
Abstract
Introduction:
Management of malignant ureteral obstruction (MUO) with ureteral stents remains a clinical challenge, often involving frequent stent exchanges attributable to stent failure or other urological complications. We report our institutional experience with ureteral stents for management of MUO, including analysis of clinical factors associated with stent failure.
Methods:
We performed a retrospective review of patients treated with indwelling ureteral stents for MUO in nonurothelial malignancies at our tertiary-care institution between 2008 and 2019. Univariate Cox proportional hazards analysis was performed to identify clinical variables associated with stent failure and stent-related complications. Stent failure was defined as need for unplanned stent exchange, placement of percutaneous nephrostomy (PCN), or tandem stents.
Results:
In our cohort of 78 patients, the median (range) number of stent exchanges was 2 (0–17) during a total stent dwell time of 4.3 (0.1–40.3) months. Thirty-four patients (43.6%) developed a culture-proven urinary tract infection (UTI) during stent dwell time. Thirty-five patients (44.8%) had stent failure. Twenty-two patients (28.2%) underwent unplanned stent exchanges, 23 (29.5%) required PCN after initial stent placement, and 6 (7.7%) required tandem stents. Ten (28.6%) patients with stent failure were treated with upsized stents, which led to resolution in seven patients. Stent failure occurred with 20/44 (45.4%) Percuflex™, 15/27 (55.6%) polyurethane, and 2/3 (66.7%) metal stents. In patients with ≥2 exchanges (N = 45), median time between exchanges was 4.1 (2.0–14.8) months. Bilateral stenting and history of radiation predicted UTI development. Median overall patient survival after initial stent placement was 19.9 months (95% CI 16.5–37.9 months).
Conclusions:
Ureteral stent failure poses a significant medical burden to patients with MUO. Better methods to minimize stent-related issues and improve patient quality of life are needed. Using a shared decision-making approach, clinicians and patients should consider PCN or tandem stents early in the management of MUO.
Introduction
Malignant ureteral obstruction (MUO) is a common complication of pelvic, retroperitoneal, and metastatic malignancies. In affected patients, ureteral obstruction causes significant morbidity and mortality, including pain, renal impairment or failure, and urinary tract infection (UTI). In such cases, obstruction may be because of extrinsic compression by primary or metastatic tumor, or by direct invasion of the tumor. The presence of MUO is an ominous sign and portends a poor prognosis, with median survival of affected patients ranging between 3 and 7 months. 1 –3
Historically, MUO was managed with surgical reconstruction. 4 However, the perioperative morbidity associated with invasive surgical approaches combined with the limited life expectancy of affected patients has led to a paradigm shift in treatment toward minimally invasive options. Current management of MUO involves urinary tract decompression with a ureteral stent or percutaneous nephrostomy (PCN), with the former often being the primary choice. However, the use of ureteral stents for MUO remains a clinical challenge, often requiring frequent stent exchanges because of stent failure or other urological complications. Up to half of patients initially stented cystoscopically for MUO go on to develop stent failure and ultimately require percutaneous drainage. 1,5
Herein, we report our institutional experience with the use of ureteral stents for the management of MUO and analysis of clinical factors associated with stent failure.
Materials and Methods
Upon Institutional Review Board approval, we retrospectively reviewed our prospectively maintained database of nonconsecutive patients who underwent primary cystoscopic retrograde ureteral stent placement for MUO between January 2008 and September 2018 at Barnes-Jewish Hospital/Washington University School of Medicine in Saint Louis, Missouri. Patients with urothelial malignancies or urinary tract anomalies, precluding retrograde stent placement, were excluded. Stent size and type were based upon surgeon preference.
Chart review was performed on all patients for demographics, comorbidities, primary diagnosis, preoperative and postoperative serum creatinine, location of obstruction, stent diameter and material, complications, UTI, stent exchanges, stent dwell time, stent failure, progression to PCN, and tandem stent placement. Baseline comorbidities were assessed using the Charlson Comorbidity Index. 6 Estimated glomerular filtration rate (eGFR) was calculated preoperatively, at the time of discharge, and at most recent follow-up using the Modification of Diet in Renal Disease equation. 7 The location of ureteral obstruction was determined by intraoperative retrograde pyelogram. Stent failure was defined as need for unplanned stent exchange, progression to PCN, or tandem stent placement attributable to hydronephrosis in the setting of acute kidney injury, infection, stent migration, or other complication. Conversion to PCN was recommended if retrograde ureteral stent placement was technically unsuccessful or did not appear feasible based on radiographic evidence of significant progression of tumor or adenopathy.
