
Abstract
Introduction:
Incidence of urolithiasis in children has increased in recent years and with technological advancements and miniaturization of surgical instruments, pediatric urologists have acquired an impressive arsenal for their treatment. Retrograde intrarenal surgery (RIRS) has gained widespread popularity as it is a natural extension of semirigid ureteroscopy and can be done through natural orifice minimizing the morbidity of percutaneous access. The aim of this narrative review is to describe how RIRS has evolved over the decades in children and if the age-related anatomical difference impacts reported outcomes especially stone-free rate (SFR) and complications.
Materials and Methods:
An electronic literature search from inception to October 15, 2021 was performed using Medical Subject Heading terms in several combinations on PubMed, EMBASE, and Web of Science without language restrictions. A total of 2022 articles were founded and 165 articles were full-text screening. Finally, 2 pediatric urologists included 51 articles that summarize the available literature regarding the development and use of RIRS in children.
Results:
RIRS as of today is well established as a superior modality for all stones in all locations compared with extracorporeal shockwave lithotripsy both in children and adults. The passive dilation has decreased the need of active ureteral dilation, but the need to perform prestenting is not defined yet. Regarding the use of the ureteral access sheath, the literature tends to lean toward its placement in most cases, but we do not know its long-term effects over the growth of children. Finally, the SFR has increased as the experience of pediatric urologists increases, as well as the number of complications has decreased.
Conclusion:
RIRS in pediatrics has crossed many milestones, yet many areas need further research and larger data are required to make RIRS the procedure of choice for renal stone management in children across all age groups.
Introduction
Incidence of urolithiasis in children is reported to be lesser than in adults and affects 57 out of every 100,000 children. 1 However, environmental and dietary influences alongside metabolic and genetic mutations have increased this in recent years (2%–3% of cases) with an all-cause recurrence rate of 55% within 5 years. 2
Akin to treatment in adult patients, urolithiasis management in children has expanded options that include retrograde intrarenal surgery (RIRS), extracorporeal shockwave lithotripsy (SWL), percutaneous nephrolithotomy (PCNL), and endoscopic combined intrarenal surgery (ECIRS). In the European Association of Urology (EAU), RIRS is recommended as a second therapeutic option in pyelic stones less than 20 mm, focusing on its usefulness in lower calix (LC) stones with unfavorable anatomy for SWL or larger than 10 mm. Regarding SWL, it continues to be the first treatment option in pediatric patients with pelvic lithiasis smaller than 20 mm, LC smaller than 10 mm, and proximal ureteral lithiasis. PCNL is recommended as the first option in staghorn stones, pyelic stones larger than 20 mm, and LC stones larger than 10 mm. 3 The American Urological Association guidelines recommend RIRS in ureteral stones with a low probability of expulsion or in which medical management has failed, and they make a general recommendation to use it in those patients whose stone load is less than 20 mm regardless of location. 4
With technological advancement and miniaturization, urologists have acquired an impressive arsenal for endoscopic treatment of lithiasis in the last decade, making this procedure more popular. However, best practices and clinical steps of surgical intervention are a direct adoption of techniques used in adults as there are few in vitro data specific to the treatment of urolithiasis in children. Like miniaturized PCNL, RIRS has gained popularity and can be performed through the natural body orifice, minimizing the morbidity of percutaneous access. With the versatility and improvements in laser technology and techniques, all stone compositions can be effectively fragmented/dusted making RIRS the most promising new-age intervention for children. 5 However, the major difference from a surgical perspective between adults and children is the anatomy of the pyelocaliceal (PCS) system and genitourinary tract, with a wide variety of anatomic differences, even across the pediatric population, from infancy to adolescence. 6
The primary aim of this scoping review is to determine how RIRS in children has evolved over the decades and whether age-related anatomic differences affect reported outcomes, particularly stone-free rate (SFR) and complications. As a secondary aim, we hope that the evidence review can help identify future needs to improve RIRS outcomes in pediatric endourology.
