as well as their orientation (anterior, posterior, and lateral). A 3D drawing was not required. Participants could use simple line drawings and point out anterior–posterior calices using the letters A and P. Participants were also awarded the opportunity to verbally describe their drawing to the tester to provide clarification. Data collected included participant training level, time to task completion, anatomical drawing, tester notes, and a silent endoscope view videorecording. Drawings were rated by two blinded senior endourologists. Scoring was based on the participant's ability to accurately identify the upper, inter, and lower pole calices and their anterior–posterior configuration. The drawings and video review from the endoscope were used for scoring. Results were analyzed using one-way analysis of variance (ANOVA) for each component and, if statistically significant, a post hoc t-test was performed to compare between groups.
Task 2—Accurate navigation to a specific calix
Participants were shown the model anatomy and were asked to navigate to preselected calices in our anatomical model and in a comparable model by Cook Medical. The Cook Medical model was previously studied and has demonstrated face, content, and construct validity in addition to improving short-term technical skills in junior-level urology trainees. 8 This task helped delineate participants' ability to use the flexible ureteroscope and intrarenal orientation. Data were analyzed using one-way ANOVA and post hoc t-tests.
Task 3—Comparison survey
During a resident ureteroscopy course, participants had the opportunity to use the three simulation platforms (Limbs & Things, Cook Medical, and our anatomical model) for a similar task. A survey was conducted to compare the experience with each model with respect to internal visualization; tactile feedback; and overall functional and teaching fidelity. An overall rating of the three models was obtained. Statistical analysis was performed using the Kruskal–Wallis test and post hoc Mann–Whitney U test. Our study had 12 participants for the Limbs & Things model and 35 participants for the Cook Medical and anatomical models.
Results
