
Abstract
Introduction:
Understanding the factors that influence the decision of urology residents to pursue an Endourology Society (ES) fellowship and the criteria used by applicants to rank programs may help residents and program directors (PDs) optimize the match process. In the present study, we surveyed current ES fellows to gain better insight surrounding their decision-making process.
Materials and Methods:
A survey was emailed to all ES fellows, comprising Endourology and Stone Disease (ESD), Laparoscopic and Robotic Surgery (MIS), and combination of ESD/MIS (COM) programs. A Likert scale ranging from 1 to 5 was used. The survey captured demographics such as geographic region, program type, duration, applicants' reasons for pursuing fellowship, criteria for ranking programs, and perceived improvements in surgical comfort levels at the end of their training.
Results:
Out of the 60 fellows who were surveyed, 40 (66.7%) responded. Among the respondents, 9 (22.5%) pursued ESD, 10 (25%) pursued MIS, and 21 (52.5%) pursued COM programs. The primary reason for seeking a fellowship was to improve surgical skills while increasing earning potential and enhancing research opportunities were deemed the least important. Fellows enrolled in 1-year programs were less likely to pursue fellowships for academic reasons. The two most significant factors in selecting a program were both related to gaining operative experience. Lastly, there was an increase in the level of comfort performing all endourological surgeries independently after fellowship.
Conclusions:
ES fellowship is seen as an opportunity to hone surgical skills and increase job competitiveness. When selecting a program, operative experience is the most important factor, and fellowship improves operative confidence. The information obtained from this study may mutually help guide future applicants and PDs in the decision process of the Endourology Match.
Introduction
The Endourology Society (ES) accredits advanced fellowship training programs in complex stone disease and minimally invasive surgery. Each year, urology trainees from around the world participate in the Endourology Fellowship Match to pursue fellowship training among one of three pathways: Endourology and Stone Disease (ESD), Laparoscopic and Robotic Surgery (MIS), or a combination of ESD/MIS (COM). Accredited programs may offer a 1- or a 2-year track within these disciplines. According to data from the 2022 application cycle, 47 out of 85 applicants successfully matched into fellowship (55%), and there were 10 unfilled fellowship positions out of 57 (17.5%). 1
Given the significant number of unmatched applicants and unfilled fellowship positions, it is important to understand the factors influencing decision making by the primary stakeholders in the match process: applicants and program directors (PDs). In a previous study, we evaluated factors utilized by PDs to select applicants and evaluate current fellows. 2 However, to our knowledge, no published studies have evaluated program selection criteria used by fellowship applicants. Such applicant-level data, particularly when compared with corresponding PD-level data, may inform applicants and PDs alike regarding the factors guiding decision making in the match process. This would provide transparency to a historically opaque admission process and help facilitate higher match rates and fewer unfilled positions.
To this end, we sought to investigate the personal and professional factors that drive applicants to pursue an endourology fellowship. Additionally, we evaluated how applicants decide where to apply and how they rank those programs. Lastly, we assessed current fellows' assessment of their perceived improvement in surgical competency at the conclusion of their fellowship.
Materials and Methods
Survey design
Following IRB approval (IRB# 22-00216), we created an anonymous survey using our institution's Research Electronic Data Capture database. The main portion of the survey was composed of four key questions: (1) “How important are the following reasons regarding your decision to complete an endourology fellowship,” (2) “Rank the following components of the fellowship application based on how important you thought they were to the programs to which you applied,” (3) “Rank the following in terms of degree of importance to you in selecting a fellowship program,” and (4) “Rank the following criteria in terms of perceived degree of importance to your program when evaluating you in your current role as fellow.” A 1–5 Likert scale (1 = not important, 5 = extremely important) was used for responses. Of note, questions (2) and (4) were similar to those asked of PDs in our prior study. 2 For question (1), possible reasons for pursuing a fellowship were: to become a better surgeon, increase competitiveness for a future job, pursue a field I am passionate about, improve career satisfaction, pursue an academic career, increase earning potential, and improve research skills.
Reasons for program selection (question [3]) included: quality of operative experience, case volume, “fit” within program, quality/prestige of faculty, quality/prestige of institution, initial interview, length of program, advisor/mentor recommendation, level of interest from the program, geographic location, recommendations by former program graduates, research opportunity, dedicated research block, and second look/site visit.
Participants were also asked to grade their comfort level performing key endourological operations independently at the end of their residency training as well as at their current level of fellowship training (fellows in the first year of a 2-year program were not given the option to answer this question; thus, everyone who responded to this question was at the tail end of their fellowship training). Again, a 1–5 Likert scale was used for responses (1 = not comfortable at all, 5 = extremely comfortable). Participants were only given options to grade surgical comfort levels for procedures specific to their type of program (for example, those in ESD programs were not given the option to grade robotic or laparoscopic procedures).