Statistical analysis was performed using R version 3.5.2. Data are presented as mean ± standard deviation (SD) or median (range). Univariate Cox proportional hazards analysis was performed to identify variables predictive of stent failure and UTI development. Kaplan–Meier estimated survival curves were generated for overall survival (OS). Statistical significance was defined by a p-value of <0.05.
Results
A total of 78 patients were identified, who met inclusion and exclusion criteria. Patient characteristics are summarized in Table 1. Mean (SD) age was 61.6 ± 12.9 years. Gynecologic cancers were most common (32.1%), followed by colorectal cancers (25.6%) and prostate cancer (19.2%). Mean serum creatinine before stent placement was 1.73 ± 1.2 mg/dL and decreased by 37% to 1.09 ± 0.52 mg/dL at the time of discharge, a median of 4 (0–23) days after stent placement. Forty-nine patients (62.8%) met diagnostic criteria for chronic kidney disease (CKD) before initial stent placement. A total of 45 patients (57.7%) had a history of radiation.
Patient Characteristics
BMI = body mass index.
The median (range) number of stent exchanges was 2 (0–17) during a median total stent dwell time of 4.3 (0.1–40.3) months. In patients with ≥2 exchanges (N = 45), median time between exchanges was 4.1 (2.0–14.8) months. Of the entire cohort, 35 patients (44.8%) experienced stent failure. Thirty-four patients (43.6%) developed a culture-proven UTI during stent dwell time. Twenty-two patients underwent unplanned stent exchanges. Reasons for unplanned stent exchange included recurrent or worsening hydronephrosis (72.7%), infection/urosepsis (13.6%), ureteral injury (4.5%), stent migration (4.5%), and ureteroiliac fistula (4.5%).
Ten patients requiring unplanned stent exchange were treated with upsized stents, which led to resolution in seven patients. Twenty-three patients (29.5%) required upgrade to PCN, whereas 6 (7.7%) required tandem stents after initial stent placement. All patients upgraded to PCN or tandem stents experienced resolution of obstruction. Stent failure occurred with 20/44 (45.4%) Percuflex™, 15/27 (55.6%) polyurethane, and 2/3 (66.7%) metal stents.
