
Abstract
Introduction:
Prostate cancer diagnosis and treatment is challenging in surgically complex patients. Radical prostatectomy can be performed without peritoneal entry using novel single-port (SP) transperineal (TP) and transvesical (TV) approaches. We sought to examine the outcomes of radical prostatectomy using novel TP and TV approaches in patients with extensive prior abdominal surgeries.
Materials and Methods:
From 2019 to 2023, 51 patients with extensive prior abdominal surgeries were identified who underwent TP (18) and SP TV (33) robotic radical prostatectomy. Indications included history of various surgeries with open laparotomy, including J-pouch reconstruction (22, 43%), active stoma (14, 27%), and open bowel resection (9, 18%). In all patients, 12/51 (24%) had a history of incisional hernia repair with mesh. A retrospective analysis was performed.
Results:
All cases were completed without open conversion, bowel injuries, or blood transfusions. Length of stay was 5.6 hours for TV and 22 hours for TP. No opioids were prescribed in 91% of TV vs 56% of TP. One intraoperative complication (ureteral injury) occurred in a patient undergoing the TP approach. Postoperative complications were noted in 14/51 (27%), including 10/18 (56%) TP vs 4/33 (12%) TV. High-grade complications (Clavien 3) occurred in three patients (6%, all TP). Pathologic staging showed pT3 in 26/51 (17 TV vs 9 TP), while the remainder were pT2. Biochemical recurrences were noted in four patients (8%, three TV and one TP). Immediate continence was noted in 30% of TV patients. Long-term continence after 12 months was 92% in TV and 67% in TP.
Conclusions:
In patients with extensive prior abdominal surgeries, radical prostatectomy is feasible using a TP or TV approach. No bowel injuries or open conversion were observed. The SP TV approach offers advantages of shorter hospital stay, shorter catheter duration, less opioid use, fewer complications, and improved continence recovery.
Introduction
Robot-assisted radical prostatectomy (RARP) is the standard of care for surgical management of localized prostate cancer, but is challenging in patients with extensive prior abdominal surgeries with dense intra-abdominal adhesions. 1 The impact of prior abdominal surgery on transperitoneal laparoscopic or robotic prostatectomy has been evaluated previously, with multiple studies showing no increase in complications or substantial increase in operative time. 2 –5 The majority of these studies include patients with a history of common laparoscopic or open procedures, with few studies specifically evaluating patients with a hostile abdomen or frozen pelvis from extensive prior surgeries. 6 –8
Approved by the FDA in 2018, the purpose-built DaVinci single-port (SP) robotic platform allows for surgery to be performed in confined spaces, including various natural orifice and tunneling procedures, which are either not possible or prohibitively difficult using a multiport robotic approach. 9 –11 Recently, single-site and SP-RARP has been performed using several extraperitoneal techniques, including transperineal (TP), retropubic extraperitoneal (EP), and transvesical (TV) approaches. 12 –17 The TP and TV approaches, in particular, have been utilized in patients whose abdominal cavities are otherwise inaccessible due to scar tissue from extensive prior abdominal surgeries. We sought to evaluate the outcomes and study the safety and efficacy of these approaches in patients for whom intraperitoneal surgery was not possible or contraindicated.
Materials and Methods
From March 2019 to February 2023, a total of 32 patients underwent SP TP RARP and 169 patients underwent SP TV RARP by a single surgeon (J.H.K.) at a single tertiary academic referral center. Of these, 51 patients were identified with extensive prior abdominal surgeries who qualified as having a hostile surgical abdomen. Indications for inclusion were the presence extensive abdominal scarring on documented physical examination and a history of multiple surgeries performed through an open laparotomy, including J-pouch reconstruction (22, 43%), history of ileostomy or colostomy (14, 27%), and open bowel resection (9, 18%). Patients had a median of three abdominal surgeries per person with a range of two to nine procedures. In all patients, 12/51 (21%) had a history of abdominal incisional hernia repair with mesh.