Survey distribution
The survey was approved by the Fellowship Committee of the ES. A complete list of currently registered fellows was obtained, and the ES distributed a link to the survey through email to each eligible participant individually. Both first and second-year fellows were surveyed in the 2021–2022 academic year. All fellows surveyed participated in the ES Match; however, some did not match and secured positions through other means. The survey was conducted from April 2022 to June 2022.
Data analysis
Our data were analyzed using a similar methodology to that described previously in our study of ES PDs. 2 In brief, given the small overall number of ES fellows, our ability to perform meaningful comparative statistical analysis was limited (even with a high respondent rate). Thus, our strategy focused on descriptively analyzing our data. We utilized centered bar charts showing the percentage of responses for each question for the respective Likert questions. This analysis was performed for all respondents. Results were plotted using the “Likert” package for R statistical software v3.6.2. 3,4
Results
Fellow demographics and responses to non-Likert questions
Of the 60 fellows registered with the ES, 40 (66.7%) participated in the survey. Respondent demographics and responses to non-Likert questions are summarized in Table 1. The breakdown of respondents by program discipline included 9 ESD fellows (22.5%), 10 MIS fellows (25.0%), and 21 COM fellows (52.5%). The breakdown of respondents by program duration was 14/39 (35.9%) 1-year fellows and 25/39 (64.1%) 2-year fellows (one respondent of the 40 did not answer this question). Of the 40 respondents, 34 (85.0%) secured their position through the Endourology Fellowship Match, while 6 (15.0%) failed to match and secured their position through other means. Most respondents applied to between 4 and 7 programs and attended between 4 and 7 interviews. Most respondents matched into their first-choice program (23/40, 57.5%).
Respondent Demographic Data
AUA = American Urologic Association; N/A = Not Answered.
Few respondents held additional advanced degrees (4/40, 10.0%) or performed a second-look site visit to the program at which they eventually matched (6/34, 17.6%). Programs from all sections of the American Urologic Association (AUA) were represented, with the North Central section having the most significant number of respondents (10/38, 26.3%). Only 2 out of 39 (5.13%) respondents indicated they were performing fellowship in the same state as their residency program. Most respondents (21/40, 52.5%) had plans to pursue careers in academic urology (Table 1).
Reasons for performing endourology fellowship
