
Abstract
The aim of this article is to illustrate a step-by-step guide to placement of Resonance® metallic ureteral stent (Cook Medical, Bloomington, IN) for management of malignant or benign ureteral obstruction. In this article, the steps of operating room setup, patient positioning, gaining access to the upper urinary tract, and endoscopic and fluoroscopic placement of a Resonance ureteral stent are described.
Featured Video
https://stream.cadmore.media/player/d470e9cd-8add-45f6-a82e-bf3dbd59d98e
Indications
Ureteral stenting allows the kidney to drain when normal flow is compromised by obstruction. Obstruction can be categorized as benign or malignant. Obstruction of intrinsic etiology originates within the urinary system and can include stone, stricture, or genitourinary malignancy. Extrinsic causes of ureteral obstruction compress the ureter from outside the urinary tract and can be malignant (gynecologic or gastrointestinal tumors or lymphadenopathy) or benign (crossing vessels or retroperitoneal fibrosis). Stents may also be placed across an anastomosis to facilitate continued drainage while the surgical site heals. Examples include traumatic or iatrogenic injury, pyeloplasty, ureteroureterostomy, or renal transplant.
Percutaneous nephrostomy (PCN) tube placement, an alternative to ureteral stents, involves creating a new tract through the back into the kidney and requires management of an external drainage bag. One of the advantages to this procedure is it does not require general anesthesia. However, it usually requires the presence of hydronephrosis to facilitate placement, and anticoagulation must be held to prevent bleeding complications. PCN does not significantly improve survival or quality of life in advanced disease, 1 and studies have shown that neither PCN nor ureteral stents are superior in relieving obstruction and infection. 2
In certain cases, stents are temporary interventions until an underlying pathology can be treated or resolves (e.g., stone surgery). However, there is not always a simple or definitive solution, and the stent must stay for a prolonged time period. This includes patients who are poor operative candidates who cannot undergo a necessary procedure, on critical anticoagulation that cannot be safely held, or who have an untreatable disease process.
Metal stents have multiple benefits compared with polyurethane or silicone materials. They require less frequent exchanges and ostensibly have lower failure rates. 3 In one single-center experience, there was a 96% success rate with resonance stents, and median dwell time was 19.5 months in benign vs 12 months in malignant obstruction. 4 Another study found a mean increase in stent duration of 4 months compared with prior polymeric stent failures. 5 Whereas nonmetallic stents are exchanged on a 3-month schedule, metal stents can remain in place for up to 12 months. This means fewer invasive procedures for the patient, more convenience, and lower cost over the longer term. 6
Preoperative Preparation
Preoperative evaluation should include laboratory testing and imaging. Baseline renal function should be obtained to monitor for improvement after intervention if kidney injury is suspected. Urinalysis and culture should be done to identify and appropriately treat infection. Infection in the setting of obstruction is a urologic emergency and should expedite the time to decompression. Imaging demonstrating hydronephrosis may be adequate if the indication is emergent, otherwise CT is preferred to identify cause, location, and severity of obstruction. Knowledge of the patient's use of anticoagulation can also help determine initial modality of decompression; it is a relative contraindication to percutaneous diversion because of higher risk of bleeding. Appropriate counseling is imperative so patients are aware of the associated risks. These include bleeding, infection, injury to the urethra, bladder, ureter, or kidney, stent discomfort, lower urinary tract symptoms, stent failure, inability to place stent, and need for further procedures.
Patient Positioning and Operating Room Setup
The patient should be placed in dorsal lithotomy with pressure points padded appropriately to mitigate risks of positional nerve related injury. The C-arm can be arranged on one side of the patient with ipsilateral arm tucked, and the endoscopic and fluoroscopic monitors on the contralateral side (Fig. 1).

Patient positioning and operating room setup.