Materials and Methods
Literature search
For the scoping review, an electronic literature search from inception to October 15, 2021, was performed using Medical Subject Heading terms in several combinations (Supplementary Table S1) on PubMed, EMBASE, and Web of Science without language restrictions. The search strategy included RIRS in the pediatric population and associated concepts. Bibliographies of included studies were also screened to ensure inclusion of all relevant studies between 1990 and 2021. Two independent authors screened all retrieved records through Rayyan Intelligent Systematic Review (
Selection criteria
The Patient Intervention Comparison Outcome Study Type model was used to frame and answer the clinical question. The population was children <17 years of age with renal stones that require surgery. The primary intervention evaluated was RIRS with laser lithotripsy in the pediatric population. Finally, the outcomes were safety, SFR, intra and immediate postoperative complications, and technical preferences.
A total of 2022 articles were founded. Two independent authors screened all retrieved records through Rayyan Intelligent Systematic Review (
Understanding risks and benefits of pediatric RIRS and ureteroscopy
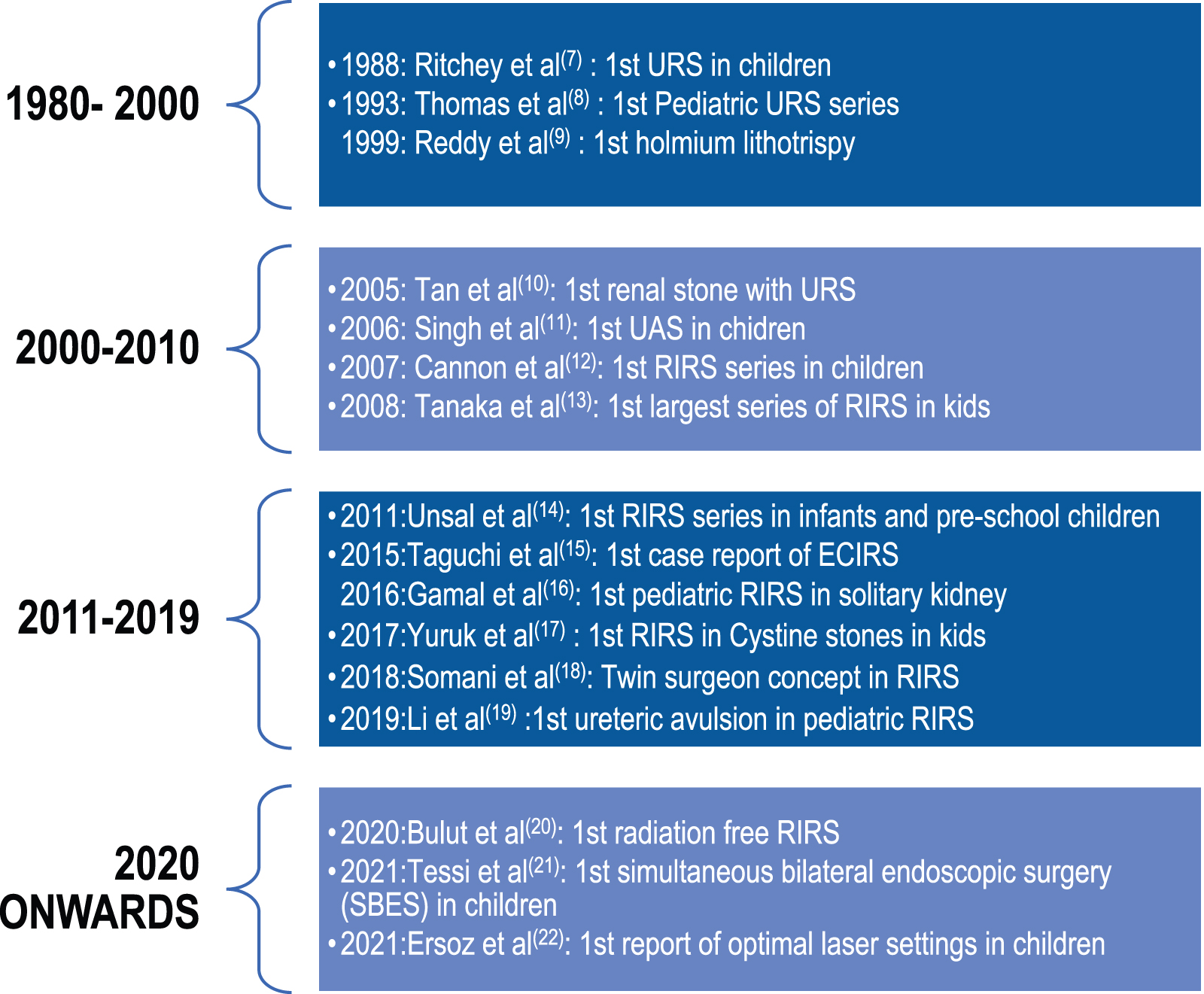
From the studies included in our review, we summarize the evolution of ureteroscopy (URS) in children over the decades, which has been brisk and remarkable (Fig. 1). It is evident from Figure 1 that the ability of RIRS to treat any stone at virtually any location in the kidney, as reflected in many of the studies listed in Table 1, has brought this technique to the forefront of pediatric urology over the decades.