Overall, the two most important reasons for performing an endourology fellowship were to improve surgical skills and to increase competitiveness for future employment. Least important reasons included improving research skills/obtaining more publications, pursuing an academic career, and increasing earning potential. When stratified by program duration, fellows in 2-year programs seemed to have greater interest in pursuing academic careers and improving research status, while those in 1-year programs appeared more driven by increasing career earning potential (Fig. 1).
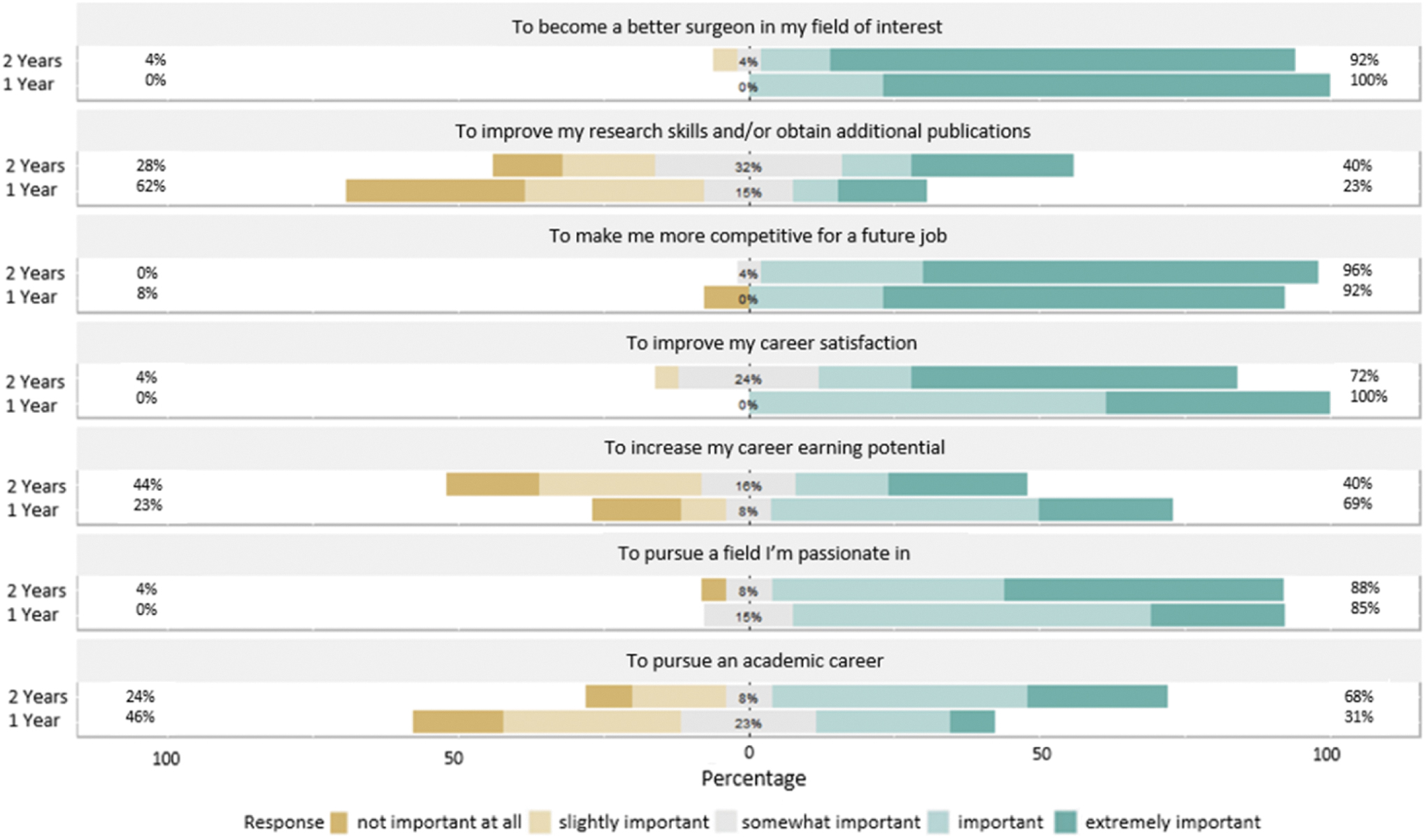
Responses to survey question in which respondents were asked: “Please rank the following statements based on the degree to which they apply to your reasons for deciding to complete an endourology fellowship.” Responses are divided into those enrolled currently in 1- and 2-year programs.
Perceived importance of applicant qualifications
Respondents believed the following qualities were the most important to programs in which they applied: level of interest from the applicant, “fit” of an applicant in the program, and initial interview. Conversely, qualities of lowest importance included advanced degrees, quality of applicant's undergraduate institution and medical school, number of presentations at national meetings, geographical location of applicant's residency, post interview ‘thank you’ email, and second-look site visits (Fig. 2).
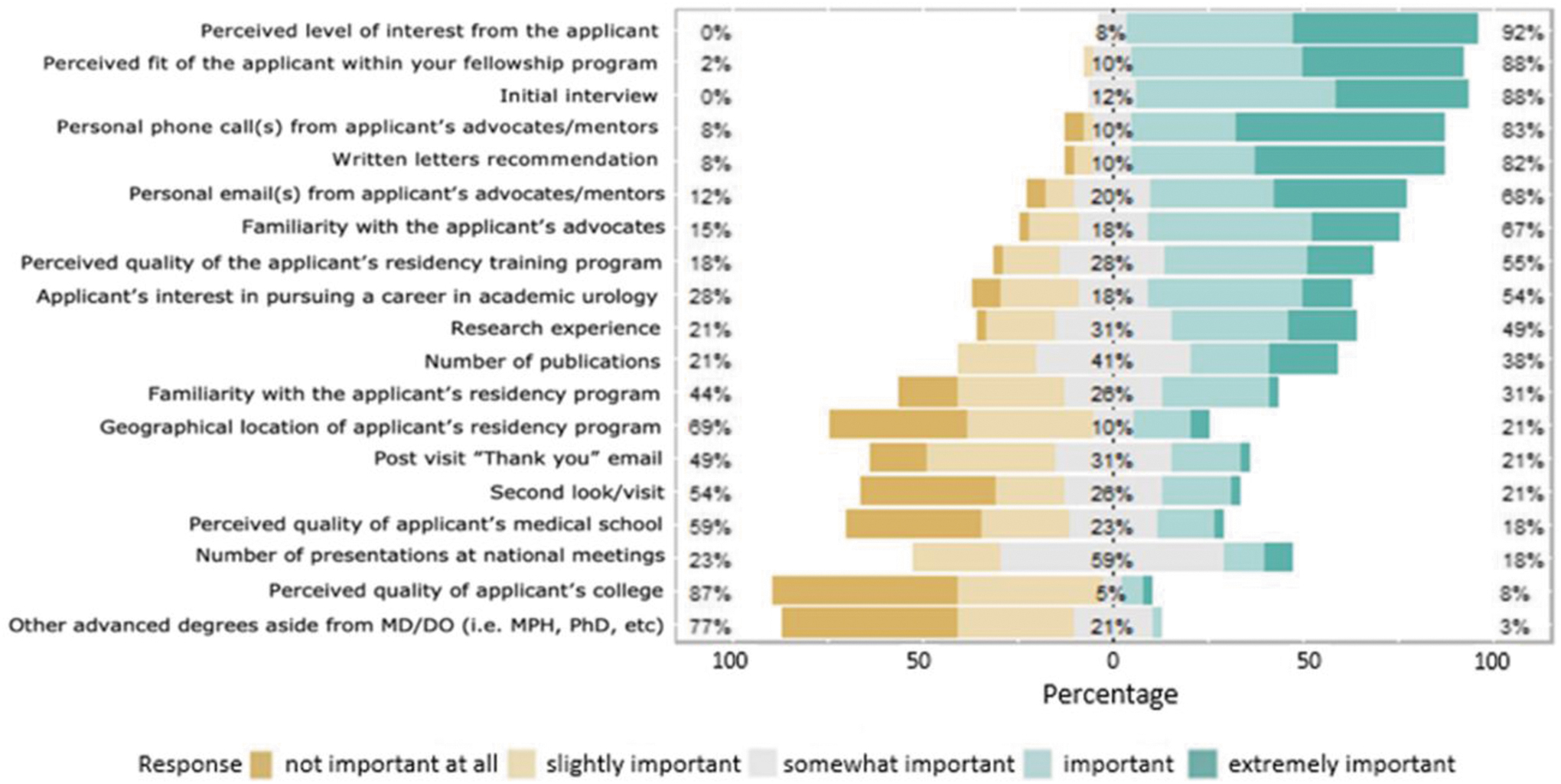
Responses to survey question in which respondents were asked: “Please rank the following components of the fellowship application based on how important you thought they were to the programs to which you applied.”