Univariate analysis of clinical factors associated with stent failure and UTI (including baseline patient characteristics, past medical history, initial stent size, and malignancy type) is summarized in Table 2. None of the tested clinical factors was associated with a higher risk of stent failure. When compared with prostate cancer, no malignancy types, including colorectal, gynecologic, or other malignancies, were associated with a higher risk of stent failure or UTI development. Significant predictors of UTI development were bilateral stenting (HR 2.26, p = 0.03) and history of radiation (HR 2.58, p = 0.019).
Univariate Cox Proportional Hazards Analysis for Clinical Predictors of Stent Failure and Urinary Tract Infection
UTI = urinary tract infection.
Kaplan–Meier estimated OS after initial stent placement is displayed in Figure 1. Median overall patient survival after initial stent placement was 19.9 months (95% CI 16.5–37.9 months).
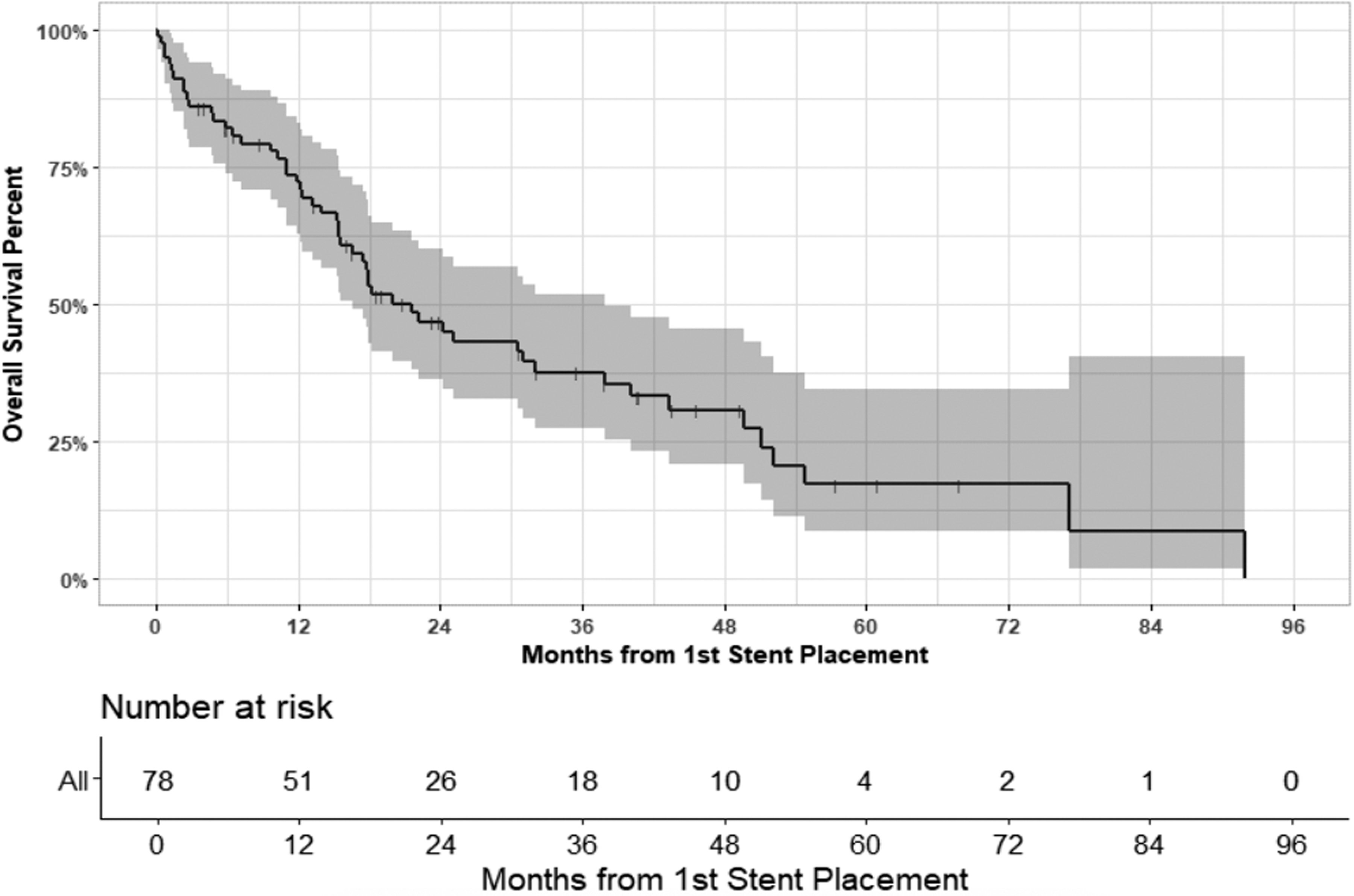
Kaplan–Meier estimated overall survival after initial stent placement.
Discussion
The management of MUO remains a clinically challenging scenario for urologists. Although ureteral stents are typically the preferred initial management option, the high rate of stent failure in this population represents a significant burden to both the patient and the health care system. Moreover, the diagnosis of MUO portends a poor prognosis for affected patients, further complicating medical decision-making. In our institutional experience, cystoscopically placed indwelling ureteral stents failed nearly half of the time, necessitating expedited stent exchange, PCN, or tandem stent placement. In addition, we found that history of radiation and bilateral stents was associated with an increased risk of UTI, whereas no baseline characteristics predicted the development of stent failure. We observed that stent failure rates are similar across patient demographics and clinical factors. Our results therefore reflect the challenges in determining which patients may require more frequent stent exchanges, upfront PCN, or tandem stents.
Those with failed stents experienced significant morbidity, most commonly because of symptomatic or worsening hydronephrosis, or urosepsis. Stratifying this population into those at greatest risk for stent failure is critical to improve outcomes in patients with MUO. These patients may require closer follow-up and different treatment strategies, but providers face uncertainty in identifying such patients. Moreover, with a median individual stent dwell time of 4.3 months, the morbidity to the patient is significant even for patients without failure. Most patients in our study underwent at least 2 stent exchanges, with a maximum of 17.