Summary of Published Series of Kidney Stones in Children Treated with Retrograde Intrarenal Surgery
Seventy-five percent success in pelvis stones, 100% in polar stones, and 14% in staghorn.
SFR was 100% for stone ≤10 mm and 97% for >10 mm after a single ureteroscopy. cAt the discretion of the surgeon.
F = flexible; Frag + Extr = fragmentation and extraction only; fUTI = febrile urinary tract infection; KUB = kidney, ureter, and bladder radiograph; LC = lower calix; MC = middle calix; R = semirigid; RIRS = retrograde intrarenal surgery; SFR = stone-free rate; U = ureteroscope; UAS = ureteral access sheath; UC = upper calix; US, ultrasound; UTI = urinary tract infection; XR, x-Ray.
The main reasons for this are the miniaturization of endoscopes, the introduction of high-power holmium lasers (HPL), and a better understanding of the physics behind laser technology such as MOSES and the vapor tunnel effect, to name a few. 23 In the MOSES technology, laser machine splits the laser pulse into two peaks. The first one divides the water creating a bubble, while the second peak delivers the energy to the stone. 24 This two-peak laser pulse allows for amplified energy transport with more efficient laser lithotripsy. 25 The vapor tunnel technology is a laser modulation (long pulse with the minimum peak power according to selected output settings). The pulse generates a vapor tunnel, and the remaining energy passes straightforwardly through the previously produced tunnel. This creates an elliptical shape bubble producing flat and shallow cavities, dust, and less retropulsion. 26
The main concerns with RIRS are high intrarenal pressure and increased intrarenal temperature due to the laser. This intrarenal temperature increases the need for a ureteral access sheath (UAS), which in turn poses a potential risk for increased ureteral injury and prolonged need for postoperative stenting. 27 Because the tolerance for error in the pediatric population is minimal, the goal of any intervention is to achieve an SFR with minimal morbidity and to reduce the number of unnecessary additional procedures at all costs. For this reason, many studies have shown that PCNL is a superior surgical modality compared with SWL and still ranks first in all guidelines. 28 However, RIRS is more effective than SWL for small stones, including lower pole (LP) stones, with less morbidity than PCNL, and it is as effective as mini PCNL. 29
For the above reasons, it is essential for urologists to be familiar with the strengths and limitations of all endourologic procedures and to describe the long-term outcomes of the various surgical techniques in the pediatric population.
With increasing evidence in adults, urologists are also gaining confidence in the use of RIRS as the first choice for more complex stones, while simultaneously expanding its use to ECIRS and simultaneous bilateral endoscopic surgery. 30,31
To understand how pediatric RIRS outcomes have evolved over time in terms of stone volume, age groups, and location, and to understand the real-world techniques and steps used in practice for ureterorenoscopy and lithotripsy, we reviewed the literature and data from available case series, in which the stones in the upper urinary tract only, are summarized in Table 1.
RIRS Technique
Most publications agree that the semirigid URS is the first step. 13,35,36,38 This allows direct inspection of the ureter for the presence of stones and assessment of its diameter and elasticity, as well as active assistance in performing the ureteral orifice (UO) dilatation. 12 –14,16 Performing a retrograde pyelogram (RPG) gives a clear idea of the PCS anatomy concerning the location of renal stones, which is particularly useful for multiple stones and stones at the LP, followed by the placement of a guidewire. In children, a 4.5F ureteroscope is preferred, but a 6F to 7.5F scope can also be used with caution. The practice of active dilatation of the UO has declined over the past decade, in light of reports of vesicoureteral reflux and ureterovesical injury. 39 Passive dilation with a Double-J stent left in situ for up to 2 weeks is currently the preferred method as also seen in 6 of our studies (Fig. 1). The question remains whether this should be routinely performed in all patients before RIRS or only when access with the ureteroscope has failed on the first attempt?
