
Abstract
Aim:
To conduct a comparative, nonrandomized study to assess the feasibility of mini-Endoscopic Combined Intrarenal Surgery (ECIRS) using supine Mini-percutaneous nephrolithotomy (PCNL) access (16F) in Galdakao-Modified Supine Valdivia position for managing proximal large-volume impacted ureteral calculi as ambulatory day-care surgery vis-a-vis standalone ureteroscopy (URS) with push-back PCNL, if needed. The primary aim was to study the outcomes and stone-free rates (SFRs). Secondary aim was to compare the intraoperative and short-term postoperative complications.
Materials and Methods:
Data of 60 patients undergoing ECIRS (Group 1) from January 2016 to December 2019 were collected prospectively in a nonrandomized fashion from a single center after Ethics Committee approval. A matched-paired analysis was performed with retrospectively collated data of 60 patients undergoing standard URS/pushback PCNL (Group 2) using analysis of variance, Fisher's exact test, and Chi-square test. p < 0.05 was considered statistically significant.
Outcomes and Results:
Group 1 patients had a significantly shorter procedure time vs Group 2 (42.1 ± 11.2 minutes vs 52.1 ± 13.7 minutes; p < 0.001). Group 1 (59/60) patients had an overall single stage SFR of 98.3%, which was significantly higher than single-stage SFR of 83% in Group 2 (50/60) (p < 0.002). Group 2 patients had a higher incidence of fever (10 vs 4, p = 0.01). However, there were no cases of sepsis in either group. Rest of the complications were comparable for both, as the need for ancillary procedures was significantly higher in Group 2 (10% vs 1.7%, p < 0.001). Patients were discharged on the same day in both groups.
Conclusions:
The findings of our study suggest that, in large and impacted proximal ureteric stones, combined minimally invasive endoscopic approach offers the best option to render the patient stone free by a single intervention. With better intra- and postoperative outcomes and safety profile, Mini-ECIRS may be considered as an ambulatory procedure in this setting.
Introduction
There are many therapeutic approaches for treatment of proximal ureteric stones, including shockwave lithotripsy (SWL), ureteroscopy (URS), percutaneous nephrolithotripsy, laparoscopic ureterolithotomy, and open ureterolithotomy, depending on size, degree of impaction, and ability to access the stone. 1
The dilemma about the best approach through antegrade or retrograde access for large proximal ureteric stones persists as both have advantages and disadvantages. Furthermore, the clinical presentation, stone characteristics, amount of impaction, and secondary changes in the pelvicaliceal system (PCS) may influence the decision and outcomes. 2 While antegrade approach allows for easy access to renal stones, flexible instrumentation may be needed to approach the pelviureteric junction and beyond. Conversely, retrograde approach may be difficult if ureter is inaccessible, and fragments may retropulse during lithotripsy. 3,4 Percutaneous nephrolithotomy (PCNL) with flexible nephoscopy and PCNL alone with a staged second-look URS have both been time-tested procedures with variable success and often patients require ancillary procedures to achieve complete stone clearance. 5,6 However, Cracco et al and Ergin et al suggested a combined approach with options of flexible instruments as the better way in managing complex renal and ureteric stones. 7,8
This study was conducted aiming for a comparative, nonrandomized study to assess the feasibility of doing upfront ambulatory mini-Endoscopic Combined Intrarenal Surgery (ECIRS) using a supine Mini PCNL access (16F) in the Galdakao-Modified Supine Valdivia (GMSV) position for managing the proximal large volume and impacted ureteral calculi. The secondary aim was to compare the stone-free rate (SFR), intraoperative and immediate postoperative outcomes of this procedure with just a standalone URS or Retrograde Intrarenal Surgery (RIRS) combined with push-back PCNL access if needed. We also looked how our outcomes fare with those in available literature.