Using 3D reconstruction of CT urograms, along with 3D printing technology, hollow, 3D, elastomer kidney models with real patient internal renal anatomy were created (Fig. 2). These models are mounted interchangeably on a custom-made, benchtop, ureteroscopy simulation platform. The simulation platform is used with closed-loop irrigation to replicate a realistic fluid dynamic environment. One representative model with complex anatomy (multiple out-of-plane upper, inter, and lower pole calices, as well as a sharp takeoff to the lower pole) (Fig. 3B) was chosen for further testing of the simulation platform.
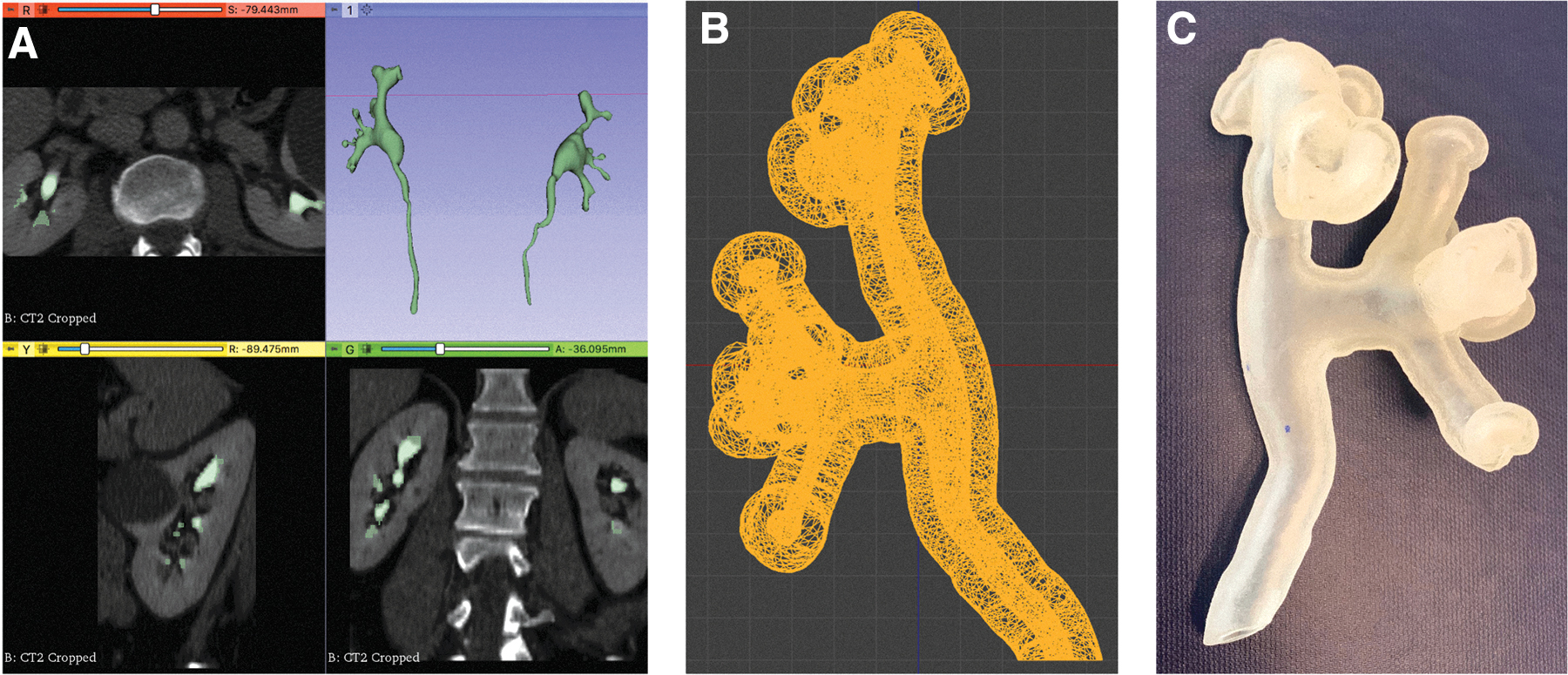
Development of a 3D renal collecting system.
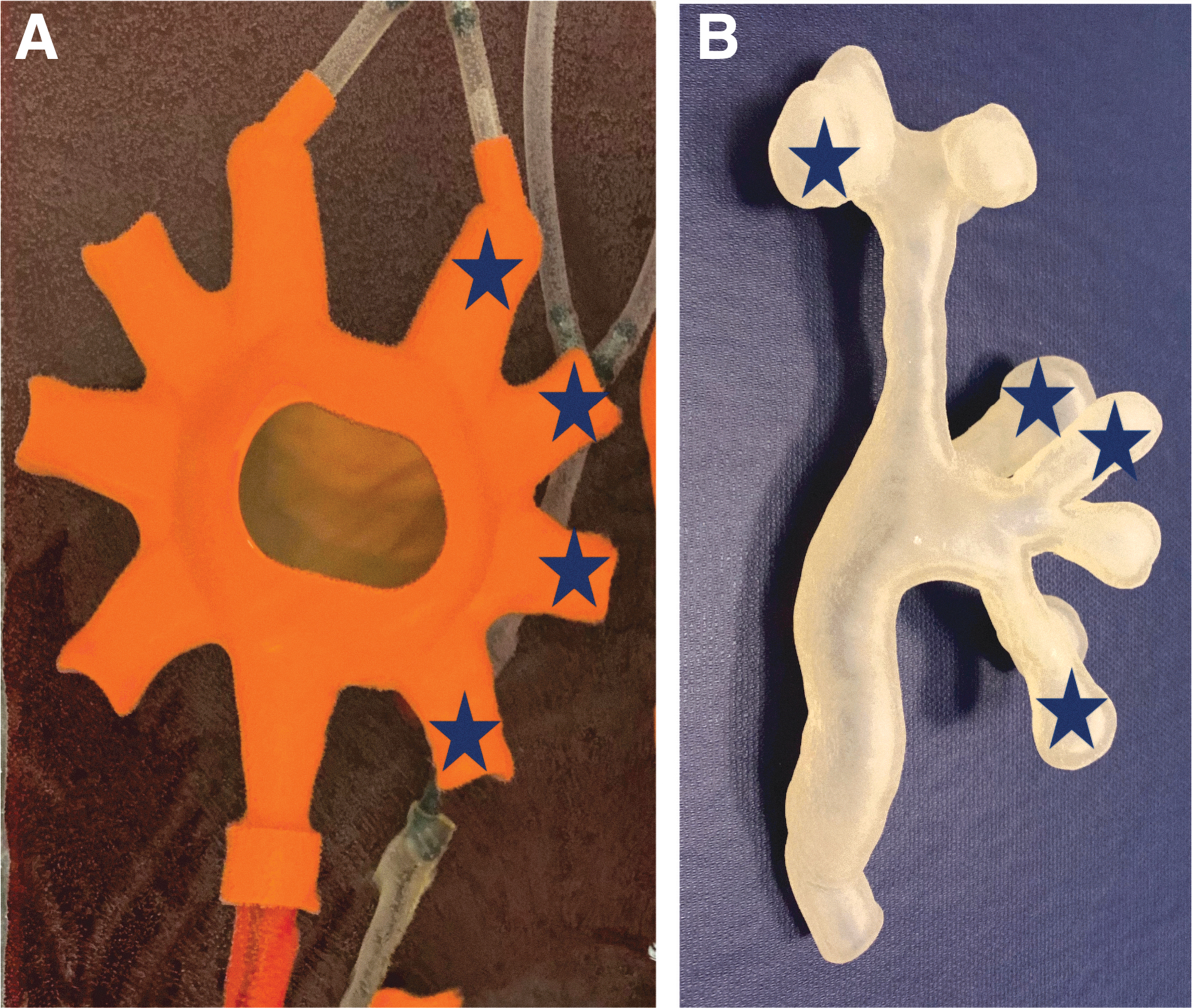
The Cook Medical™ fURS model
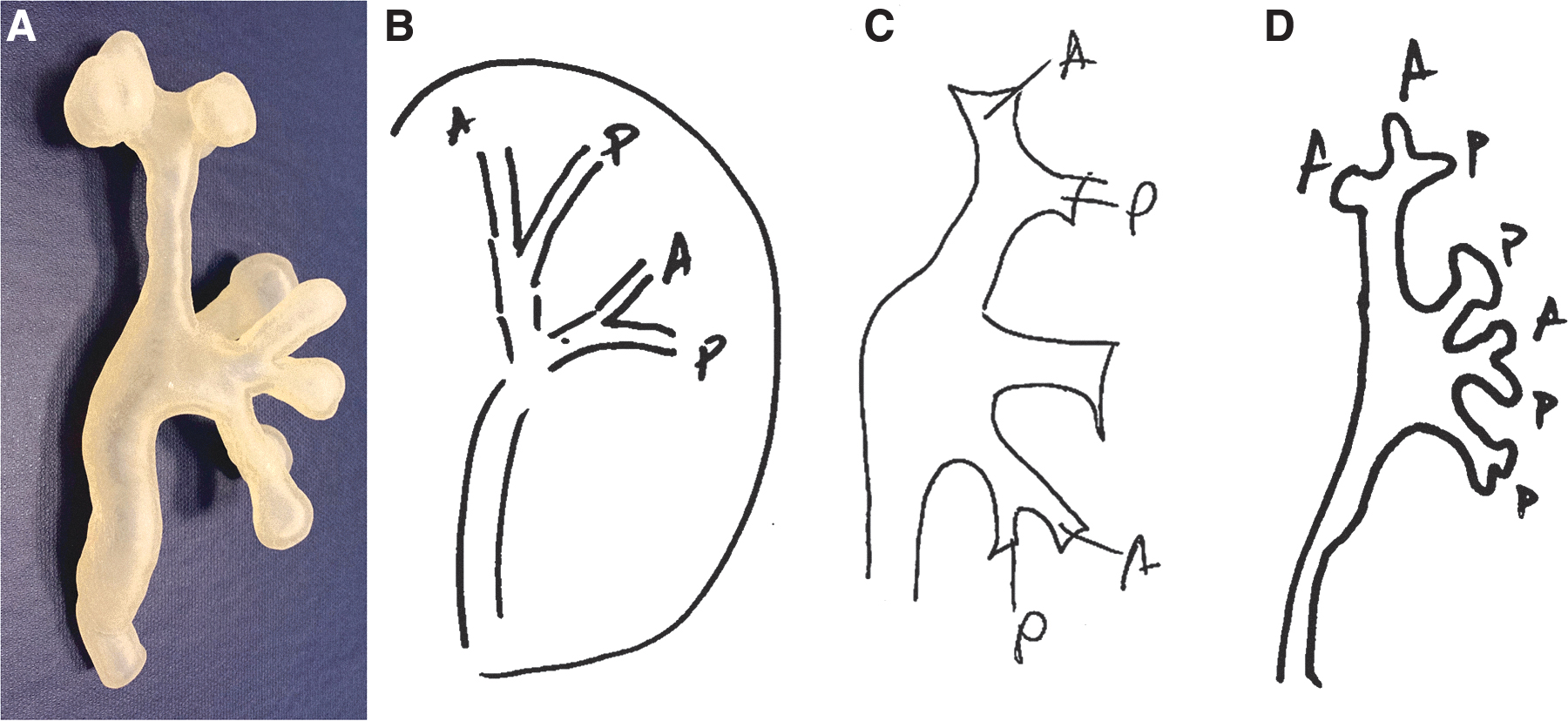
For Task 1, participants were asked to navigate the new model collecting system (without a priori knowledge of its anatomy or access to fluoroscopy) until they were satisfied that they can draw the collecting system anatomy from memory. For this task, there was a clear correlation between participant expertise level and accurate identification of major calices. In addition, we noted that most novices and residents missed the takeoff to the lower pole calices and thus failed to identify these calices. The effect of expertise level