In adults, stent placement before RIRS can be performed under local or moderate anesthesia as a quick outpatient procedure, but for a child, this means an additional general anesthesia (GA), which defeats the minimally invasive nature of the intervention. In our series, as there were no complications with prestenting, this strengthens the case for prestenting in children to avoid unnecessary ureteric injury. However, as this may need an additional anesthesia in children, whether this is feasible is to be considered. In adults, measures, such as taking preoperative alpha-blockers for 2 weeks in conjunction with UAS and smaller diameter scopes, have been shown to be effective in improving the success of primary UAS without compromising the safety of UAS placement, 40 avoiding ureteral injury as described by De Coninck et al, 27 and avoiding the possibility of ureteral avulsion as reported by Li et al. 19 Further pediatric studies need to confirm this, as all precautions must be taken to completely avoid this terrible complication.
Currently, there are no guidelines or consensus statements, and this needs to be studied in more detail in children, as the diameter and elasticity of the ureters are different in different age groups. 41 The use of alpha-blockers for medical expulsive therapy in children is well established 42 and alpha-blockers might be helpful to eliminate ureteral fragments since Tasian et al demonstrated that their use was associated with more than three folder of spontaneous passage of ureteral stones. 43 However, the use of alpha-blockers before RIRS as a complementary measure in adults is unknown.
Ureteroscopes: which one should we use?
For RIRS proper, the choice of using a disposable vs reusable and digital vs fiberoptic depends on the surgeon's individual preference and available resources.
Chandramohan et al 36 have used 7.5F fiberoptic scopes and Jones et al 44 have used disposable digital scopes with equal success in pediatric cases. Since, intrarenal anatomy differs in age groups, a careful dynamic assessment of the ureteropelvicaliceal system with an on-table RPG and diagnostic URS may best help to determine what scope may be best used for each individual case.
In a recent prospective randomized controlled trial (RCT) in adults by Bozzini et al 45 disposable ureteroscopes were characterized by significantly lower postoperative complications and infection rates, while having comparable costs and SFRs. This is an important finding and may be useful to assess in children as well.
UAS in children
Nine of the 11 series in Table 1 reported the use of a UAS 36 after semirigid URS. Some pediatric surgeons performed UO dilation before the passage of the ureteral sheath, but this practice has been in decline. 39 The preferred UAS that is considered safe for children is the 9/11F UAS. 36,38 Singh et al 11 were the first to report their results in 2005 using UAS in 8 children with a mean age of 9 years. They reported no complications and concluded that UAS appears to facilitate flexible URS and lithotripsy for multiple renal and proximal ureteral stones.
Aljumaiah et al 46 demonstrated in a single-center study that a 10/12 F UAS was successfully placed in all 14 children (9 months to 17 years of age) with no reported complications. Anbarasan et al 38 placed a UAS in all of their cases (2–16 years) with no procedural or long-term complications reported at a mean follow-up of 26 months (4–37 months). This again demonstrates that UAS can be safely used in all age groups. The 7.5F flexible ureteroscope is almost always preferred in pediatrics. Newer disposable ureteroscopes are also available in smaller diameters and can be a very useful alternative in centers where RIRS is not routinely performed but expertise is available. This was confirmed by Ferretti et al, 47 who reported that 100% single-stage access, with a 76.6% SFR was achieved in children 2 to 16 years of age during RIRS of stones <2 cm.
In 2018, De Coninck et al 27 concluded that the use of a UAS improves irrigation and decreases intrarenal pressure but found insufficient evidence that its use decreases complications or increases SFR. EAU guidelines 3 do not recommend mandatory routine use of a UAS and leaves it to the surgeon to consider its use when placement is readily available.
Based on the available data, it is not possible to make an absolute recommendation for or against its use in the pediatric population. However, if the pediatric urologist feels that the best option for the patient is a UAS, the smallest available should be used. Furthermore, the follow-up period in the pediatric population is limited to 2 years, so any long-term adverse effects still need to be explored.
