
Abstract
Background:
Patients who have undergone renal transplant may have a concomitant benign prostatic hyperplasia (BPH), a condition that can potentially hinder the recovery of the renal graft and necessitate surgical intervention. However, endoscopic treatment of BPH should be performed carefully because of the associated perioperative risks. We aimed to systematically assess the factors affecting surgical indications and perioperative outcomes of BPH surgical treatment in renal transplantation (RT) recipients.
Methods:
A systematic literature search was performed on January 28, 2023, using Scopus, PubMed, and EMBASE with no date limit. Preclinical and animal studies, reviews, letters to the editor, case reports, and meeting abstracts were excluded.
Results:
Eighteen articles were accepted and included. Clinical BPH has a high incidence rate after RT, particularly in elderly men. Secondary events associated with BPH, such as acute urinary retention and urinary tract infections, can lead to a gradual decline of renal graft function and patient survival. BPH procedure can prevent these events and guarantee improvements in serum creatinine levels, voiding parameters, and lower urinary tract symptoms. When the urine culture is negative, the endoscopic procedure of the prostate may be performed within 1 month of the initial procedure, particularly in older patients, more prone to develop voiding dysfunction. Alternatively, a transurethral incision of the prostate may be recommended for patients with smaller prostates who wish to preserve ejaculatory function. Data on comparative BPH surgical procedures are lacking.
Conclusions:
BPH procedure should be offered in RT recipients who develop bladder outlet obstruction owing to BPH. Endoscopic treatment should be performed after a few weeks from RT to avoid further graft deterioration.
Introduction
Patients with chronic kidney disease or end-stage kidney disease (ESKD) frequently have concomitant lower urinary tract symptoms (LUTS). This clinical condition is associated with a sensory protein expression anomaly in the bladder urothelium, although there is no higher risk of decreased bladder capacity or anuria status. 1 Nevertheless, abnormal storage function and bladder outlet obstruction (BOO) occur in 71.0% and 51.6% of these patients, respectively. 2 Furthermore, patients with ESKD on regular dialysis treatment tend to develop LUTS more than people of the same age. 3 ESKD patients undergoing renal transplantation (RT) will continue to experience storage symptoms, such as frequency, nocturia, and urinary urgency, owing to a combination of high fluid intake, a denervated donor kidney, a long-term defunctionalized urinary bladder during dialysis, and psychosocial distress mostly. 4
Yet, men with RT and benign prostatic hyperplasia (BPH) require close monitoring because BOO may harm the recovery of the renal graft owing to an increase in postvoiding residual (PVR) urine, recurrent urinary tract infections (UTIs), and high voiding pressure, which may impair graft function. 5 In a cohort of 23,622 adult male renal recipients with a new diagnosis of BPH on post-transplant Medicare claims, an association between BPH and the risk of graft loss was noted. 6 Therefore, BPH diagnosis and timely management are mandatory to prevent graft deterioration. Medical therapy with α-adrenergic receptor-blocking agents, such as Doxazosin, has been found to influence renal graft function and improve blood pressure. 7 Nonetheless, transurethral resection of the prostate (TURP) is recommendable after RT in oliguric or anuric patients with BPH to minimize morbidity. 8
Historically, 3 months post-RT was considered the optimal interval for any surgical treatment for associated BOO to optimize the short- and long-term outcomes. 9 However, in some cases, an earlier BPH procedure is desirable to preserve graft function. 10
We aimed to perform a scoping review on factors associated with the need for BPH procedure and consequent surgical outcomes in kidney transplanted patients suffering from LUTS owing to BPH.
Evidence Acquisition
Literature search
Literature search was performed on January 11, 2023 using PubMed, EMBASE, and Scopus. The following term and Boolean operators were used: (surgery OR surgical procedures OR bladder outlet relief) AND (benign prostatic hyperplasia or BPH) AND (kidney transplant OR renal transplant OR renal graft).
Selection criteria
Preclinical studies were excluded. Retrospective, prospective, and prospective randomized studies were accepted. Reviews, letters to the editor, case reports, and meeting abstracts were excluded.