Materials and Methods
Study design
Inclusion and exclusion criteria
Adult patients with a single large impacted proximal ureteral stone (>10 mm) situated below pelvi ureteric junction (PUJ) up to a distance of <5 cm from PUJ were included in the study. Included patients had a normal renal function (Cr <1.2 mg/dL) and no history of prior treatment for the same stone. Patients with concomitant renal, mid, or distal ureteral or bladder stone were excluded from the study. Pediatric (<15 years) and pregnant patients were also excluded. Patients unfit for general anesthesia (GA) or with spinal deformity, ongoing treatment for documented active urinary tract infection, those with previous sepsis and indwelling nephrostomy or Double-J stent, as well as those with previously known or newly diagnosed bleeding disorders were also excluded. Furthermore, on table, if there were any ureteric anomalies or stones found impacted and embedded in the ureteric mucosa that may cause a stenosis/stricture and hence planned for a second-stage procedure subsequently were also excluded from this study. An informed consent was obtained from all the patients regarding the procedure and possible need for subsequent intervention for residual fragments (RFs).
All necessary permissions were obtained from the Institutional Ethics Board and the study was approved by the Institutional Review Board (2015-52).
Preoperative assessment
All patients had a routine baseline laboratory evaluation for their renal function and urine culture. A diagnosis of a proximal ureteric stone was confirmed by a noncontrast CT scan, CT urogram or intravenous urography. Patients underwent a preanesthetic check-up for fitness for GA and were admitted on the day of surgery. Preoperative antibiotics were given at induction.
Operative technique (Group 1)/modern approach (upfront supine ECIRS only)
All patients had GA and were directly positioned in the supine GMSV position for ECIRS. 9 Two surgeons positioned themselves appropriately for a mini PCNL (16fr) and URS, respectively. Initially a semirigid URS with a 6/7.5Fr URS (Richard Wolf, Knittlingen, Germany) was done to inspect the ureter and an attempt was made to pass a hydrophilic guidewire across the stone into the PCS, and to disimpact the stone to push it into the kidney if possible. If the stone was impacted, fragmentation was incomplete with significant remaining stone burden and in those cases where even with a flexible URS, the stone clearance was incomplete or significant stone fragments migrated proximally, which could not be accessed retrogradely, a decision to proceed with Mini PCNL was made to achieve 100% clearance in the same sitting.