on accurate anatomical drawing of the collecting system was statistically significant [ANOVA F(2,22) = 11.6, p = 0.0004] (Figs. 4 and 5). The post hoc t-test showed significant differences between all groups (p < 0.05). Although there appears to be a trend toward an inverse relationship between exploration time and expertise level, the result showed a nonsignificant effect of the expertise level on the time needed to explore the model [ANOVA F(2,22) = 2.39, p = 0.11] (Fig. 5).
Anatomical model
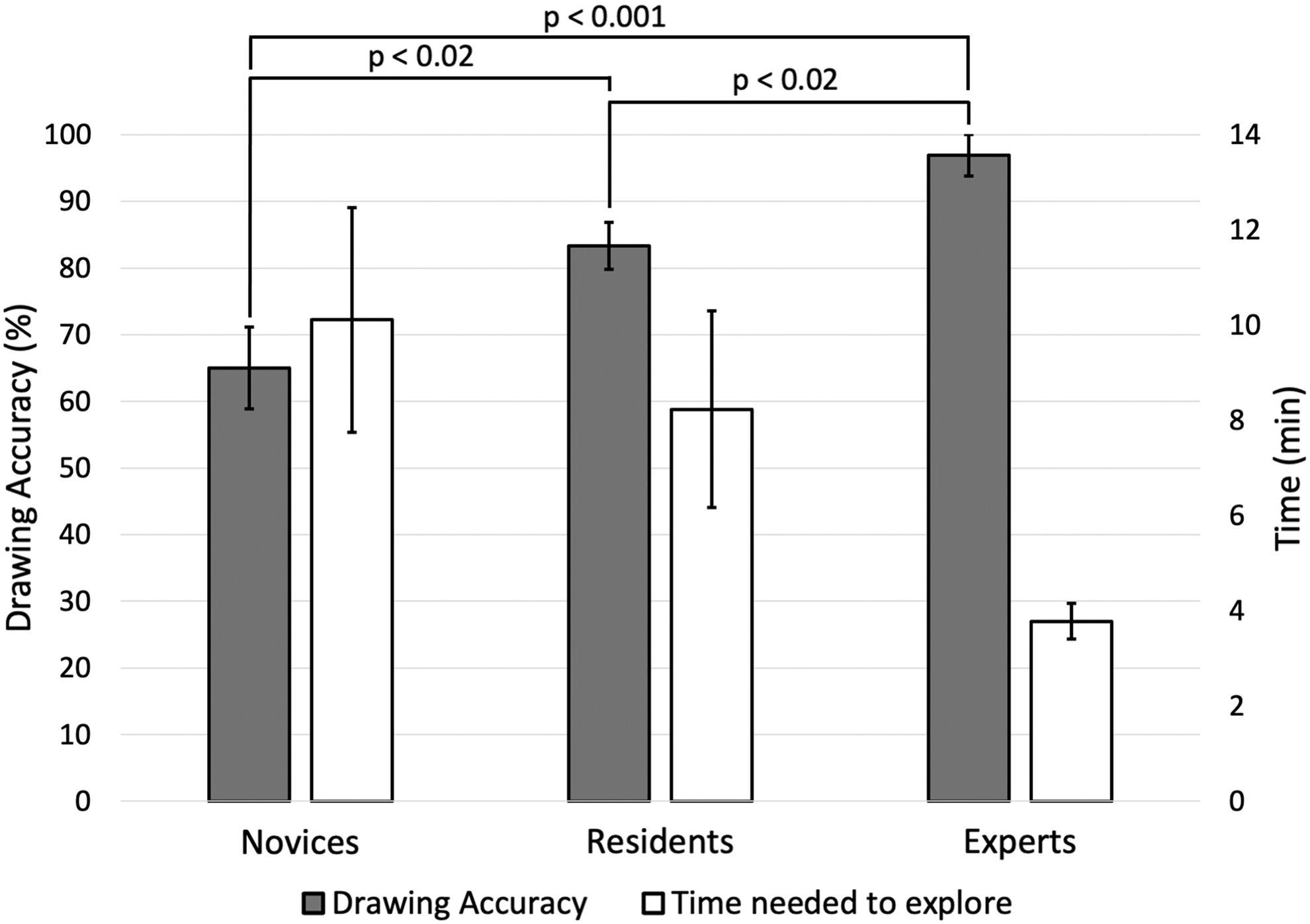
Accuracy of identifying major calices (without prior knowledge of renal anatomy) in the anatomical model, and the time each group took to explore the model (Task 1).
For Task 2, participants were asked to navigate to four specific preidentified calices (one upper pole, two interpolar, and one lower pole) in the anatomical and the Cook Medical models. The effect of expertise level on correctly identifying these preselected calices was significant in the anatomical model [ANOVA F(2,22) = 4.93, p = 0.017] (Fig. 6). The post hoc t-test showed significant differences in correct calix identification between novices and experts and