The Hostile Abdomen Index (HAI) is a prediction tool for perioperative bleeding and enterotomy, with high risk associated with values of 3 or 4 (Fig. 1). 18 In this population, all patients had a preoperative HAI of 3 (22%) or 4 (78%). In the majority of cases, patients were referred in the context of anticipated difficult surgical access related to known or presumed intra-abdominal adhesions. Patient characteristics and demographic information were collected with special attention to surgical history. Patients with unclear or incomplete surgical histories were excluded. All data were prospectively collected in an IRB-approved database and a retrospective analysis was performed.
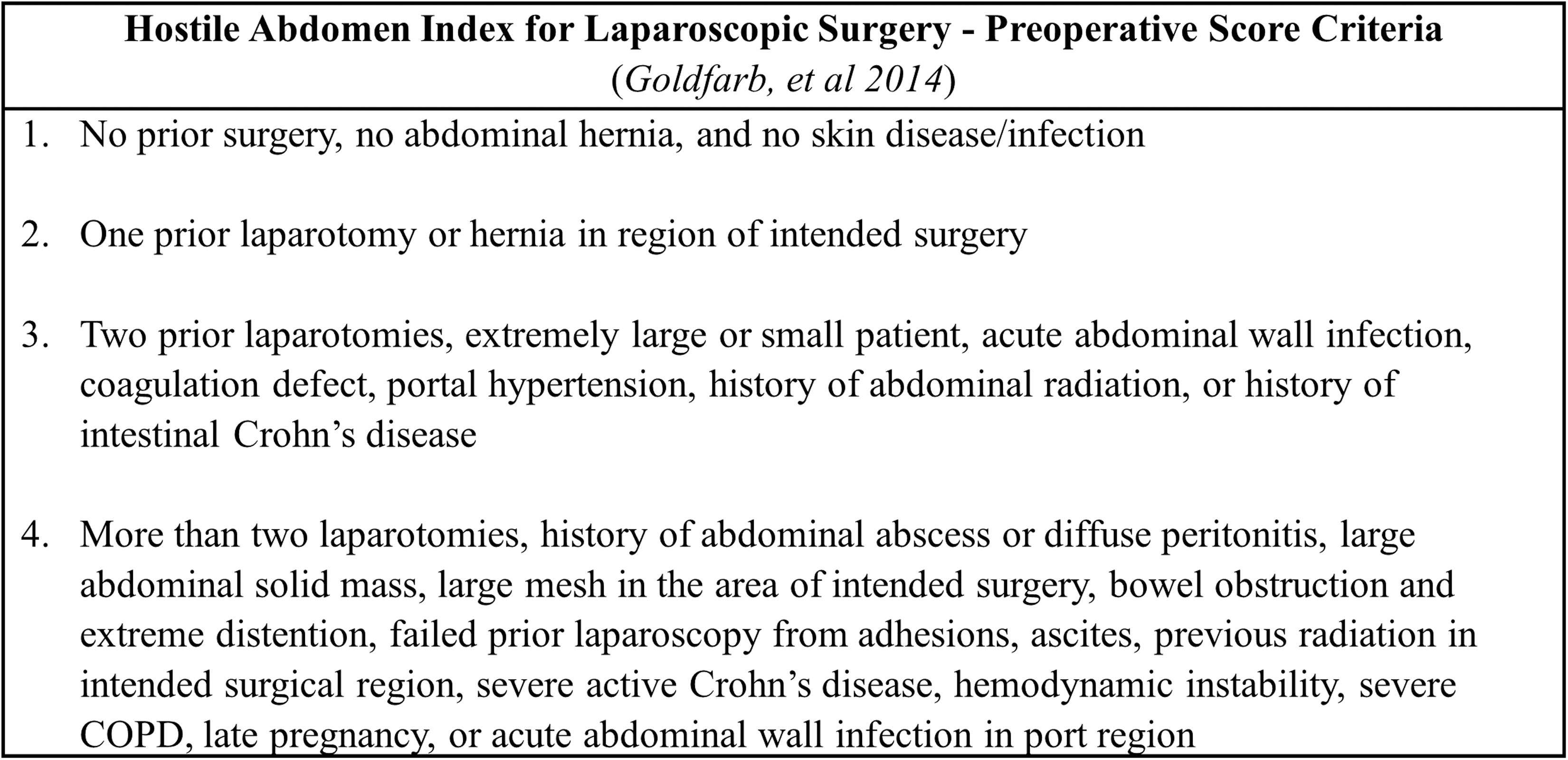
Preoperative Scoring Criteria for Hostile Abdomen Index for laparoscopic surgery as described in Goldfarb et al. 18
TP and TV radical prostatectomy were performed as previously described using the DaVinci SP robotic surgical system (Intuitive Surgical, Inc., Sunnyvale, CA). 13,17 TP access is obtained and a Gel Port is placed through the perineal incision, allowing for robot docking (Fig. 2B). TV access is obtained through a 3 to 4 cm suprapubic midline incision (Fig. 2C). A small cystotomy is created after aspirating fluid from the bladder. An access port is placed directly into the bladder, which allows for SP robot docking. Both approaches are extraperitoneal and allow for avoidance of intra-abdominal adhesions related to prior surgeries (Fig. 3). Both approaches utilize the floating dock technique, which allows for increased working space when the target anatomy is <10 cm from the incision site. 19 Insufflation is maintained at 8 to 12 mm Hg and limited to the perineum and within the bladder in these approaches.