Percutaneous access was then made under ultrasound (USG) and/or fluoroscopic, along with endoscopic guidance, in a supine position. Initial puncture was done with a trocar tip 18-gauge needle (Cook Medical), and a Terumo guidewire was used for establishing the tract. The tract was dilated with Teflon screw dilators (15F) followed by 16F mini PCNL sheath from Karl Storz, Germany, which is preloaded with a 15F Single-step reusable screw dilator sourced locally, as shown in Figure 1. A 12F nephroscope (Karl Storz) was used to inspect the PCS and approach the stone. Laser lithotripsy/stone extraction was done antegrade by the vacuum cleaner effect or with a basket, aided from below by ureteroscope, which also prevented distal migration of fragments. Complete stone clearance was confirmed on fluoroscopy and combined use of nephroscope and ureteroscope. 10 A Double-J stent was placed at the end of procedure, and all cases were completed in a tubeless fashion. 11 The Double-J stent was removed under local anesthesia on follow-up after 2 to 3 weeks.
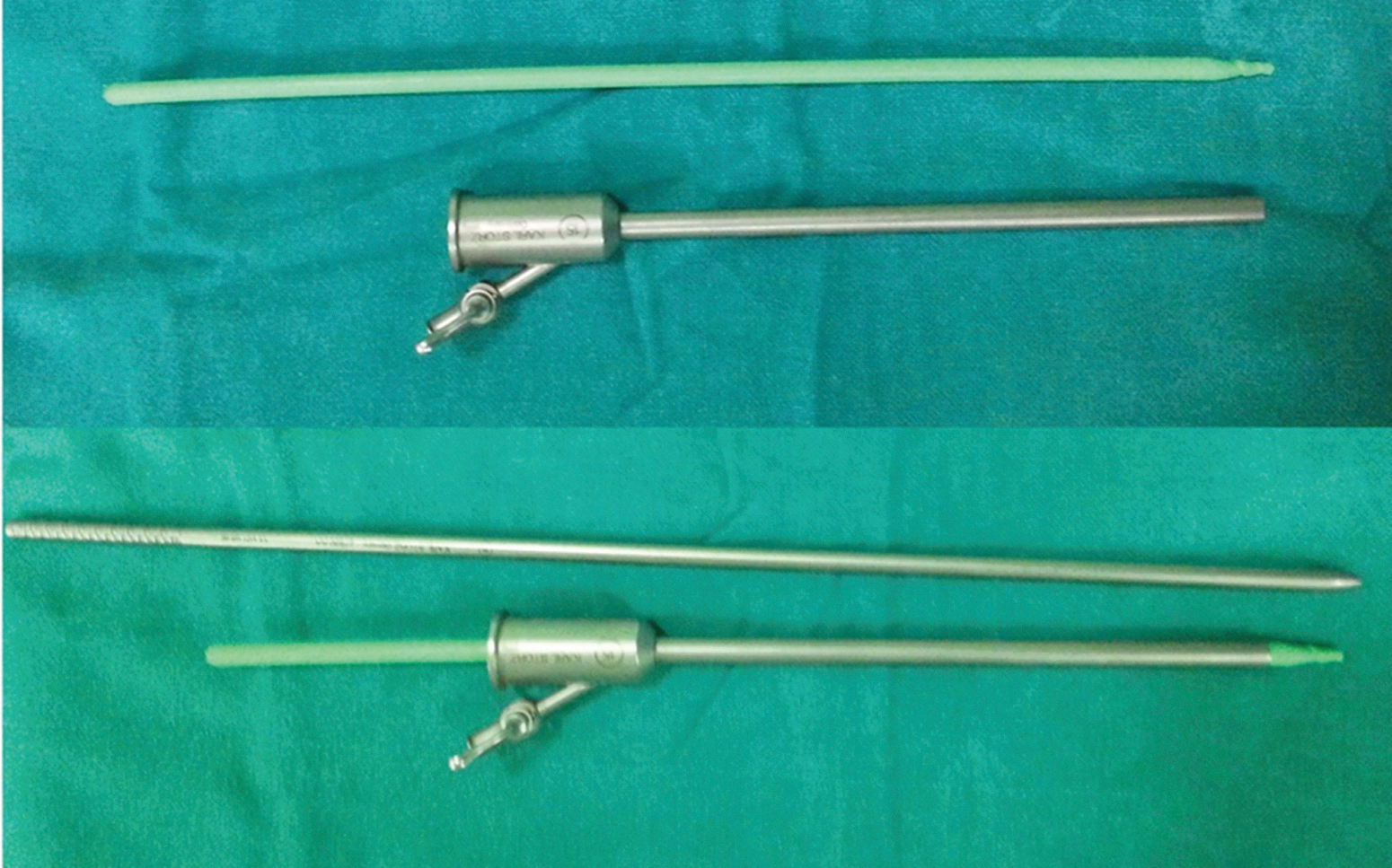
Single-step screw dilator with preloaded access sheath. Color graphics are available online.
Operative technique (Group 2)/traditional approach (upfront semirigid or flexible URS failing which prone antegrade mini percutaneous access)
A single surgeon operated on all the cases in this group. Patients were placed in a lithotomy position, and cystoscopy and retrograde pyelography followed by a semirigid URS with 6F/7.5F scope (Richard Wolf, Knittlingen, Germany) Flexible URS was also attempted in some cases where the stone was reached with semirigid ureteroscope, but the partial fragmented calculus migrated into the kidney proximally.
After an initial check, cystoscopy attempt was made to access the proximal ureteric stone for fragmentation and lithotripsy by semirigid URS. If retrograde access was unsuccessful either due to a difficult ureter or stone migration, the patients were then made prone and an antegrade access was attempted by percutaneous approach.
A mini PCNL was done to clear the stone, following which a Double-J stent was placed as part of tubeless procedure, which was subsequently removed in 2 to 3 weeks under local anesthesia.
A matched pair analysis of prospectively collected data between January 2016 and December 2019 was made between Group 1 patients (n = 60) (Upfront supine ECIRS) vis-a-vis Group 2 (Semirigid URS±Prone mini PCNL) (n = 60). The primary aim of the study was to compare the feasibility and safety of intervention in Group1 with Group 2. The secondary aim was to assess the efficacy and intra and immediate perioperative outcome of the modern approach in managing impacted proximal ureteric calculi.