Study screening and selection
All retrieved studies were screened by two independent authors through Rayyan Intelligent Systematic Review (
Evidence Synthesis
Literature screening
Literature search found 351 articles. Twenty-two duplicates were automatically excluded. A total of 329 articles were screened against title and abstract. Among the latter, 305 articles were further excluded because they were irrelevant to the purpose of the present review. The remaining 24 full-text articles were further screened for appropriateness and 6 articles were excluded. Finally, 18 articles were accepted and included. 11 –28 Figure 1 provides the flow diagram of the literature search.
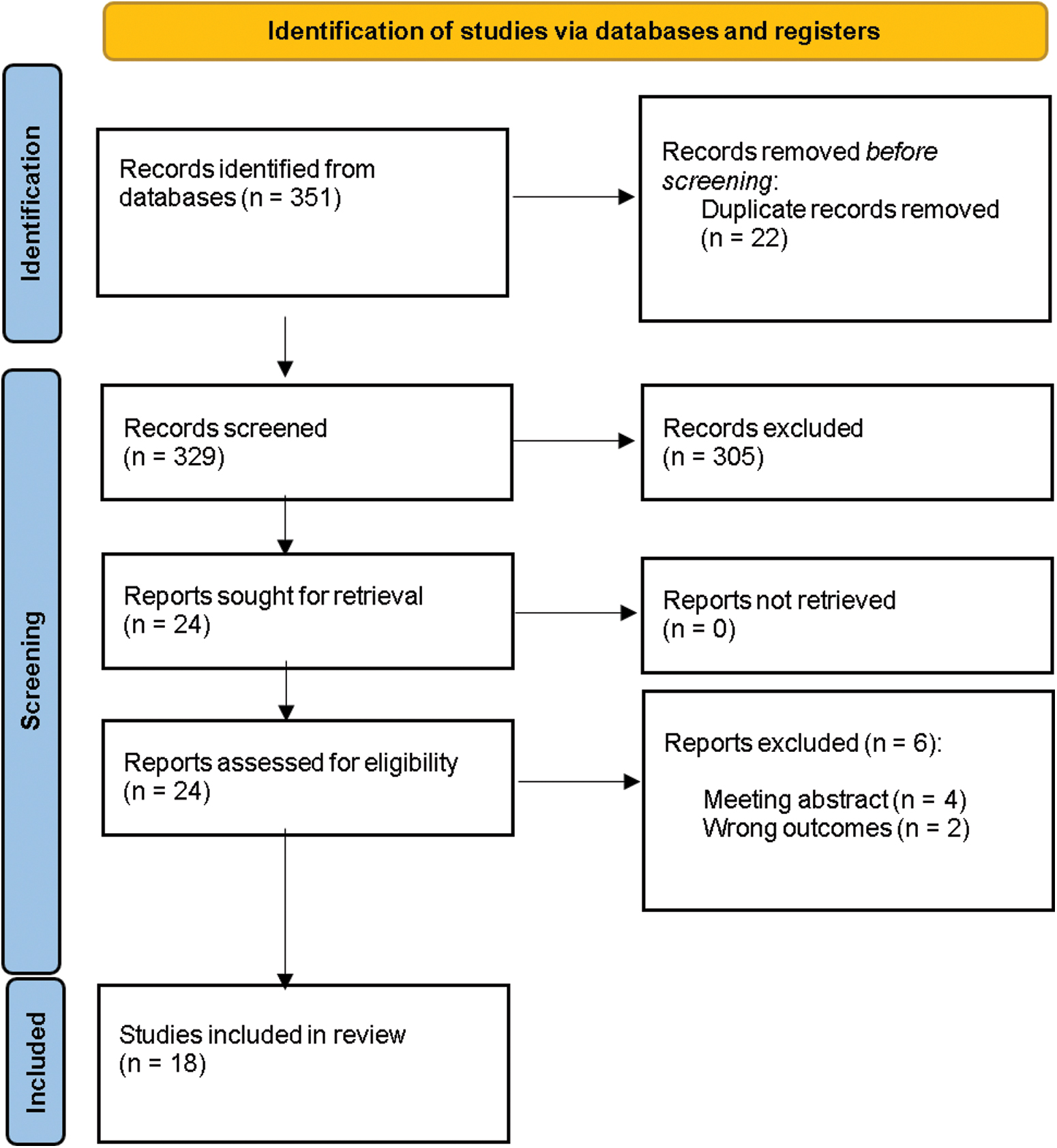
PRISMA 2009 flow diagram detailing the search strategy and identification of studies used in data synthesis. Color images are available online.