residents and experts (p < 0.05), but not between novices and residents. The effect of expertise level for this task was not significant in the Cook Medical model [ANOVA F(2,22) = 1.22, p = 0.31] (Fig. 6).
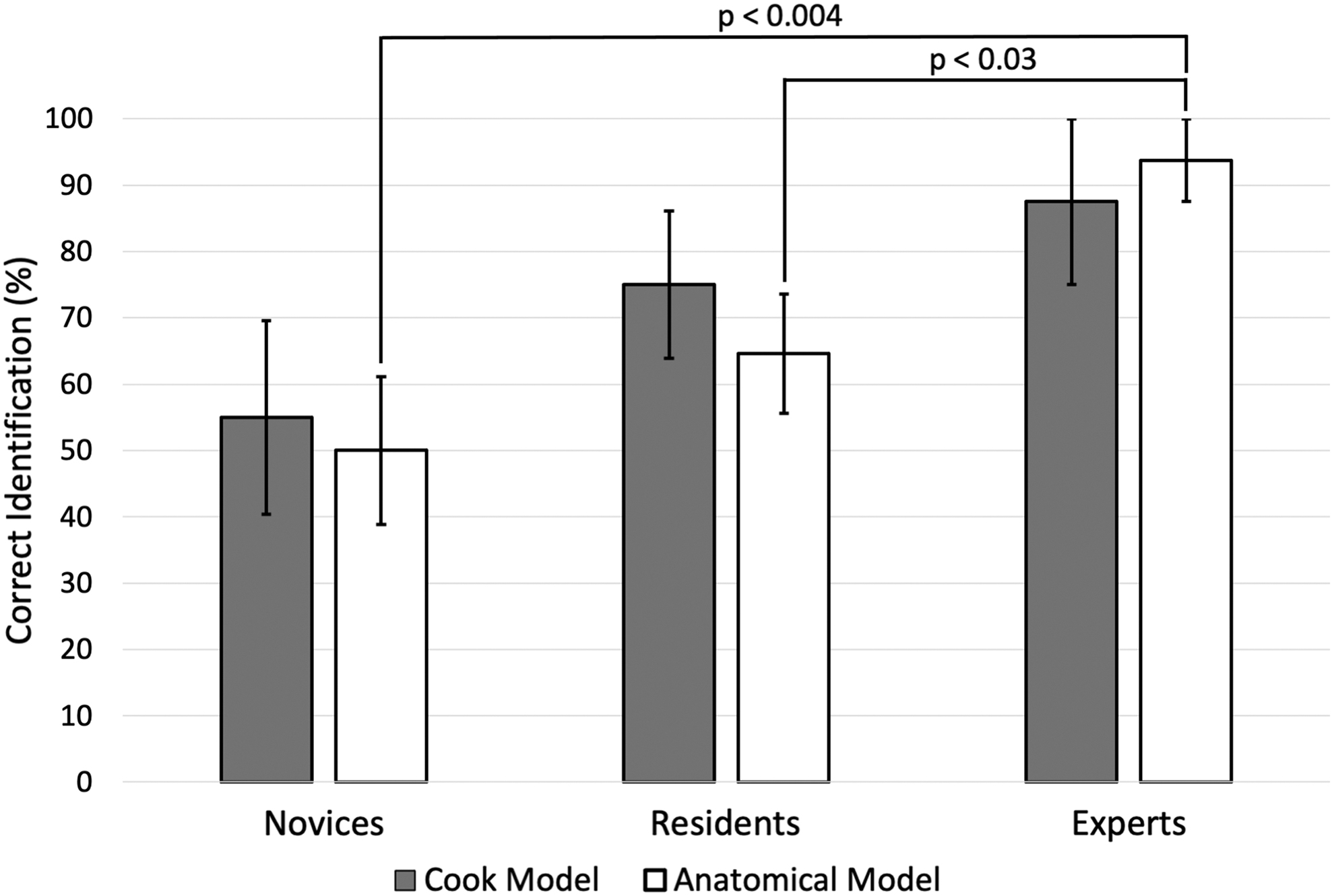
Comparison of correctly identified calices in each model among the three expertise groups (Task 2, Cook Medical vs anatomical model).
Participant survey results revealed that the anatomical model consistently scored higher in all areas surveyed compared with the Cook Medical and Limbs & Things models (p < 0.05). Aspects evaluated included internal visualization; tactile feedback; anatomic realism; functional fidelity; and usefulness in teaching and assessment. When asked about their overall impression, participants rated our model preferably over the Cook Medical and Limbs & Things models with statistical significance (Figs. 7 and 8 and Table 1).
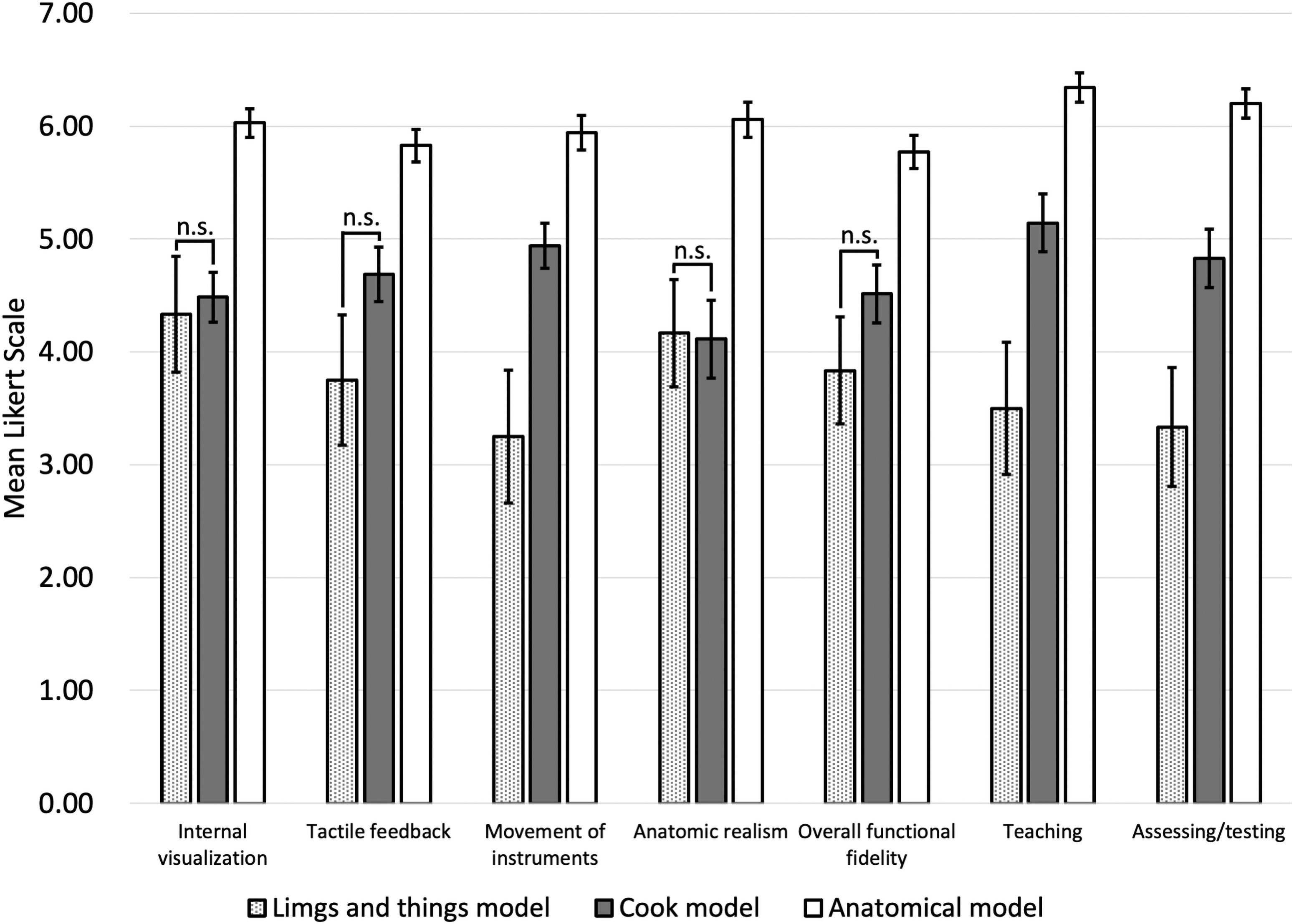
Mean Likert scale ± standard error of Limbs & Things™ vs Cook Medical vs anatomical fURS models. All groups showed significance between the models except when noted n.s. Scale: 1 = poor and 7 = excellent. n.s. = not significant.