Surgical Steps
Cystoscopy, deployment of guidewire alongside existing stent if one present
A 21F rigid cystoscope with 30° lens may be used to enter the bladder. A straight sensor wire with 0.038″ diameter is used to cannulate the ureteral orifice with or without the aid of a 5F open-ended catheter for guidance. Fluoroscopic imaging should confirm the wire positioned within the renal pelvis. If there is a pre-existing stent, a flexible grasper is used to grasp the distal curl of the stent and remove it from the collecting system while having a guidewire deployed alongside the stent. Alternatively a flexible cystoscope can be utilized for this step (Fig. 2).
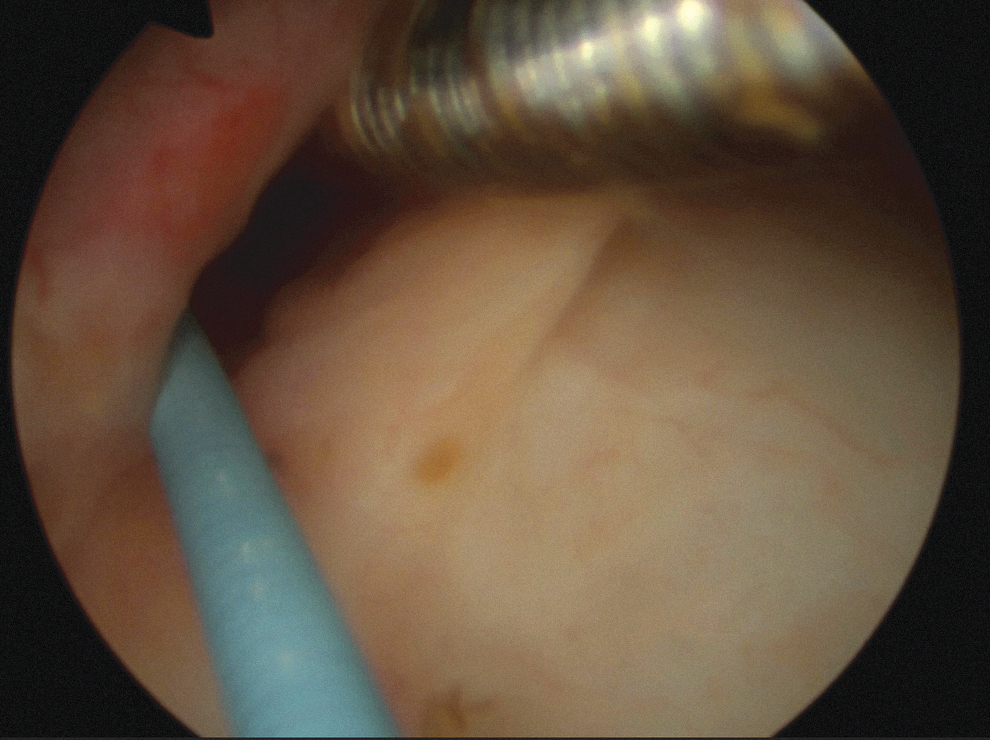
Deployment of guidewire.
Retrograde ureteropyelogram
A retrograde ureteropyelogram should be performed after wire placement (and before stent removal if applicable). Contrast injected through the cystoscope to opacify the upper tract is used to confirm the location and degree of obstruction (Fig. 3).