Study characteristics
There were 17 retrospective studies 11 –16,18 –28 and 1 prospective study. 17 There was one article in French, 24 and the remaining ones were in English. 11 –22,24 –28 The prevalence and management of LUTS owing to BPH and factors affecting the need for operation after kidney transplantation were evaluated in six studies. 11 –16 Regarding surgical techniques, eight studies used TURP, 12 –14,17 –20,22 one study used transurethral incision of the prostate (TUIP), 23 three studies both TURP and TUIP, 24 –26 and the remaining two compared different surgical approaches. 27,28 Six case series reported perioperative outcomes of endoscopic procedure after 1 month of transplantation, 12 –14,17 –19 whereas seven studies 20 –26 reported outcomes within a month. Table 1 provides the study characteristics.
Studies Benign Prostatic Hyperplasia Management in Renal Transplant Recipients
AUR = acute urinary retention; BOO = bladder outlet obstruction; BPH = benign prostatic hyperplasia; CD = Clavien Dindo; GL PVP = GreenLight photoselective vaporization of the prostate; HoLEP = holmium laser enucleation of the prostate; IPSS = International Prostatic Symptoms Score; LUTS = lower urinary tract symptoms; PVR = postvoiding residual; RT = renal transplantation; sCr = serum creatinine; TUIP = transurethral incision of the prostate; TURP = transurethral resection of the prostate; UTI = urinary tract infection.
Discussion
Factors associated with the risk of BPH procedure after kidney transplantation
RT is the preferred treatment for ESKD because of its ability to provide improved survival and better quality of life compared with regular dialysis treatment. With advancements in surgical techniques and immunosuppressive therapy, RT is also offered to elderly people. In fact, in the last two decades, it has become a safe procedure for elderly patients as well, particularly those aged older than 60 years and selected patients older than 70 years. 29 Clinical BPH is more commonly observed in elderly patients as its prevalence increases linearly with age. 30 Furthermore, in men older than 70 years of age, the progressive nature of BPH leads to the symptoms worsening and a decline in voiding function. 31 This association reinforces the need for close monitoring of older transplanted men.
LUTS typically manifest as voiding or storage symptoms. When left untreated, BPH-related complications, including recurrent UTI, and acute urinary retention (AUR), can negatively impact renal graft function, with a progressive decline in renal function, hydronephrosis, and potential graft loss. Therefore, a preoperative full assessment of LUTS and voiding parameters in case of preserved diuresis has been suggested before listing the patient for kidney transplantation. 11
Because most of the kidney transplant candidates are oligo-anuric before transplantation, the screening for BPH should be performed in the first year after RT. Flow/pressure study with measurement of bladder voiding pressure is an appropriate examination to evaluate men with moderate-to-severe LUTS and identify patients with a greater risk of BOO and secondary graft failure, 12 considering that men with BOO are five times more likely to develop graft failure than recipients without it. 13
Recurrent UTIs are an independent risk factor for graft loss and can cause graft pyelonephritis and lead to urosepsis. The incidence of UTIs in BPH patients was reported to be 6.5% and UTIs are associated with high PVR or AUR. 31 Furthermore, in the transplanted recipients, the risk of UTIs is increased because of the presence of the immunosuppressive therapies especially in the first 6 months after transplantation. 32
Chronic urinary retention is another major complication of BOO that can adversely affect the function of transplanted kidneys by turning the bladder from a low-pressure to a high-pressure reservoir. This ultimately leads to vesicoureteral reflux in the graft, despite the presence of an anti-reflux ureteroneocystostomy. BOO can also produce hydronephrosis and pyelonephritis with concomitant graft damage. The incidence of AUR in recipients was 6% to 10% during a 3-year follow-up. 11,14 de Oliveira Marinho et al. reported a similar incidence (4.6%) at an average time of 38.5 days after kidney transplant and identified men aged older than 55 years and poor residual diuresis as risk factors for recurrent AUR episodes. 15
In another study, Gratzke and colleagues 16 reported similar findings and suggested that surgical treatment should be anticipated in elderly patients after kidney transplantation with a long history of dialysis, and the absence of diabetes because these factors were associated with a significantly higher risk of urinary retention necessitating TURP after kidney transplantation. Indeed, diabetes might protect against AUR caused by BPH/BOO, possibly because of altered testosterone biosynthesis in older diabetic patients. They also suggested that younger age in type 1 diabetic patients might provide additional protection against AUR. Medical therapy with α-adrenergic blockers, either alone or in combination with 5α-reductase inhibitors, started before transplantation AUR was associated with a lower risk of AUR. 15
BPH procedure performed after 1 month after renal transplant
BPH procedure after RT is indicated in patients with BOO and acute/chronic urinary retention, particularly in case of recurrent UTIs, but special considerations are required owing to the patient's altered anatomy and immunosuppressed condition, considering that the incidence of UTI after TURP in the general population was reported to be of 4.1%. 33 The time between the RT and endoscopic procedure should be individualized to ensure safe postoperative outcomes.