Mean Likert scale ± standard error of Limbs & Things vs Cook Medical vs anatomical fURS models on the overall rating of the simulator models. Scale: 1 = useless and 10 = amazing.
Comparison of Ureteroscopic Experience with the Limbs & Things and Cook Medical Models vs the Anatomical fURS Model
Data are presented as mean ± standard deviation.
Mann–Whitney U test.
Cook = Cook Medical™; fURS = flexible ureteroscopy; L&T = Limbs & Things™; n.s. = not significant.
Discussion
Due to the ever-growing constraints on surgical training, there is an opportunity for supplementary education outside the operating room. Legal and ethical considerations as well as ever-increasing pressure on operating room efficiency and quality assurance may make the operating room less desirable for primary teaching or evaluation of surgical skills. Surgical simulators have the advantage of not putting patient safety and health care resources at risk and offer a unique standardized venue for both training and assessment of surgical skills. 9 –11 In addition, simulation environments offer the opportunity to collect distinct quantifiable and reproducible metrics (such as time, precision, motion, and force analysis parameters), which can provide meaningful feedback information to the surgical trainee, and objective metrics for potential evaluation by teachers. 12 Benefits of surgical simulation are well established, and in the coming years, it is expected that more and more surgical programs will integrate simulation-based surgical training into formal surgical education curricula.
Single-operator surgical procedures, such as fURS, are particularly well suited for simulation training as there may be limited opportunity for junior trainees to practice intraoperatively, especially during challenging cases. To this end, many simulation platforms for fURS have been developed, each with specific benefits and trade-offs. While current benchtop fURS models are inexpensive, they have been criticized for their lack of realistic anatomical complexity. Conversely, while VR simulators can provide such complexity, their widespread use has been limited by high costs and lack of tactile feedback. While cadaveric or live tissue models can offer both anatomic and tactile realism, they are subject to cost, sustainability, ethical, and exposure risk limitations.