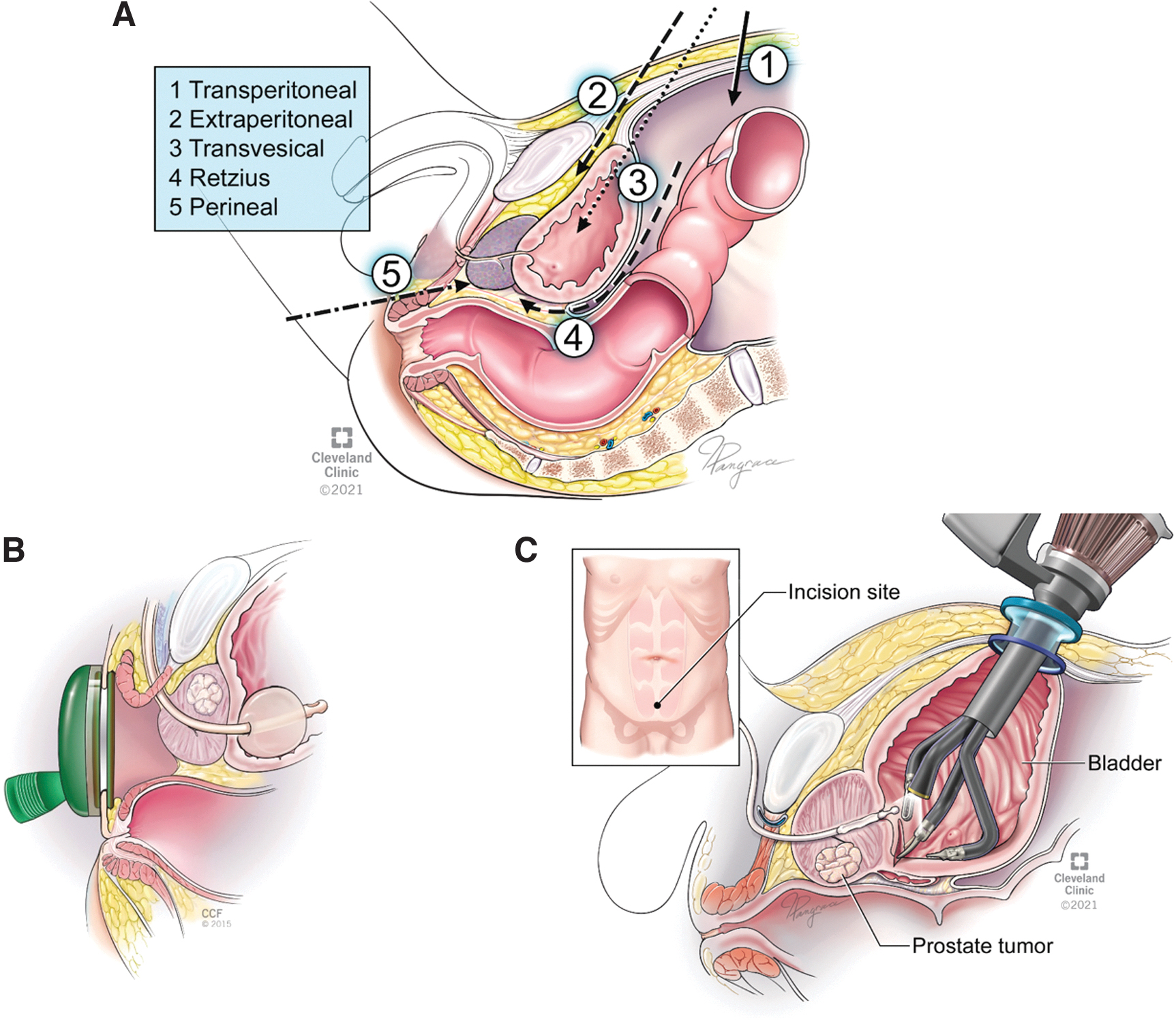
Various approaches are possible for prostate access when performing robotic radical SP robotic radical prostatectomy
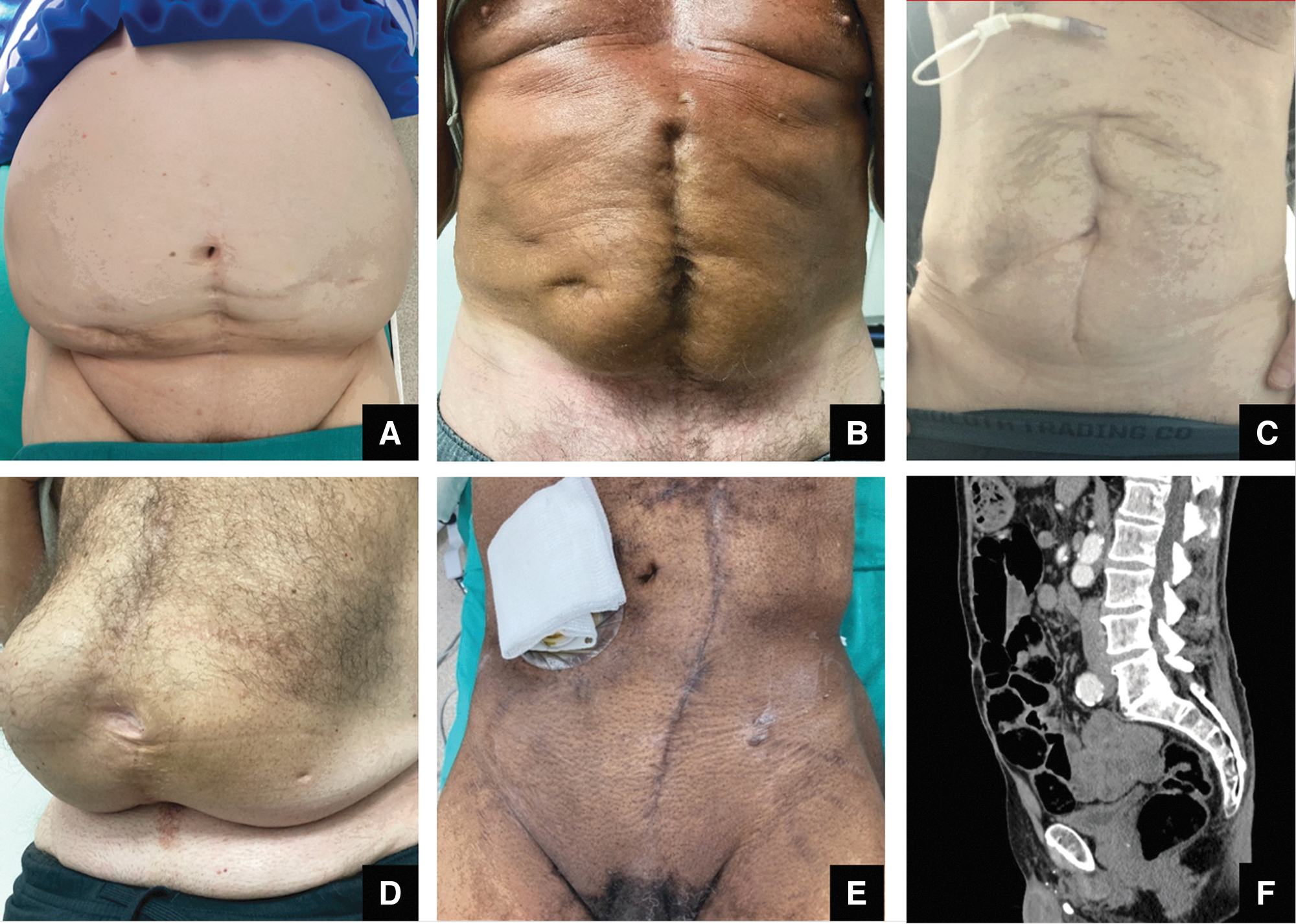
Examples of typical incision sites for patients with a hostile abdomen, including dense abdominal scars and prior stoma sites
Intraoperative and postoperative data were collected prospectively. Biochemical recurrence was defined as PSA ≥0.2 after radical prostatectomy. Urinary continence was defined as requiring one security pad or less per day. Postoperative complications were defined using the Clavien-Dindo classification system. 20
Categorical variables were reported as frequencies and proportions. Continuous variables were reported using median and interquartile range (IQR). Statistical significance was determined at a p-value of <0.05 using chi-square and Fisher's exact tests for categorical variables and Mann–Whitney U for continuous variables. Statistical analysis was performed using R version 3.6.1 (The R Foundation for Statistical Computing, Vienna, Austria).