In the series by Volpe et al., 17 32 patients underwent TURP after a median time of 6 months after RT. Transplanted patients who underwent TURP experienced improvements in their Qmax, International Prostatic Symptoms Score (IPSS; 80% after 6 months), and PVR compared with their preoperative values. Serum creatinine (sCr) levels were significantly lower at 1 and 48 months post-TURP. Compared with a control group of age-matched transplanted patients who did not undergo TURP, patients awaiting TURP had significantly higher sCr levels at 6 months post-transplant, but no significant difference was observed during follow-up, demonstrating that bladder outlet relief improved their graft function. This study also showed that the improvement in sCr levels after TURP was sustained during long-term follow-up.
Ergesi et al. 14 reported the prevalence and management of LUTS in 131 men after RT. Eleven percent of patients complained of LUTS before transplantation, and the rate increased to 47% after 1 year. Eight (5.3%) patients experienced urinary retention because of BOO (with 62.5% of cases occurring immediately after the transplant), whereas 37% of patients developed UTIs within the first year. Nine men underwent TURP during the first year, and 6 (62.5%) had postoperative UTIs. This study confirmed a high prevalence of LUTS/BPH after RT, with an increasing number of men suffering from LUTS within 1 year after RT.
In a study of seven men who required TURP after RT, Gokce and colleagues 18 found that mean preoperative sCr levels significantly decreased from 2.53 ± 0.76 to 1.66 ± 1.12 mg/dL 6 months after TURP.
In the study by Sarier and colleagues, 19 89 TURP were performed in a cohort of 2423 transplant recipients. The average period between RT and TURP was 13 months. In the postoperative period, 12 patients (13.5%) experienced UTIs. After a 1-month follow-up, there was a significant decrease in sCr values and IPSS, an improvement in voiding parameters, and a reduction in PVR. In the long-term follow-up, 11 (12.3%) patients required reintervention because of TURP long-term complications, with 3 (3.4%) cases of bladder neck contracture and 8 (9%) cases of urethral stricture.
Neri et al. 13 assessed 268 male kidney transplant recipients and found that 55 (20.5%) experienced LUTS, with concomitant UTI, dysuria, and BOO in 18, 18, and 19 cases, respectively. The mean time to onset of LUTS from RT was 14.23 months. Patients with LUTS had a trend toward lower graft survival rates than those without them at 1-, 3-, and 5-year post-transplantation. Thirty-four (12.6%) men were treated with α-blockers, whereas 18 (6.7%) underwent TURP. The mean latency time for TURP was 8.43 months. The authors also showed the importance of the timing of TURP on renal function, with a significant improvement in the estimated glomerular filtration rate when TURP was performed less than 6 months from the beginning of the LUTS.
In the study by Righetto and colleagues, 12 a series of 52 transplanted patients aged ≥50 years with BOO diagnosis was evaluated. Among them, 36 underwent TURP after a median time of 9 months from RT. The other 16 were not eligible for procedure and were treated with α1-blockers and/or 5-ARIs. Three months after the operation, patients experienced significant improvements in IPSS, Qmax, and PVR, with a decrease in their sCr levels. Patients who underwent TURP earlier had better kidney function than those with delayed procedure. Men who underwent the procedure showed a better estimated glomerular filtration rate than patients treated with medical therapy, although no significant difference at 36 months from procedure occurred.