Selecting the right fellowship program
Respondents were most concerned about the quality of operative experience and the volume of procedures performed when ranking fellowship programs. Respondents also highly valued their perceived “fit” within the program and the quality/prestige of the faculty. A second-look site visit was the least important factor in selecting a fellowship. Similarly, a dedicated research block and the ability to perform research at the institution were also of relatively low importance in the program selection process (Fig. 3).
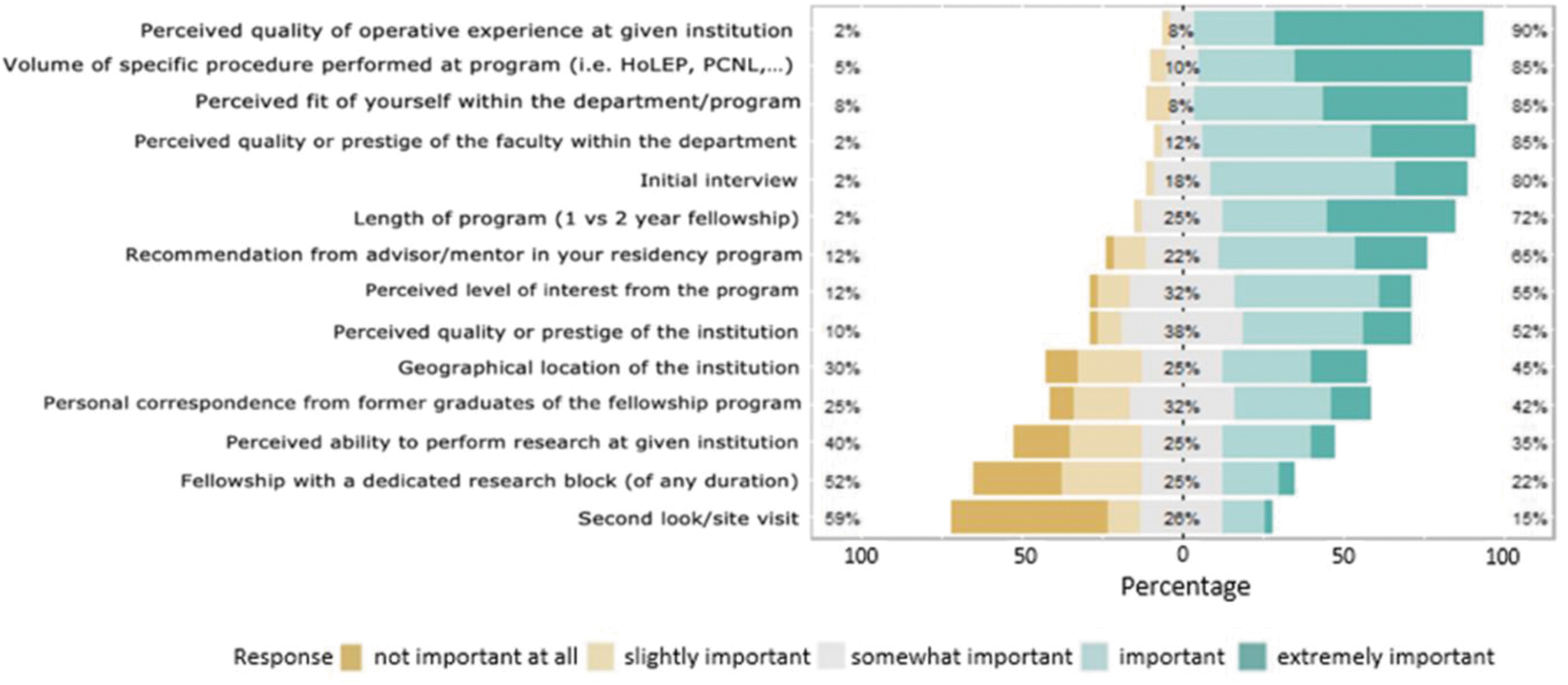
Responses to survey question in which respondents were asked: “Please rank the following in terms of degree of importance to you in selecting a fellowship program.” HoLEP = holmium laser enucleation of prostate; PCNL = percutaneous nephrolithotomy.
Fellow evaluation
Respondents felt they were being evaluated by their PDs based on their clinical and interpersonal skills more than their academic productivity. The two criteria that fellows believed most important to their evaluations were operative skills and attitude/demeanor (Fig. 4).
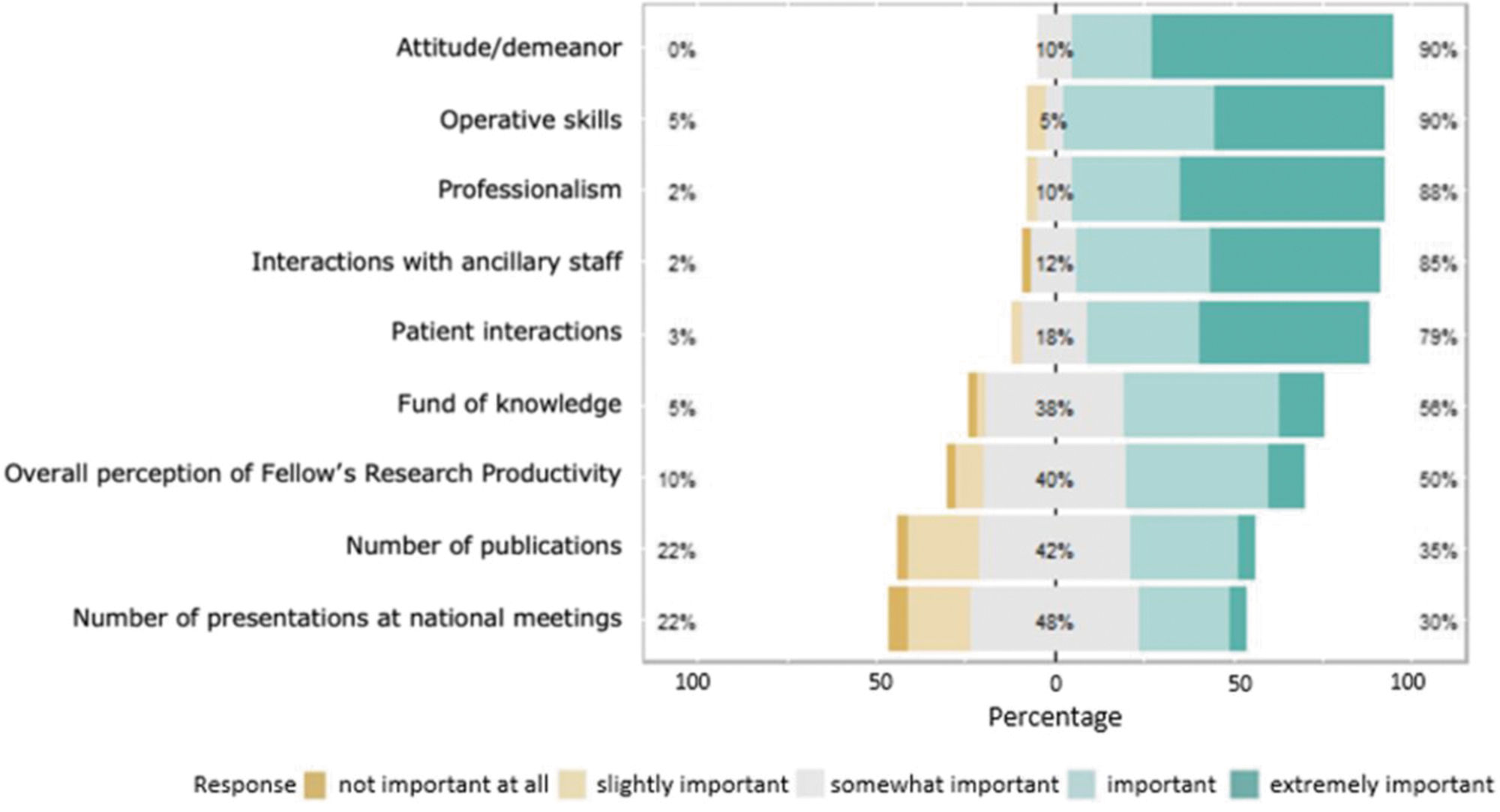
Responses to survey question in which respondents were asked: “Please rank the following categories in terms of perceived degree of importance to your program when evaluating you in your current role as fellow.”