Lasers in pediatric RIRS
Holmium lasers have been time tried in adults and children over time, with laser lithotripsy first reported by Reddy et al 9 in 1999 (Table 1). Ho:YAG is the most commonly used laser, as seen in all 11 series (Table 1). Similar to Chandramohan et al, 36 Ersoz et al 22 reported in a follow-up of 116 children undergoing PCNL and RIRS with holmium laser that low-power settings of 0.5 to 0.8 J and 10 to 20 Hz were effective for RIRS with minimal complications, including febrile urinary tract infections. Of note, no study compared dusting vs fragmentation with extraction. Seven studies used fragmentation to retrieve stones for analysis, whereas three studies used a dusting approach, and one study a combination of dusting and fragmentation according to each case. The remaining one did not report the lithotripsy mode. The SFR in the studies included in our analysis ranged from 50% to 100%, with 5 of 11 studies reporting an SFR of 80% or greater (Table 1). In the more recent series after 2016, 16,17,37,38 an SFR of nearly 95% or greater was reported, demonstrating how the training or acquisition of knowledge and a better understanding of laser physics and its applications has made RIRS a highly effective modality for pediatric lithiasis.
As mentioned by Traxer and Keller, 48 the new Thulium fiber laser (TFL) technology seems to be particularly beneficial for RIRS and may become the next reference laser for kidney stone treatment. Because the TFL outperforms the Ho:YAG laser in terms of dust quantity and quality, produces much finer particles, significantly reduces retropulsion, and lowers stone ablation thresholds by a factor of four, it has been hailed as the laser of the future. 49 However, its safety in children has not yet been proven.
The use of MOSES and HPL technology and limited use of TFL in children have been mentioned by Lim et al. 50 They report that while ideal laser settings in children are unknown, the use of TFL in 39 patients was associated with better SFR compared with conventional holmium laser.
To stent or not to stent following RIRS
First described in 1978 by Finney, 51 the ureteral stent has secured a permanent place on the shelves of all urologic theaters worldwide. The use of a Double-J stent after RIRS is another important consideration, especially since it requires an additional outpatient procedure under GA in children and can be troublesome. 44 Many urologists individualize each case depending on the operative time, size of the stone, or suspected injury to the ureter during the procedure. In clinical practice, there are now several noncystoscopic removal methods such as stent on string, magnetic retrieval, and modified snare techniques. Mainly studied in adults, an increasing number of studies have been reported in the pediatrics but formal evaluation of the available evidence remains inadequate until recently when the EAU Young Academic Urology Urolithiasis Group found the use of the above techniques to be safe and effective, feasible alternatives that can save GA and its associated costs. 52
Special Considerations in Pediatric RIRS
RIRS in different age groups
Regarding the age for the implementation of the RIRS, there is no limit, since the reports range from children under 1 year to adolescents. The first case series on pediatric RIRS was published by Cannon et al 12 in 2007, but most children were postpubertal (>15 years old). In 2011, Unsal and Resorlu 14 published the first series of publications on the efficacy and safety of RIRS in 16 preschool children <7 years (mean age: 4.2 years) with kidney stones (mean size: 11.5 mm). Balloon dilation of the UO was required in 29.4% and UAS was placed in 17.6%. One 14-month-old girl with balloon dilation experienced distal ureteral perforation and extravasation. SFR was 88% (100% for stones <10 mm and 81.8%> 10 mm). A Double-J stent was placed in all patients.
In 2014, Erkurt et al 35 presented their cohort of 65 children under 7 years of age with kidney stones (38.8% in LC). The mean stone size was 14.6 mm. They attempted to use UAS in all patients, but only 61.5% were successful. In the remaining 30.8%, they reported for the first time direct flexible URS by railroading over the guidewire. SFRs were 83.07% and 92.3% after the first and second procedures, respectively. There were no significant differences between the prestented and nonstented patients in terms of SFRs, complication rates, operative times, and reintervention rates.