Follow-up and outcome assessment
Patients were discharged within 24 hours if they had no fever, pain, or significant bleeding. An X-Ray kidney, ureter, and bladder radiograph (KUB) was done on the day of discharge to assess stone clearance. On follow-up visit at 2 to 3 weeks, another X-ray KUB and USG examination was done before Double-J stent removal to assess the final stone clearance in both groups. Complications were assessed according to the Clavien classification. 12 Outcomes assessed were SFR, operative time, hospital stay, and complications. The operative time for both groups was from start of URS until completion of the procedure, excluding the time for anesthesia.
Statistical analysis
The results are presented as mean ± standard deviation. All the parameters were analyzed statistically using the analysis of variance, Fisher's exact test, and Chi-square test. A p < 0.05 was considered statistically significant.
Results
The analysis was done in R Studio (version 1.3.1073). All the parameters were analyzed statistically using the analysis of variance and chi-square test. A p-Value <0.05 was considered statistically significant.
Demographic parameters of both groups were well matched for age, body mass index, gender, and stone size (Table 1). The mean distance from uretero pelvic junction to stone was 2.6 ± 1.26 cm in the mini-ECIRS group and 3.05 ± 1.20 cm in the ureteroscopic lithotripsy (URSL) group, which was statistically significant (p = 0.047). However, this did not have a clinical significance in influencing the choice of directly using either a semirigid or flexible ureteroscope as preferred instrument for retrograde access in either group.
Basic Demographic and Operative Parameters
ECIRS = endoscopic combined intrarenal surgery; PCNL = percutaneous nephrolithotomy; RIRS = retrograde intrarenal surgery; URSL = ureteroscopic lithotripsy.
Group 1 patients had a significantly shorter procedure time of stone removal vs Group 2 (42.1 ± 11.2 minutes vs 52.1 ± 13.7 minutes; p < 0.001). Group 1 (59/60) patients had an overall single stage (SFR) of 98.3%, which was significantly higher than single-stage SFR of 83% in Group 2 (50/60) (p < 0.002).
On subgroup analysis of Group 2, there were three subsets. Initially all 60 patients underwent semirigid URS (Table 2). The first subgroup of 15/60 (25%) cases had only semirigid URS and did not proceed to RIRS or PCNL. In this subgroup, 10 had complete clearance, whereas 5 were found to have RF on follow-up. Only 3/5 needed to undergo repeat URS as ancillary procedure for fragment removal giving this subgroup a clearance rate of 10/15 (66.6%).
Group 2 Subset Analysis
URS, ureteroscopy.
The second subgroup included 19/60 (31.6%) cases who proceeded to RIRS following semirigid URS. Only 15/19 (78.9%) had complete clearance following RIRS and 4/19 had RFs with only 1/19 needing an ancillary procedure in this subgroup.
The third subgroup had 26/60 cases who went for Mini PCNL in prone position following failed URS. This subgroup had complete clearance in 25/26 (96.15%) cases and only 1/26 needing an ancillary URS to clear a fragment. The overall clearance in Group 2 was 50/60 (83%).
At the end of the procedure, all the patients had a DJ stenting (mini-ECIRS n = 60 and URSL group n = 59). Patients in both groups were planned for discharge from the hospital on postoperative day one. Although the values were not significant (p = 0.21), postoperative stay was 3 hours higher in Group 2 (30.2 ± 11.2 hours) compared with Group 1 patients (27.7 ± 9.99 hours).
Group 2 patients had a higher incidence of fever 10 vs 4 (p = 0.01). However, there were no cases of sepsis in either group. Rest of the complications were comparable for both (Table 3). The need for ancillary procedures was significantly higher in Group 2 (10% vs 1.7%) (p < 0.001).
Postoperative Outcomes
Discussion
EAU guidelines on urolithiasis recommend URS (ante- or retrograde) as first option for large (>10 mm) upper ureteric stones. 13 Several options, including open approach, laparoscopic ureterolithotomy, extracorporeal SWL, have been described with variable success in the past to approach these stones. 14 –17 However, when impacted, achieving a good stone clearance in large proximal ureteric stones with minimal morbidity has been debatable.