In this study, we have drawn upon recent advancements in 3D printing technology (particularly for hollow elastomer models) and the wide availability of CT imaging to create an anatomically realistic, benchtop ureteroscopy simulator. This model has many advantages. It is low cost (estimated total manufacturing cost is less than $200 for simulation platform and kidney models). It uses a standard flexible ureteroscope, allowing trainees to practice and gain comfort with the same tool they would use intraoperatively. The kidney models can be freely interchanged, allowing trainees to practice on a variety of challenging patient anatomies (sharp infundibulopelvic angles and complex or spidery collecting systems, etc.). The system can be connected to closed-loop fluid irrigation, thus replicating realistic intrarenal fluid dynamics. The material of construction of the renal model is distensible and allows for a degree of dilation of the model as would be seen in real life. This property may potentially allow this model to be used for studies on intrarenal pressure, although further material property data are required at this time. The model can also be used to teach lasering or basketing of renal stone fragments from difficult locations, such as behind caliceal ridges or around the rim of prominent papillae. Furthermore, this basketing practice can occur under realistic fluid recirculation zones and dynamics, which are dictated by the internal renal anatomy.
In this study, we were further able to demonstrate the advantage of a more challenging fURS platform for resident training. While experts were able to accurately identify and draw out the collecting system anatomy from memory, residents and novices typically missed the sharp takeoff to the lower pole and thus never identified the lower pole calices in the new model (often mistaking the interpolar calices as lower pole calices). Compared with an existing benchtop fURS model (Cook Medical) (for which all upper, inter-, and lower pole calices lie in one plane and equidistantly), the anatomical model was more challenging to accurately navigate for the identification of predefined calices. Experts were significantly better at identifying these calices compared with both residents and novices in the anatomical model, while no difference was seen among groups for the Cook Medical model. This clearly demonstrates a need for further resident training on a more anatomically realistic and challenging fURS platform.
In a survey comparing the simulation experience between the three benchtop models, the anatomical model scored higher in all aspects surveyed, including anatomic realism and internal visualization. We believe the model provided better internal visualization due to its material of construction, which provided good light penetration and minimal refraction. Tactile feedback was also more realistic as the anatomic model was distensible and allowed a smooth and soft scoping surface, as opposed to a firm plastic model.
We recognize that there are multiple limitations to this study. A small number of participants were recruited using convenience sampling, limiting recruitment to volunteers who are affiliated to the University of Toronto or St. Michael's Hospital. Volunteers were arbitrarily grouped based on their level of training. While the current study serves as an initial proof of concept for an anatomical benchtop simulator, further rigorous validation studies are required to determine both the face and content validity of this simulator, with the goal of translation of trainee skills to the operating room. Furthermore, we are in the process of extending the model to include the lower urinary tract (urethra, bladder, ureterovesical junction, and lower ureter) to provide an even more realistic intraoperative experience through this simulation platform.
Conclusions
We were able to create an anatomically accurate, benchtop fURS simulator using patient CT scans, which provides a more realistic ureteroscopy experience. Preliminary testing reveals that trainees will likely benefit from this simulator by learning how to navigate challenging and complex collecting systems in a safe and cost-effective simulation environment.
Footnotes
Acknowledgments
The authors thank all surgeons, fellows, residents, and students who contributed their time to this study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Abbreviations Used
Appendix A1
Simulation Experience Questionnaire
| How would you rate this flexible ureteroscopy model with respect to: | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 = Poor | 2 | 3 | 4 | 5 | 6 | 7 = Excellent | ||||
| Internal visualization | ||||||||||
| Tactile feedback | ||||||||||
| Movement of instrument | ||||||||||
| Anatomic realism | ||||||||||
| Overall functional fidelity | ||||||||||
| Usefulness in teaching ureteroscopy skills | ||||||||||
| Usefulness in assessing and testing ureteroscopy skills | ||||||||||
| 1 = Useless | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 = Amazing | |
|---|---|---|---|---|---|---|---|---|---|---|
| Overall rating |