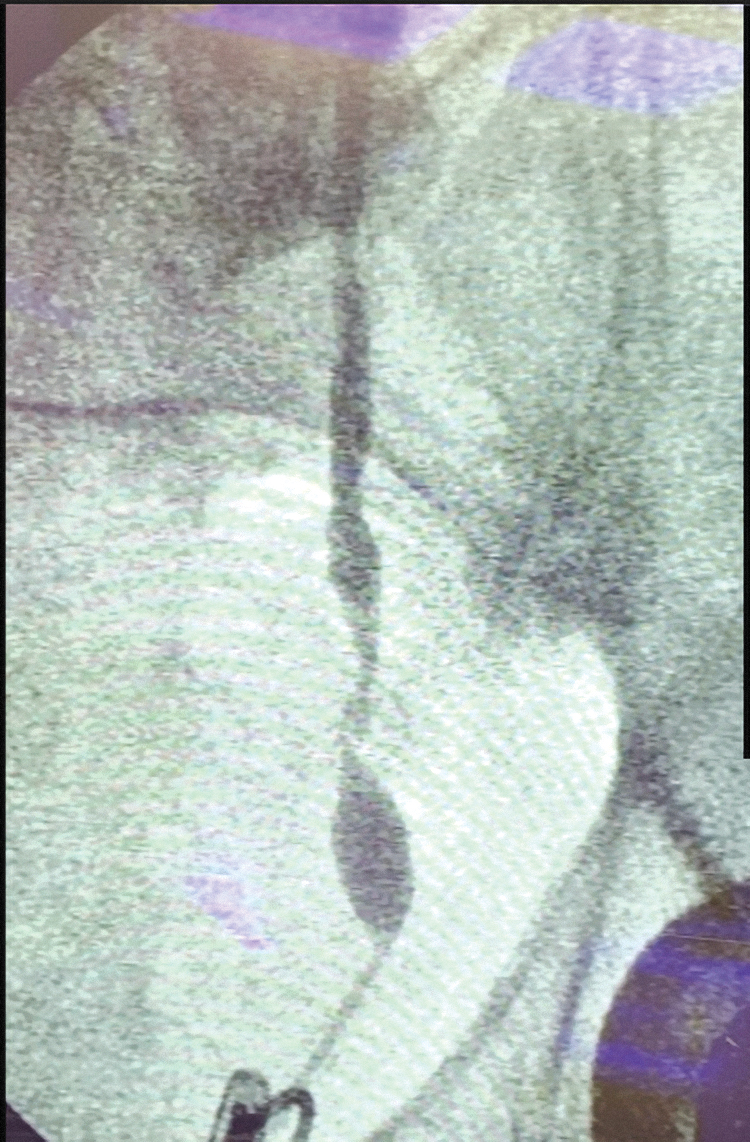
Retrograde ureteropyelogram.
Placement of obturator and sheath
The sheath and introduction catheter are advanced over the guidewire under both endoscopic and fluoroscopic guidance. There is a radio-opaque tip to the sheath that should be advanced no further than the ureteropelvic junction to avoid perforation of the parenchyma (Fig. 4).
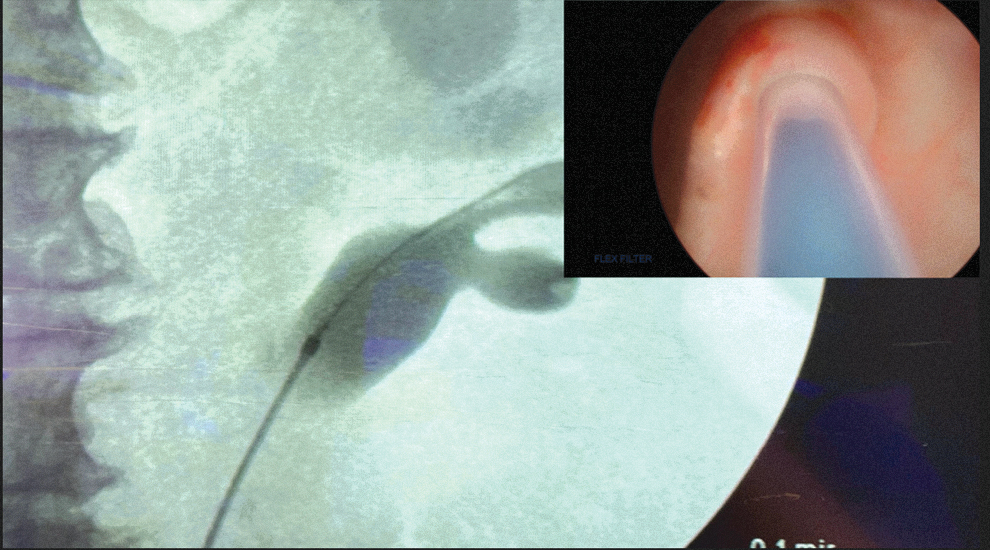
Placement of obturator and sheath.