Procedural comfort level
When asked to rank comfort level performing specific endourological procedures independently, there was an overall increase in comfort level across all procedures listed. The procedure with the most significant increase in comfort level between residency and fellowship training was laser prostate enucleation. There was a smaller yet substantial improvement in comfort levels for percutaneous nephrolithotomy and robotic/laparoscopic procedures, and a modest improvement with extracorporeal shock wave lithotripsy. Robotic retroperitoneal lymph node dissection (RPLND) and ureteroscopic laser lithotripsy (URSLL) had minimal improvements in comfort level even after fellowship training. Comfort levels for all procedures are outlined in Figure 5.
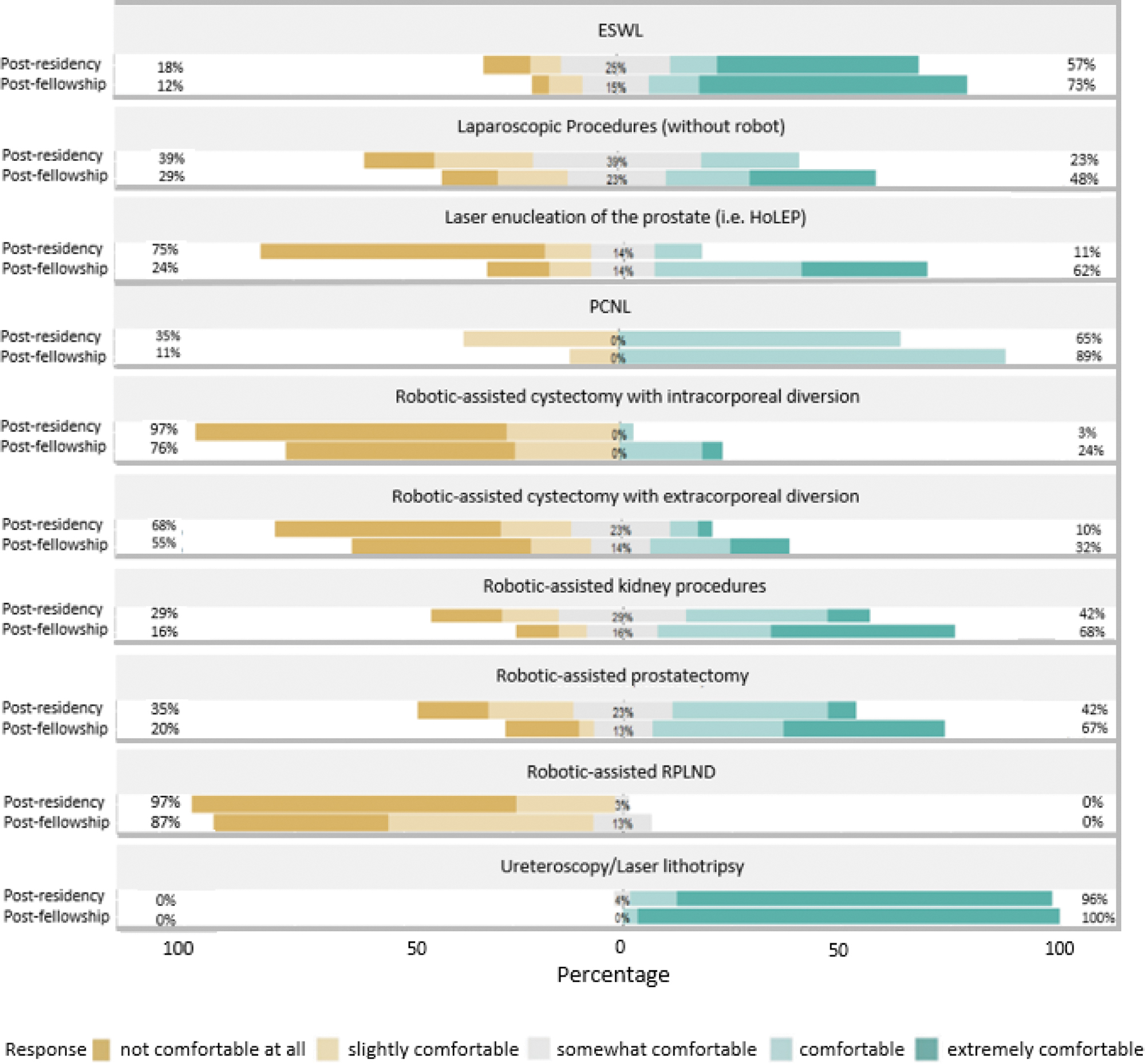
Responses to two consecutive survey questions in which respondents were asked: (1) “Please rank your comfort level performing operations independently at the end of your residency” (postresidency), and (2) “Please rank your comfort level performing operations independently now that you are at the end of your fellowship” (postfellowship). ESWL = extracorporeal shock wave lithotripsy; RPLND = retroperitoneal lymph node dissection.
Discussion
Fellowship training has become increasingly sought after as the practice of urology and medicine, in general, have become more specialized. Endourology fellowships are popular among contemporary urology trainees, and most training programs are organized by the ES and filled through the Endourology Fellowship Match. However, the considerable number of unmatched applicants and unfilled positions suggests a disconnect between applicants and PDs regarding expectations, values, and sentiments within the match process. Our previous study focused on PD perspectives on the importance of several criteria in selecting a fellowship candidate. Yet, applicant perspectives driving this selection process are largely unknown as no published applicant-level data on factors informing program selection and ranking for endourology or any urology fellowship discipline exists. Herein, we have performed the first study evaluating applicant perspectives on the factors influencing the decision to pursue fellowship and program selection in endourology.