Kim et al 33 reported the experience with the flexible URS at Philadelphia Children's Hospital and reported the results of 170 procedures performed on 167 pediatric patients with a mean age of 5.2 years (range: 3–218 months). The mean stone dimension was 6.1 mm (range: 3–24 months), with only 60% of cases being intrarenal (28% pelviureteric and 12% upper ureteral stones). Interestingly, no intra- or postoperative complications were reported in this series. Recently, in 2020, Chandramohan et al 36 published their work on 62 children <5 years old, with kidney and upper ureteral stones of 12 mm. All children had Double-J stent preoperatively for 12 days. They are the first to describe the need for urethral dilation with Hegar dilators. UAS placement was successful in 63.5% but was unsuccessful in younger children (<12 months) with an SFR of 76.3%. In two patients, the ureter was injured during UAS insertion and in the postoperative period complications occurred in 38%, most of which were Clavien–Dindo I. It is from here that the highest rate of failure in the placement of UAS in infants begins to be reported, compared with children in the preschool stage. Before them, a comparison between the different age groups had not been made.
Regarding the age impact on the success of the surgery, only the systematic review of Ishii et al 53 in 2015 found greater complications in patients under 6 years of age, but there is no clear explanation for this methodological finding. A plausible reason for this is that intrarenal anatomy varies in children at different stages of development. Therefore, the surgeon must adapt the principles of RIRS based on a dynamic continuous evaluation of the intrarenal anatomy to avoid the negative effects of intrarenal pressure 54 and high temperatures 55 that can cause complications, especially when using high-power lasers. For the rest, the publications do not find a direct relationship between the SFR of the RIRS and the age of the patients.
With so many different practices, a standardized approach for different age groups is needed to avoid complications and maximize outcomes.
RIRS and stones >2 cm
The only RCT, which randomized 43 renal units with renal stones >2 cm in RIRS and PCNL (21 and 22 patients, respectively) by Saad et al 56 showed that the SFR of RIRS monotherapy was significantly lower compared with PCNL monotherapy (71% vs 95.5%, p = 0.046), but the PCNL group had statistically significant more complications compared with the RIRS group (p = 0.018).
The EAU guidelines for children 3 recommend PCNL in children with stones larger than 2 cm, and to date, there are no specific recommendations for RIRS. However, because it has minimal complications, it has the potential to treat stones up to 2 cm in diameter, as well with ECIRS, or an alternative staged option when percutaneous, open, or laparoscopic surgery is not feasible.
Lower caliceal stones
Pearle et al 57 and Kuo et al 58 tried to identify the best approach and outcomes for the treatment of LP stones in adults. However, this remains an enigma for both adults and children, and infundibular length, width, and infundibulopelvic angle, 59 all play a role in outcomes after any form of lithotripsy. On RIRS for LP, the principal concerns are the ability to access and effectively clear all stones in this part of the kidney. In the systematic review by Karim et al, 60 it was found that an infundibulopelvic angle of less than 30° significantly affected the SFR of the RIRS in the LP of adults. Donaldson et al 61 in a meta-analysis compared PCNL, RIRS, and SWL in adults. They concluded that SWL was less efficient in LP stones.
In children, we could not find a focused review analyzing the impact of renal anatomy on RIRS outcomes. In 2007, Cannon et al 12 described 21 RIRS in LP for children with a mean age of 15 years. The mean stone burden was 12 mm. Three-quarters of all children had a 93% SFR at 11 months. Halinski et al 62 analyzed 38 RIRS and 15 MicroPerc for stones in LC in children. RIRS and MicroPerc were comparably effective methods of treating LC stones in children, but RIRS patients have a lower risk of complications (6% vs 2.6%) and hospital stay.
The lack of dedicated LP studies necessitates further studies. However, because the safety of RIRS is well established, and the results are comparable to those of MicroPerc and mini PCNL, RIRS can be used for LP stones. Ong et al 63 have described how micro-ECIRS may be the best approach for small-volume stones in the pediatric age group, and herein lies the value of adding flexible URS to renal access.
Follow-up images post-RIRS
The EAU does not establish a follow-up imaging protocol, but it does emphasize the primary use of ultrasound and abdominal radiography for diagnosis and recommends it for follow-up. Indeed, Resorlu et al 64 showed that a combination of ultrasound and plain abdominal radiography was a safe and effective imaging procedure in postoperative follow-up of children undergoing URS, with a sensitivity, specificity, negative and positive predictive values for detecting hydronephrosis, and residual fragments (RF) of 85.7%, 100%, 97.7%, and 100%, respectively. Low-dose noncontrast tomography (LD CT) would be the ideal study but given the ionizing radiation to which children would be exposed, it is only recommended in cases where the first two images mentioned do not give a clear diagnosis, much less is indicated in follow-up postoperative. 3 Lim et al 50 reported in their multicentric study that only 1% of the cases have CT scan in the follow-up of RIRS and more than 67% had ultrasound alone or in combination with kidney, ureter, and bladder radiograph.