Results
A total of 51 patients with a hostile surgical abdomen were included, with 33 undergoing SP TV RARP and 18 undergoing SP TP RARP. Baseline demographic characteristics are summarized in Table 1. The median follow-up duration was 6 months for SP TV and 16.5 months for SP TP. A total of 27 patients (53%) had a history of inflammatory bowel disease (52% SP TV and 56% SP TP). When comparing approaches, significant differences were noted in median prostate size on preoperative imaging (38 g in SP TV vs 27.6 g SP TP, p < 0.05), time from biopsy to surgery (136 days SP TV vs 98 days SP TP, p < 0.05) and follow-up duration (6 months SP TV vs 16.5 months SP TP, p < 0.05). There were no statistical differences in patient age, race, comorbidities, surgical history, preoperative functional status, or oncologic characteristics.
Demographics and Preoperative Patient Characteristics
ASA = American Society of Anesthesiology; BMI = body mass index; IPSS = International Prostate Symptom Score; IQR = interquartile range; NCCN = National Comprehensive Cancer Network risk; PSA = Prostate-Specific Antigen; SBO = Small bowel obstruction; SHIM = Sexual Health Inventory for Men.
Perioperative and postoperative outcomes are summarized in Table 2. All cases were completed without extra ports or open conversion. No intraoperative bowel injuries occurred and there was one (2%) intraoperative complication for the entire series (recognized left ureteral injury during SP TP RARP). The median (IQR) estimated blood loss was 75 mL (50–100) and no intraoperative or postoperative blood transfusions were required. Postoperative drains were used in three patients (6%). One in the first TP case as a precaution, and the remaining two for procedures with difficult anastomosis. A total of six patients (12%) required readmission. For the entire series, 30-day postoperative complications occurred in 14 (27%) patients, of which 11 were (22%) low-grade (Clavien 1, 2) and 3 (6%) were high-grade (Clavien 3) complications.
Perioperative and Postoperative Outcomes
Continence defined as 1 pad per day for security or less.
All Clavien 3 complications occurred in the SP TP approach and consisted of urine leak requiring suprapubic catheter insertion, urine leak with cystoscopy for foley catheter replacement, and percutaneous drain insertion for an infected lymphocele.
When comparing the outcomes of TV and TP approaches, there were significant differences in operative time, hospital length of stay, opioid prescription use, foley catheter duration, and postoperative complications, all in favor of the TV approach. While not statistically significant, positive margins were less frequent in the TV approach (39% vs 56%, p = 0.27) and positive margins were significantly more likely to be limited to <3 mm in the TV approach (10/13 limited in TV vs 3/10 limited in TP, p < 0.05). Oncologic outcomes were similar between groups and biochemical recurrence was observed in four patients during the follow-up period (three SP TV and one SP TP, p = 1.0). Immediate recovery of urinary continence was achieved in 30% of SP TV patients. Urinary continence was significantly higher in SP TV at 6 weeks (51% SP TV vs 17% SP TP, p < 0.05).