BPH procedure performed within 1 month after renal transplant
Considering the frequent difficulty of BOO diagnosis in oliguric patients waiting for RT and the high incidence of LUTS/BPH after transplant, some clinicians have considered offering BPH procedure very soon after RT, as the detrimental effect of BOO can occur early after diuresis restoration.
Reinberg et al. 20 conducted a retrospective study back in the 1990s to evaluate the outcomes of TURP in eight patients within 10 days of RT. TURP was associated with a 25% rate of major infective complications, including one death. The authors concluded that TURP can be safely performed in transplanted men with sterile urine and under antibiotics therapy.
In a study by Koziolek and colleagues 21 evaluating 11 RT recipients older than 55 years, 8 (72.7%) had concomitant BPH detected using the IPSS. All patients experienced an episode of AUR and were treated with α-receptor antagonists and, subsequently, underwent TURP. No postoperative complication was present in all cases. The IPSS score significantly increased, and BOO improved with increased uroflowmetry parameters after the procedure. They concluded that TURP should be offered in patients with an IPSS score >15 or after an AUR episode.
In 2009, Tsaur et al. 22 conducted a retrospective study on 242 male transplant recipients. Patients were divided into two groups according to a threshold age of 60 (group 1 patients older than 60 years; group 2: patients younger than 60 years). After catheter removal, 27% of patients in group 1 and 19% in group 2 recipients experienced voiding dysfunction. The most common cause was BOO owing to BPH in 25% and 12% of patients in groups 1 and 2, respectively. TURP was performed in 21 group 1 patients (20%) and 14 group 2 patients (10%) at a mean of 31.1 and 29.5 days after RT, respectively. The authors concluded that early post-transplant voiding dysfunction had a high incidence in older men, and BOO management should be considered in older recipients soon after RT.
Dörsam et al. 23 evaluated 259 men after RT. Fifteen patients (5.8%) developed urinary retention after procedure. Urine cultures were positive in 6 (40%) of 15 patients. These patients underwent TUIP. There was post-TUIP. Median Qmax and PVR significantly improved, and there was no episode of AUR, bladder neck contracture, or perioperative fever post-TUIP, showing that TUIP was a safe and effective alternative treatment for transplant recipients with AUR owing to small-size BPH.
In a study by Védrine and colleagues 24 evaluating 256 transplanted patients, 20 (7.8%) underwent a bladder outlet relief surgical procedure. This procedure included TURP in 12 (60%) cases and TUIP in 8 (40%). Operation was performed after a mean period of 15.2 days after RT. One (5%) patient experienced AUR and required temporary bladder catheterization. Three (50%) of six patients who received targeted antibiotic prophylaxis and had a positive bacteriological examination of urine still developed UTI. Instead, only 1 (7.1%) postoperative UTI episode occurred among the 14 patients with negative urine cultures. No deterioration in kidney function or graft loss was observed. Renal function improved in five patients after prostate procedure. The authors concluded that early TURP or TUIP procedures do not carry an elevated risk of infection with sterile urine before operation.
Mokos et al. 25 conducted a study on 24 patients who had undergone RT and transurethral surgical procedures for repeated BOO (i.e., AUR, elevated PVR with or without UTIs), with an average interval of 16 days between RT and prostate procedure. Nineteen patients (79.2%) underwent TUIP, and the remaining 5 (20.8%) underwent TURP owing to the median prostate lobe. All surgical procedures were performed without any complications, and none of the patients experienced a decline in renal function. In all cases, micturition parameters improved, and PVR was insignificant. Based on their findings, the authors suggested that these surgical procedures should be considered early in patients with repeated BOO who have not responded to medical therapy.
In a study by Sarier et al., 26 38 male patients underwent TURP or TUIP owing to BOO with a median of 19 days from RT. None of the patients required a blood transfusion during the postoperative period. UTI and AUR occurred in 5 (13%) and 2 (5%) patients, respectively. One month after operation, the mean sCr level dropped significantly. Mean Qmax increased. An acceptable urethral stricture (8%) and bladder neck contracture (5%) rate occurred in the long term.