LD CT has been shown to have 59% lower organ-specific radiation compared with standard CT, and currently the ultra-low-dose CT (ULD CT) protocols have been developed. A systematic review demonstrated that ULD CT (<1.9 mSv) and LD CT (<3.5 mSv) had comparable sensitivity for ureteral stones. 65 Perhaps in the future, this type of improvement in terms of radiation reduction may be sufficient to consider this imaging modality as the standard also in pediatrics and help us create more explicit criteria for SFR.
RIRS and Special Scenarios
Solitary kidney
Lithiasis management in a solitary kidney requires a minimally invasive approach with maximum SFR and minimal morbidity, in both adults and children. Furthermore, the risk of bleeding and the need for blood transfusion may be higher in patients with a solitary kidney due to a compensatory increase in renal parenchymal thickness. 66 In 2016, Gamal et al 16 included 14 children with solitary kidneys with a median age of 9.5 years, who had RIRS (mean stone size12 mm) and no UAS used. All stones were dusted and the SFR was 79% on the 1st postoperative day, reaching 100% after 3 weeks. This is the only report on children, and they confirmed that RIRS is safe and efficient, and no intraoperative complications were observed. This could be indicative of how an experienced surgeon can achieve good outcomes by RIRS even in challenging cases, yet, as in the above series, nonusage of UAS can be a double-edged sword for complications and again reiterates the need for more insight through clinical trials.
Cystine stones
Cystinuria patients have a life-long risk of cystine stone formation, which are shockwave resistant, and often have impaired renal function and low quality of life. This accounts for 2% to 6% of all urinary stones in children. The high recurrence rate makes this metabolic disorder a therapeutic challenge for pediatric urologists. 3,67,68 For adults, flexible URS is the ideal intervention with a low complication rate, except for staghorn stones. 69
Yuruk et al 17 reported on RIRS in children with cystine stones, 14 children 11 years of age with an average stone diameter of 13 mm, had a 100% SFR with a short surgical time of 38 minutes using holmium lithotripsy. A Double-J stent was placed in all patients and subsequent medical management was initiated. Pediatric urologists can have confidence in this study, which paves the way for a safe alternative to PCNL in managing the complex problem in a minimally invasive way.
RIRS in anomalous kidneys
We did not find any current evidence or articles supporting the use of RIRS in children with anomalous kidneys. A recent multicentric publication by Garcia Rojo et al 70 on trends and outcomes of RIRS for the treatment of urolithiasis in anomalous kidneys reported that it is safe and effective with a high single-stage SFR and low complication rate. Considering that anomalous malformations are picked up earlier in pediatric patients with lithiasis, extrapolating this evidence we could establish that RIRS is an equally safe and effective tool. It is time for clinical trials and evidence acquisition to establish its potential as an adjunct to PCNL 71 and SWL in this population.
Future Directions and Requirements for Pediatric Urolithiasis
RIRS in pediatrics has crossed many milestones, yet many areas need further research and larger data are required to make RIRS the procedure of choice for renal stone management in children across all age groups. We have identified the key areas for future research, and this can help any urologist doing RIRS in children. Perhaps it is indeed time for a pediatric endourology subspeciality as RIRS promises to be the next best evolution even in pediatric urology by its versatility and safety profile.
Footnotes
Authors' Contributions
Y.Q.M. and V.G.: Abstract screening, reading full articles, and article writing/editing. B.K.S., E.G., M.C., and J.Y.C.T.: Systematic search of articles, and article writing/editing. Y.T., O.T., and A.B.T.: Protocol/project development, and article writing/editing. S.T., S.S., E.J.L., and K.Y.F.: Systematic search of articles and article categorization. D.C.: Abstract screening and article writing/editing. B.M.Z.H., E.L., and H.S.D: Systematic search of articles.
Author Disclosure Statement
None of the authors has conflicts of interest.
Funding Information
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest or nonfinancial interest in the subject matter or materials discussed in this article.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.