
Abstract
Introduction:
There are only a few clinical data on nononcologic procedures performed with the new Hugo™ robot-assisted surgery (RAS) system. Robot-assisted simple prostatectomy (RASP) is a minimally invasive treatment option for benign prostatic hyperplasia, and it demonstrated equal early functional and better perioperative outcomes as compared with open simple prostatectomy. In this article, we reported the first large series of RASP performed with Hugo RAS system.
Methods:
This Supplementary Video S1 is a step-by-step description of two different techniques for RASP. We analyzed the data of 20 consecutive patients who underwent RASP at OLV Hospital (Belgium) between February 2022 and March 2023. Patients baseline characteristics, perioperative and pathologic, and 1-month postoperative outcomes were reported, using the median (interquartile range [IQR]) and frequencies, as appropriate.
Results:
Median age (IQR) and preoperative prostate specific antigen (PSA) were 72 (67–76) years, and 7.7 (5.0–13.4) ng/mL, respectively. A total of 11 patients experienced an episode of preoperative acute urinary retention, and 8 men had an indwelling bladder catheter at the time of the surgery. No intraoperative complication occurred, and there was no need for conversion to open surgery. Median operative and console time were 165 (121–180) and 125 (101–148) minutes. On the first postoperative day the urethral catheter was removed in 80% of the patients. Median length of stay was 3 (3–4) days. Three patients had minor postoperative complications. On final pathology report, median prostate volume was 120 (101–154) g. On postoperative uroflowmetry, median Qmax and postvoid residual were 16 (13–26) mL/s and 15 (0–34) mL, respectively.
Conclusions:
This series represents the first report of surgical outcomes of RASP executed with Hugo RAS system. Awaiting study with longer follow-up, our study suggests that Hugo RAS has multiple applications, and it can ensure optimal outcomes in nononcologic procedures.
Introduction
Simple prostatectomy is indicated in patients with enlarged glands (>80 g) who present with recurrent or persistent lower urinary tract symptoms, acute urinary retention, significant symptoms from bladder outlet obstruction (BPO) not responsive to medical therapy, recurrent gross hematuria of prostatic origin, bladder calculi secondary to obstruction or pathophysiologic changes of the kidneys, ureters, or bladder secondary to prostatic obstruction. 1
Robot-assisted simple prostatectomy (RASP) is a minimally invasive surgical technique first described by Sotelo et al. in 2008 as an alternative to open simple prostatectomy (OSP) for treating benign prostatic hyperplasia. 2 Instead of traditional open surgery, RASP employs a robotic system to remove the enlarged prostate gland through small abdominal incisions.
Studies have shown that RASP offers better perioperative outcomes and equal early functional outcomes compared with OSP, including shorter hospital stay, reduced blood loss, lower risk of blood transfusion, and shorter learning curve. 3,4
RASP is particularly well suited for patients with large prostate glands or for those who have concomitant bladder diverticulum and/or bladder stones. 5,6
Despite these potential benefits, the widespread adoption of RASP is currently limited by a few factors. First, the availability of robotic surgery platforms is still limited in some regions. In addition, the cost-effectiveness of RASP is one of the most important factors involved in the application of this surgical technique. However, recent studies demonstrated that, in the past decade, with the innovation of robotic surgery and the introduction of dedicated robotic training programs, the related costs for robotic surgery might be reduced because of the significantly decreased length of stay, rate of complications, and readmissions. 6 –9
Furthermore, in the coming years the global market for surgical robots is expected to grow, with new companies entering the market, and leading to potential cost savings thanks to less expensive devices and an increased competition between companies. 7,8 In this context, on February 2022, the Medtronic modular multiport robotic system, HUGO robot-assisted surgery (RAS) system, has received the CE Mark approval for urologic, gynecologic, and general surgical procedures in adults. The new HUGO™ RAS consists of a system tower, an open console with innovative hand controllers with a “pistol-like” design and four independent arm carts.
There are limited clinical data on nononcologic procedures performed with the new HUGO RAS system in urology. In this Supplementary Video S1, we describe two surgical techniques of RASP and report the first series of RASP performed with this new robotic platform.
Materials and Methods
Patient population and study outcomes
We analyzed data of 20 consecutive patients who underwent RASP at OLV Hospital (Aalst, Belgium) between February 2022 and March 2023. Procedures were performed by four experienced robotic surgeons using the novel HUGO RAS surgical platform.
Our main goal was to describe step-by-step two different surgical techniques for RASP (anterior and posterior approach). Patients' baseline characteristics, perioperative outcomes, pathologic outcomes, and 1-month postoperative outcomes were reported. Before surgery, all patients with elevated prostate specific antigen levels underwent MRI to exclude the presence of area with Prostate Imaging Reporting and Data System score ≥3 and the need for a prostate biopsy. Complications were prospectively recorded according to the Dindo–Clavien classification. 9 All data are reported using the median (interquartile range [IQR]) and frequencies (proportions), as appropriate. Owing to the low number of procedures, we were not able to compare surgical outcomes between the two different techniques described in the Supplementary Video S1.