PDs and applicants rate the same three factors as most important to the application process: “fit” within the fellowship program, initial interview, and applicant's demonstrated level of interest. 2 However, there were also noteworthy areas of discordance elicited. Contrary to PDs, who placed more weight on research experiences and presentations at national meetings, applicants weighed academic productivity as less of an essential factor in their application. Thus, increasing research productivity in residency may serve as an opportunity for applicants to strengthen their ES fellowship application. Furthermore, compared with PDs, applicants placed a higher value on the reputation and location of their training institutions and the credibility of their advocates, which may provide a false sense of security for applicants hailing from prominent institutions.
Despite the numerical differences in each criterion, the general rank order was similar for applicants and PDs across all categories, with one major notable exception being second-look site visits. While 49% of PDs viewed second-look site visits as important or extremely important, only 21% of applicants held similar sentiments. The emphasis on second-look site visits by PDs is understandable as these can be used as a proxy for determining how serious an applicant is in matching to that specific program. However, this may also create an undue burden for applicants as they are tasked with balancing the need to interview broadly while also executing their clinical duties in residency. The additional expenses associated with travel and lodging must also be considered. This burden is compounded for international and non-locoregional applicants. Thus, consideration should be given to codifying rules regarding second visits similar to existing regulations governing the AUA residency match. 5
Regarding perspectives on evaluation during fellowship, fellows and PDs generally shared similar views, as we observed similar elements of importance in rank order with two notable exceptions. First, fellows put less emphasis on funds of knowledge compared with PDs. Therefore, PDs should consider explicitly communicating the importance of continuing to develop a knowledge base throughout fellowship as a primary training goal. Second, fellows put less emphasis on patient interactions compared with PDs. The reasons for the discordance in this area of evaluation are not discernable from the present study, however, there are several possible explanations. The degree to which fellows interact with patients may vary widely between programs. Programs in which fellows spend most, if not all their time in the operating room, likely involve very little face-to-face patient interactions, whereas programs which incorporate the fellows into the office-based practice require more robust face-to-face interactions.