A simultaneous dual approach may be ideal in this unique situation. By accessing the stone from an antegrade and a retrograde approach, one can ensure that all fragments can be cleared in a single session even if they retropulse into the kidney. Furthermore, it may be safer to extract stones percutaneously from the kidney rather than retrograde from the site of an inflamed ureter secondary to stone impaction. 18,19 Described by Scoffone et al for improving outcomes in endoscopic renal stone intervention, ECIRS can be a potential one-stop solution for this unique dilemma in the management of proximal ureteral calculi especially large and impacted calculi. 9,20
Miniaturized intervention can not only give a good SFR, it can also minimize the complications of a standard access both in PCNL and RIRS in adults and children too. 12,21 –23 Ong et al 24 and Biligere et al 25 have described how even micro-ECIRS has the potential to treat large-volume renal and ureteral stones with good outcomes. In our study Group 1, patients had a significantly higher SFR (p < 0.002) and lower need for ancillary procedures as compared with Group 2 patients (p < 0.001).
SFRs with URS alone for large upper ureteric calculus of size >10 mm range between 71% and 87% with stone retropulsion rates ranging from 5.4% to 27.7% among various studies. 26 –28 Mini PCNL as a standalone modality for large impacted calculi has SFRs of >90% in multiple prospective studies with lower complication rate compared with standard PCNL. 19,29 In our study, patients in Group 2 had poorer single-stage SFR, and only after changing the position of patient to prone for a mini PCNL, the SFR reached 96.15% (Table 2) comparable to other reported series of ECIRS. 30
This clearly demonstrates the benefits of combined minimally invasive approach to obtain higher single-stage SFR, as well as ease in intervention in supine position. 31 In our study, in Group 1, ECIRS in supine position was successfully performed in all 60 patients with minimal complications, and high single-stage SFR. Only 1 patient required an ancillary procedure (Table 3) confirming its efficacy in impacted proximal large ureteric calculi. The caveat being preoperative counseling to the patient that there may be need for either antegrade or retrograde or simultaneous access based on a dynamic intraoperative anatomical assessment on table, which is the fundamental key to tailor and personalize stone approach by ECIRS. 32
ECIRS does indeed need the presence of two surgeons and two sets of operative endoscopic equipment and the trade-off for a higher SFR maybe additional cost. However, by maximizing SFR, we can minimize ancillary procedures and this can offshoot any additional hospital and surgical intervention cost for patients. Patients who were managed through the modern approach had an overall lower complication rate, allowing majority of patients to be discharged within 24 hours with just a Double-J stent. These outcomes do favor the option of performing ambulatory tubeless ECIRS procedure. 33
Limitations and strengths
The major limitation of the present study is that this is a single-center nonrandomized study, a matched-pair analysis comparing two cohorts of patients with proximal ureteric stone managed in two different time periods. However, the cohorts are well matched in demographics and outcomes were measured in a robust way.
A definitive advantage is seen with miniaturized supine ECIRS in obtaining a high single-stage SFR, with low complications even when done as ambulatory daycare surgery procedure. ECIRS allows the surgeon complete flexibility of managing the stone synchronously through dual access, and the urologist must use the advantage of visualizing the complete caliceal system unequivocally to remove any RFs that might be missed by fluoroscopy alone. To our knowledge, this is the first study that has attempted to objectively compare real-world practice outcomes of miniaturized supine ECIRS done as a daycare ambulatory procedure vs URS and push-back PCNL.
We also acknowledge that a randomized study would indeed highlight the missing details in our study, especially radiation time, a true reduction in the postoperative imaging by single intervention, the real cost burden and influence on fluoroscopy and radiation exposure, as well as long-term outcomes of impaction on kidney function. A CT scan would have been the best way to assess residual stone. However, we have primarily relied on a visual on table assessment and an X-ray and USG assessment in follow-up as stated.
Conclusions
Our study findings suggest that for management of large and impacted proximal ureteric stones, the combined mini-ECIRS offers the best option to render the patient stone free by a single intervention with better intra and immediate postoperative outcomes. Furthermore, the safety profile seen in our study paves the way for Mini-ECIRS to be done as an ambulatory procedure.
Footnotes
Authors' Contributions
D.K.M.: Conceptualization (lead); writing—original draft (lead); and writing—review and editing (equal). M.S.A.: Methodology (lead); conceptualization (supporting); and review and editing (equal). M.S.: Software (lead); and writing—review and editing (equal). K.N.: formal analysis (lead); and writing—review and editing (equal). Z.H.B.M.: Conceptualization (supporting); and writing—review and editing (equal). V.G. Writing—original draft (supporting); writing—review and editing (equal); and formal analysis (supporting).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.