Studies comparing different surgical BPH procedures
In a retrospective series, 27 Sarier et al. evaluated 79 male patients with a prostate volume up to 30 cm3 who underwent TURP (47 cases) or TUIP (32 cases) after RT. The median time between RT and TUIP/TURP was 14 (0–84) months and 19 (0–66) months for TURP and TUIP, respectively. In both groups, a postoperative improvement in Qmax, a reduction in sCr and IPSS, and a decrease in PVR occurred. UTIs and retrograde ejaculation were higher in the TURP group than the TUIP group (12.7% vs 6.2% and 68.1% vs 25%, respectively), whereas the urethral stricture incidence was more prevalent after TUIP (12.5% vs 6.3%). The authors affirmed that TUIP should be the preferred surgical option over TURP for sexually active patients, particularly younger ones, interested in preserving ejaculation.
Prudhomme et al. 28 reported the surgical management of BOO after RT in three centers with a 1-year follow-up comparing different surgical procedures. TURP, holmium laser enucleation of the prostate (HoLEP), and GreenLight photoselective vaporization of the prostate (GL PVP) were performed in 34, 17, and 9 cases, respectively. The median time between RT and BPH surgical procedures was 10.6 months, with the HoLEP group having a significantly longer time (64.5 months) than the other two groups. The HoLEP group had a significantly higher overall postoperative complications rate than the GL PVP and TURP groups. Although the incidence of early postoperative complications was similar across groups, the 1-year follow-up revealed a significantly higher rate of complications in the HoLEP group. Specifically, UTI occurred in 29.4% patients in the HoLEP group, compared with 0 cases in the GL PVP and TURP groups.
AUR necessitating bladder catheterization was experienced with a higher frequency in the HoLEP group (29.4% vs 0% and 2.9% in the HoLEP, GL PVP, and TURP groups, respectively). As for functional outcomes, the three groups did not show significant differences in the reduction of sCr levels at 3, 6, and 12 months after the procedure and improvement in the uroflowmetric profile. The three procedures demonstrated comparable efficacy, although the safety of HoLEP appeared inferior to that of the other techniques. However, the group that underwent the latter approach had a significantly longer interval between RT and endoscopic procedure. Based on the current evidence of a safer profile of HoLEP over TUR in the general population, we argue that the longer time between RT and BPH procedure in HoLEP patients compared with TURP patients and the small sample size of this study may explain the differences in complication rate between the groups.
Take-home messages
Taken as a whole, the above studies pointed out six key points: (i) the incidence of BPH/LUTS steadily increases after RT; (ii) BOO can be a contributing factor to graft function deterioration and should always be taken into consideration in transplanted men with an unexplained increase in sCr levels; (iii) BOO and AUR can develop soon after RT, even after catheter removal and a pre-RT assessment of LUTS/BPH should be performed in men with pre-transplant preserved diuresis to detect men who will likely develop BOO after RT; (iv) the earlier, the better; when indicated, bladder outlet relief procedure should be performed as soon as possible after RT to avoid further graft deterioration; (v) preoperative sterile urine and antibiotics prophylaxis should be ensured to avoid postoperative serious infectious complications; (vi) data are lacking regarding the best surgical BPH treatment to be offered in kidney transplant men and further studies are indeed required.
Conclusions
Our review provides insight into the surgical treatment of BPH in RT recipients. The sequelae of BOO owing to BPH can deteriorate renal graft function, and this may be unrecognized in oliguric patients with ESKD until recovery of diuresis. Our study also suggests that TURP after RT provides satisfactory functional outcomes associated with an sCr level reduction from pre-BPH procedure. A timing of <1 month between the two procedures may be appropriate in cases of negative urine culture, especially in older patients who tend to develop BOO/AUR more frequently than younger men. Alternatively, TUIP may be recommended for patients with small-sized prostates who wish to preserve anterograde ejaculation. Finally, further studies comparing different surgical BPH procedures are demanded to assess the superiority of the new techniques over traditional TURP and TUIP.
Availability of Data and Materials
The datasets used and analyzed during this study are available from the corresponding author upon reasonable request.
Footnotes
Authors' Contributions
C.G.: Methodology, Writing—original draft, Writing—review and editing. D.C.: Conceptualization, Methodology, Writing—review and editing. V.G.: Writing—review and editing. G.M.: Supervision, V.P.: Writing—original draft. M.B.: Writing—original draft. A.C.: Writing—original draft. A.A.: Writing—original draft. V.D.S.: Writing—original draft. A.R.: Writing—review and editing. A.B.G.: Conceptualization, Project administration, Writing—review and editing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.