Similarly, the degree of direct attending physician oversight may vary widely between programs, and programs with a large portion of fellow “independence” may give PDs little opportunity to observe a fellow's patient interactions. It is possible that fellows that spend little to no time in the office or in the presence of the attending physician may believe that their patient interactions are less important in their evaluations. As with funds of knowledge, communication of expectations from PD to fellow is likely the key to eradicating the discrepancy in this area of evaluation.
To further inform residents who may be unsure whether to pursue a fellowship, we surveyed current endourology fellows on their motivations for doing so. Overall, respondents were most motivated by improving their surgical skills and enhancing their employment competitiveness. Despite the length of urology residency training, the ever-growing array of surgical competencies required to become a well-trained urologist may have resulted in a “dilution” of technical skills. Residents must now learn to perform more surgeries and possess more knowledge than ever before, yet residency duration has not changed to accommodate this. Furthermore, completing fellowship training allows one to declare themselves a subspecialist. As our health care system trends toward specialization, it is unsurprising that graduating residents may feel a push toward claiming their “urological niche” to secure a desirable job. Indeed, compared with their younger counterparts, urologists over the age of 45 are far less likely to have completed a fellowship. 6 To guide applicants debating between 1- and 2-year programs, responses for reasons to pursue fellowship were stratified by program duration.
There were several categories with notable differences, namely research productivity, desire to pursue an academic career, and increasing financial earning potential. These data suggest that applicants with a predisposition toward academic urology may want to pursue 2-year programs, while others may be better suited to a 1-year program.
There was an improvement across nearly all types of surgeries when comparing surgical comfort levels at the tail end of residency and fellowship for various procedures. Notable exceptions included URSLL and robotic RPLND. The minimal improvement in comfort level for URSLL is likely due to the ubiquitous use in academic training institutions, and residents likely have extensive exposure to this procedure. 7 On the contrary, we hypothesize minimal changes in comfort levels with robotic RPLND as this procedure may be outside of the scope of ES fellowships and more under the purview of oncological training.
Applicants prioritize clinical and surgical training over academic and scholastic opportunities when evaluating possible programs. Interestingly, the geographic location did not appear to be an essential criterion in the ranking process, which is corroborated by the fact that only two respondents conducted a fellowship in the same state as their residency program. Furthermore, candidates feel that the reputation of the faculty members is more important than the institution's reputation. This is likely due to candidates' perceptions that, besides superior instruction, prominent faculty may have a wider network, which may better position the applicant for job market competitiveness.
This study is not without limitations. To begin with, the entire cohort available to conduct this survey is small and hence may not be fully representative of the larger population. However, we believe the high respondent rate helps mitigate any inaccuracies induced by the limited sample size. Second, most respondents in their first year of fellowship at the time of the survey went through the application process during the initial COVID-19 pandemic lockdown, which may have significantly altered their application and interview experiences, and in turn, their sentiments in ranking programs. Similarly, second-year respondents may have missed some of their fellowship training due to the lockdowns, possibly altering their training experience. Finally, given the wide variability in program pathway and duration within the ES, there is potential that the sentiments depicted herein are overgeneralized or skewed to favor certain fellowship categories. Despite these limitations, the overall message to future applicants remains essentially unchanged.
Conclusion
Herein, we present the first study to assess applicant perspectives on factors influencing program selection and the decision to pursue an endourology fellowship. An endourology fellowship is largely viewed as an opportunity to improve surgical skills and job competitiveness. To improve match success, applicants should strongly consider performing second-look site visits and improving their academic productivity in residency. Furthermore, 2-year programs may better serve those inclined to pursue academic careers. Finally, a fellowship in endourology appears to improve surgical confidence significantly. The information obtained from this study may mutually help guide future applicants and PDs in the decision process of the Endourology Match.
Footnotes
Authors' Contributions
A.J.Y.—conceptualization, formal analysis, investigation, methodology, and writing. R.K.—conceptualization, formal analysis, investigation, methodology, and writing. J.A.K.—conceptualization, investigation, methodology, and writing. A.R.—visualization, writing, data curation, and methodology. B.G.—conceptualization, methodology, project administration, and resources. D.J.L.—formal analysis, data curation, and visualization. C.C.—visualization, data curation, and formal analysis. R.S.—visualization, data curation, and formal analysis. W.M.A.—conceptualization, methodology, and supervision. M.G.—conceptualization, methodology, formal analysis, writing, and supervision.
Author Disclosure Statement
M.G. is compensated for educational training for Cook Urological Incorporated, Boston Scientific Incorporated, Olympus Incorporated, Lumenis Incorporated, and Retrophin Incorporated. M.G. also serves as Editor-in-Chief of Video Urology. W.M.A. is compensated for educational training for Boston Scientific Incorporated. All other authors have no relevant disclosures.
Funding Information
No funding was received for this article.