Although not statistically significant, continence remained higher throughout follow-up in SP TV and at 12 months, 92% of SP TV patients were continent vs 67% of TP patients (p = 0.09). There was no significant difference in recovery of erections in previously potent patients at 12 months (2/4 SP TV vs 7/14 SP TP, p = 1.0).
Discussion
Prostate cancer diagnosis and treatment can be problematic in patients with extensive prior abdominal and pelvic surgery, particularly those with a history of multiple bowel surgeries and inflammatory bowel disease. 8,21,22 In certain patients, intraperitoneal access to the prostate is not possible due to dense adhesions or a frozen pelvis. 7 Furthermore, previous violation of the retropubic space may limit the application of an extraperitoneal retropubic approach. In this series, we carefully selected patients with the most severe abdominal scarring from prior intra-abdominal open surgery who underwent robotic radical prostatectomy using TP and transvesical access.
Several prior studies have shown the feasibility and safety of robotic radical prostatectomy in patients with a history of aborted open radical prostatectomy 7,23 or prior abdominal surgery, citing no increase in complications and insignificant increase in operative time. 2 –5,24 An important consideration, however, is that patients with prior abdominal surgery included those with only laparoscopic or inguinal procedures, such as laparoscopic appendectomy, laparoscopic cholecystectomy, orchiectomy, and inguinal or umbilical hernia repair. In one series, lysis of adhesions was not required in up to 76% of patients with a history of prior abdominal surgery. 3 For patients requiring lysis of adhesions, a mini laparotomy incision was utilized and partially closed before robot docking, which may obviate advantages of a minimally invasive approach. 3,6
In our study, indications for inclusion were patients with severe visible abdominal scar tissue combined with an extensive or complex history of open abdominal surgery, including J pouch reconstruction (43%), bowel resection with ileostomy or colostomy (27%), open bowel resection (18%), and previous aborted radical prostatectomy for dense adhesions (4%). In all patients, 12/51 (24%) had a history of abdominal incisional hernia repair with mesh. Among the excluded patients in our study were those who often had made up most patients in the treatment arm of other studies, including those with one prior abdominal surgery consisting of inguinal hernia repair, appendectomy (open or laparoscopic), upper abdominal (hepatic, biliary, or gastric) procedures, and endoscopic or laparoscopic bowel procedures.
Despite complexity, there were no instances of open conversion, blood transfusions, or bowel injuries in this series. One intraoperative ureteral injury occurred during the left pelvic lymph node dissection for the first SP TP RARP in the series, which was recognized and repaired by ureteroureterostomy with ureteral stenting. On follow-up after stent removal, there was no evidence of hydronephrosis. The majority of reported postoperative complications (11/51, 22% overall) were low grade, most commonly consisting of urine leak (n = 5), urinary retention (n = 4), and ileus (n = 2). Notably both patients with ileus had a long history of intermittent spontaneous ileus predating surgery. High-grade complications occurred in 3/51 patients (6% overall), all of which were from the SP TP group. A total of six (12%) patients were readmitted after initial discharge (2/33 TV vs 4/18 TP, p = 0.17).
It is important to highlight the significant differences in outcomes when comparing the TV and TP approaches. The TV approach was associated with statistically significant improvements in operative time (206 minutes vs 245 minutes), length of hospital stay (5.6 hours vs 22 hours), opioid prescription requirement (9% vs 44%), complication rate (12% vs 56%), and foley catheter duration (5 days vs 10 days). Pathologic staging showed pT3 in 26/51 or 51% overall (51% TV vs 56% TP) and the remainder were pT2. Negative margins were achieved in 55% overall (61% TV vs 44% TP). Despite no significant differences in rates of extraprostatic extension (p = 0.92) or positive margins (p = 0.27), nonlimited positive margins (>3 mm) were significantly less frequent in the TV approach (3/13 TV vs 7/10 TP).
Although speculative, factors contributing to positive margins may be related to iatrogenic false positives from difficult dissection or specimen extraction, delayed time from biopsy to treatment (median 135 days), or high rate of pT3 disease in this population. Immediate continence was 30% for the TV approach and overall continence for the TV approach exceeded 90% at 12 months compared to 67% in the TP approach. Oncologic outcomes, including the pathology Gleason Grade, TNM stage, and rates of biochemical recurrence, were similar between groups. Erection recovery in previously potent patients was also similar between groups.