Previous studies have reported a variety of factors associated with stent failure for MUO with some inconsistencies. In a study of 71 patients with MUO attributable to nonurologic cancers managed with Double-J stents, Yu and colleagues reported that preoperative serum creatinine >1.2, Glasgow Prognostic Score >1, and mid to lower obstruction location were significantly associated with stent failure. 8 Conversely, our study found that a history of CKD (preoperative eGFR <60) was not associated with stent failure. More recently, Yoon and colleagues reported on 117 patients undergoing ureteral stenting for MUO and found that disease progression, prestent pyuria and procedural complications were associated with stent failure. 9 Other studies have suggested that age, bladder invasion, and severe hydronephrosis before stenting could be associated with failure. 10,11
However, few of these predictors have been reported consistently in the literature. 12,13 In a 2016 systematic review, Pavlovic and colleagues concluded that despite the existence of several potential risk factors, stent failure is most often related to cancer progression, 12 which is ultimately difficult to predict. Finally, ongoing studies on metallic stents have indicated a mean increase in functional duration of 4 months compared with traditional Double-J stents. 13 Although metallic stents offer the benefit of improved rigidity and increased dwell times, their major limitations include stent migration and occlusion. 12 Given the limited use of metallic stents at our institution and in this study, we are unable to validate differences in performance based upon stent material.
Perioperative and functional outcomes of ureteral stents and PCN for the management of MUO are similar. 14 However, although urologists and oncologists tend to prefer the use of ureteral stents over PCN, 15 patient quality of life with PCN has been shown to be equivalent or superior to indwelling ureteral stents over time. 16,17 Irritative voiding symptoms may occur in as much as 80% to 90% of patients with ureteral stents. 18,19 Moreover, as we have demonstrated in this study, most patients require multiple stent exchanges.
This process of exchanging stents every 3 or 4 months not only negatively affects patient quality of life but also comes with associated risks of general anesthesia. As we found in our study, a significant number of patients ultimately experience stent failure and require additional intervention. A retrospective study of 62 patients with MUO secondary to nonurologic malignancies found that roughly 37% of patients required immediate referral for PCN and 23% experienced stent failure at a later time. 20 Given the high rate of failure and adverse impact on quality of life, these data indicate the importance of careful consideration of upfront PCN, or tandem stents after initial stent failure, as part of a shared decision-making approach in patients with significantly limited life expectancy.
Finally, we found that patients with a history of radiation or bilateral stents were at greater risk for UTI. Given the high risk of urosepsis in this group, these results may indicate the importance of closely monitoring the urine culture data and clinical symptomatology in patients who have received radiation or those with bilateral stents. At present, the AUA only recommends periprocedural antibiotic prophylaxis in patients undergoing endourologic procedures. 21 This guideline is informed by randomized trial evidence that prophylaxis reduces the incidence of bacteriuria in patients undergoing ureteroscopic stone extraction. 22 Given our study findings, further investigation is warranted to determine whether a prolonged course of antibiotic prophylaxis may be beneficial in such patients who are at higher risk of UTI development.
A major limitation to our study is the selection bias common to retrospective analyses. As patients are not randomized based on stent diameter or composition, management decisions are presumably guided by physician preference, demographics, and clinical variables such as those included in our model. Therefore, stent failure rates may also be affected by differences in management decisions owing to these factors, such as the frequency of stent exchanges. With this retrospective study, we did not have information on stent-related quality-of-life information (such as the Ureteral Stent Symptom Questionnaire) 23 in this specific group of patients. Having such information may aid physicians in individualizing urinary tract decompression options offered to patients with MUO. Finally, given our limited sample size, larger multi-institutional studies are needed for this common and important clinical problem to better delineate factors that place patients with MUO at risk for stent failure.
Conclusions
Ureteral stent failure poses a significant medical burden to patients with MUO. Identifying patients at high risk for stent failure using baseline clinical factors poses a significant challenge to providers. Future studies may aim to identify these factors to optimize treatment strategies and minimize morbidity related to stent drainage in this generally poor prognostic population. Using a shared decision-making approach, clinicians and patients should consider PCN or tandem stents early in the management of MUO.
Footnotes
Authors' Contributions
N.A.P.: study design, data acquisition, data analysis, and article drafting.
B.M.W.: study design, data acquisition, and article drafting.
J.M.V.: study design, data analysis, and article drafting.
S.J.C.: study design, data acquisition, data analysis, and article drafting.
N.S.B.: study design, data acquisition, and article drafting.
G.M.H.: study design, data acquisition, and article drafting.
K.D.: study design, data acquisition, data analysis, and article drafting.
R.S.F.: study design, data analysis, and article revision.
A.C.D.: study design, data analysis, and article revision.
R.V.: study design, data analysis, and article drafting (Principal Investigator).
Acknowledgments
Preliminary findings of this study were presented as abstracts at the 36th and 37th World Congress of Endourology Meetings and are published in the Scientific Programs of the 36th and 37th World Congress of Endourology in the Journal of Endourology.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.