Removal of obturator and wire and placement of resonance stent
The introduction catheter is removed. The resonance stent is then introduced through the clear sheath. The introduction catheter is then used to push the stent until both the pusher is seen at the bladder neck and proximal end of the stent is seen above the ureteropelvic junction under fluoroscopy. The sheath and introduction catheter are then removed in succession to deploy the stent (Fig. 5).
Deployment of resonance stent.
Postoperative Care
Stent placement can be done on an outpatient basis. In cases where patients may suffer from an active infection, renal injury, or other issues related to the obstruction or its underlying cause, they may require further inpatient stay and treatment. Patients can be monitored for resolution of symptoms (fever, pain, nausea/vomiting) and trending creatinine, with interval imaging to assess stent position and resolution of hydronephrosis. There is no standard protocol as the patient and pathology are heterogeneous.
Troubleshooting
In the event of stent encrustation, extracorporeal shockwave lithotripsy, ureteroscopy, and laser lithotripsy can be performed. 7 A guidewire can also be inserted to uncurl the coils or a sheath can be passed over the stent. Care should be taken not to pull too hard when resistance is met because of the risk of ureteral injury and stent damage. Stent removal should be done under fluoroscopy to ensure safe removal. Stent duration has the greatest impact on risk of encrustation. If the stent is found to be encrusted, consideration should be given to increasing the frequency of stent exchange.
Clinical Outcomes and Complications
Outcomes for chronic stenting vary widely given the variety of stent types and etiology of obstruction. Success rates for stent placement range from 85% to 100% for combined malignant and benign obstruction. 6 Stent failure may occur in the form of subjective complaints (flank pain, lower urinary tract symptoms) or objective (persistent hydronephrosis, acute kidney injury, and encrustation). It is reported that 35% to 50% of plastic stents fail. These traditional stents may fail because of external compression or secondary to encrustation. In one study, 41% of patients had their metallic stent removed at median of 5 months because of bothersome symptoms, infection, obstruction, or migration. 8 There are better results for metal stents compared with polymeric stents, with late failure rates of 0% to 44% and 16% to 44%, respectively. 6 One study reported stent failure from an extrinsic source in 44% to 58%. 9 Another study demonstrated stent failure in 40.6% of patients; in those with metastatic cancer, 32.2% were deceased at a mean of 5.8 months. 10
In some patients with poor prognosis, rapid progression, and no plan for systemic therapy, then it may be prudent to avoid intervention altogether. This decision is best done with shared decision-making model (patient, family, and provider). Survival in malignant ureteral obstruction in some series after decompression is generally <12 months. 11 Risk stratification tools have been created to identify patients as good, intermediate, or poor risk using factors such as cancer origin and prestent renal function. 12
One of the most feared complications with long-term ureteral stents is ureteroarterial fistulas. Ureteroarterial fistulas are rare occurrences however. 13 Mortality ranges from 10% to 38%. Risk factors include chronic indwelling stent, malignancy, abdominal, and pelvic surgery. The most frequently noted fistula is a connection with the common iliac artery. These patients present almost universally with gross hematuria, and there is potential for hemodynamic instability. Arteriography and ureterogram can be used to diagnose this complication. Treatment options include endovascular repair, open surgery, vascular bypass grafting, and even nephrectomy.
Footnotes
Patient Consent Statement
The author(s) have received and archived patient consent for video recording/publication in advance of video recording of procedure.
Author Disclosure Statement
R.S. is a consultant for Boston Scientific, Cook Medical, and Karl Storz. The remaining authors have no disclosures to declare.
Funding Information
No funding was received for this article.