Specific situations were encountered in this patient population that present special challenges. While not a contraindication, prostate glands larger than 80 g are challenging in either approach. In patients with previous bladder surgery, history of pelvic radiation, or abdominopelvic resection, the bladder anastomosis may be especially difficult and may be on significant tension. This can lead to prolonged catheter duration and impair continence recovery postoperatively. In both approaches, the pelvic lymph node dissection is feasible, but more challenging than in the retropubic approach and an extended node dissection is not possible in most cases. In the TV approach, only a limited pelvic lymph node dissection is feasible.
In the TP approach, the node dissection is challenging and was associated with one of three reported high-grade complications and the only intraoperative complication (ureteral injury) in this series. Therefore, patients undergoing TP or TV RARP with a hostile abdomen and high-risk localized disease should be counseled that lymph node sampling may be insufficient or increase complication risk.
Our study has several limitations to acknowledge. The difference in median (IQR) follow-up for TV and TP approaches was 6 months (3–12) and 16.5 months (7–30), respectively. This is because the TV approach is a relatively new technique by comparison. While this may limit some conclusions regarding long-term functional and oncologic outcomes, the analysis of intraoperative and perioperative outcomes is not impacted. Next, all procedures were performed by a single experienced surgeon with extensive SP and multiport robotic experience at a single tertiary academic center, which may limit the generalizability of results. Furthermore, there is no published learning curve for either approach and the SP TP approach remained particularly challenging after a total of 29 total procedures performed at our institution.
In addition, the lack of a control arm may limit conclusions, although comparison to a standard transperitoneal multiport robotic approach without a laparotomy was not possible in this group based on inclusion criteria. We attempted to extract data from a historic institutional database of prostate cancer patients undergoing open radical prostatectomy, but reliable information for surgical history and physical examination findings was not available. Furthermore, the goals of this publication were to report the outcomes of two minimally invasive approaches and not for comparison of this cohort with the general population undergoing RARP.
We also acknowledge the heterogeneity of patient presentations leading to a hostile surgical abdomen. To account for this, we included only patients with complete surgical histories demonstrating prior multiple prior open intra-abdominal surgeries combined with physical examination findings demonstrating visible dense abdominal scarring and/or active stoma site. Based on criteria set forth in the HAI for Laparoscopic surgery (scale of 1 to 4), all patients included in this study are considered high risk for bleeding or enterotomy with laparoscopic surgery. 18 Also, depressed scar tissue documented on physical examination has previously been shown to predict intra-abdominal adhesions. 25
This study provides evidence that SP TP and TV radical prostatectomy are not only feasible, but indicated in patients with a hostile abdomen from prior abdominal surgeries in whom intraperitoneal approaches may be dangerous or impossible. Given the high rates of bowel reconstruction and inflammatory bowel disease in this patient population, surgery is often preferred over radiation therapy. 21 On comparison, the SP TV approach showed significant improvements in complication rate, faster recovery, and shorter foley catheter duration. As a result, for surgeons with sufficient experience, the SP TV approach should be the preferred surgical treatment modality in this patient population.
Conclusions
In patients with extensive prior abdominal surgeries and a hostile abdomen, radical prostatectomy is feasible using a TP or TV approach. Neither approach was associated with an increased rate of open conversion or bowel injury. Compared to the TP approach, the SP TV approach offers advantages of shorter hospital stay, shorter catheter duration, less opioid use, fewer complications, and improved continence recovery.
Footnotes
Authors' Contributions
Conceptualization and Design: E.L.F. and J.K. Data Acquisition: E.L.F., R.R.-C., N.S., J.S.C., and A.G. Analysis and Interpretation of Data: E.L.F. Drafting of Article: E.L.F. Critical Revision of Article: J.K. and R.R.-C. Statistical Analysis: E.L.F. Obtaining Funding: N/A. Administrative, Technical or Material Support: N/A. Other: N/A.
Author Disclosure Statement
J.K. is a speaker for Intuitive Surgical, Inc., and is a consultant for VTI.
Funding Information
No funding was received for this article.