Surgical techniques
After general anesthesia, the patients were placed in a supine 25° to 30° Trendelenburg position. The 11-mm endoscope port was placed on the midline above the umbilicus, ∼16 to 18 cm from the target anatomy, as previously described. 10,11 Other two 8-mm robotic ports were placed under vision on a transversal line 5 cm below the optical port and at least 8 cm between each other, and 2 cm away from bony prominences. Then, the fourth arm port is placed on the same plane of the endoscope port, at least 8 cm from the surgeon's left-hand port.
Finally, one 5-mm laparoscopic trocar and one 12-mm AirSeal© system port were positioned in the right hemiabdomen for the bedside assistant (Fig. 1). 12
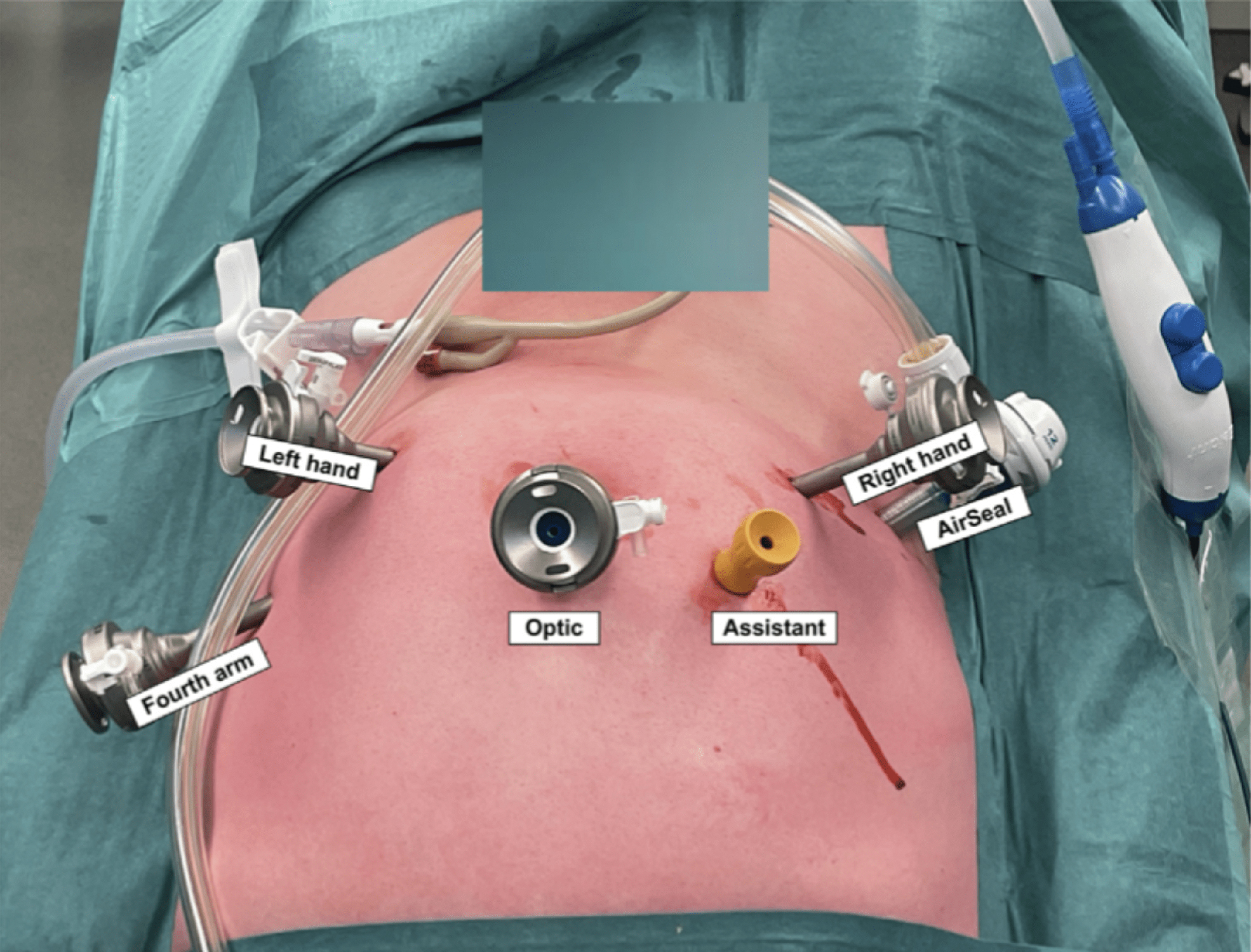
Trocar placement for RASP. The optic trocar is an 11-mm trocar, whereas all the other robotic trocars are 8 mm. The assistant trocars are 5 and a 12 mm AirSeal. RASP, robot-assisted simple prostatectomy. Color images available online.
To guarantee enough space and maneuverability for the bedside assistant, three carts were docked from the left side of the patient and one from the right side. The tilt and docking angles of each cart were already described and are illustrated in Figure 2. 13,14
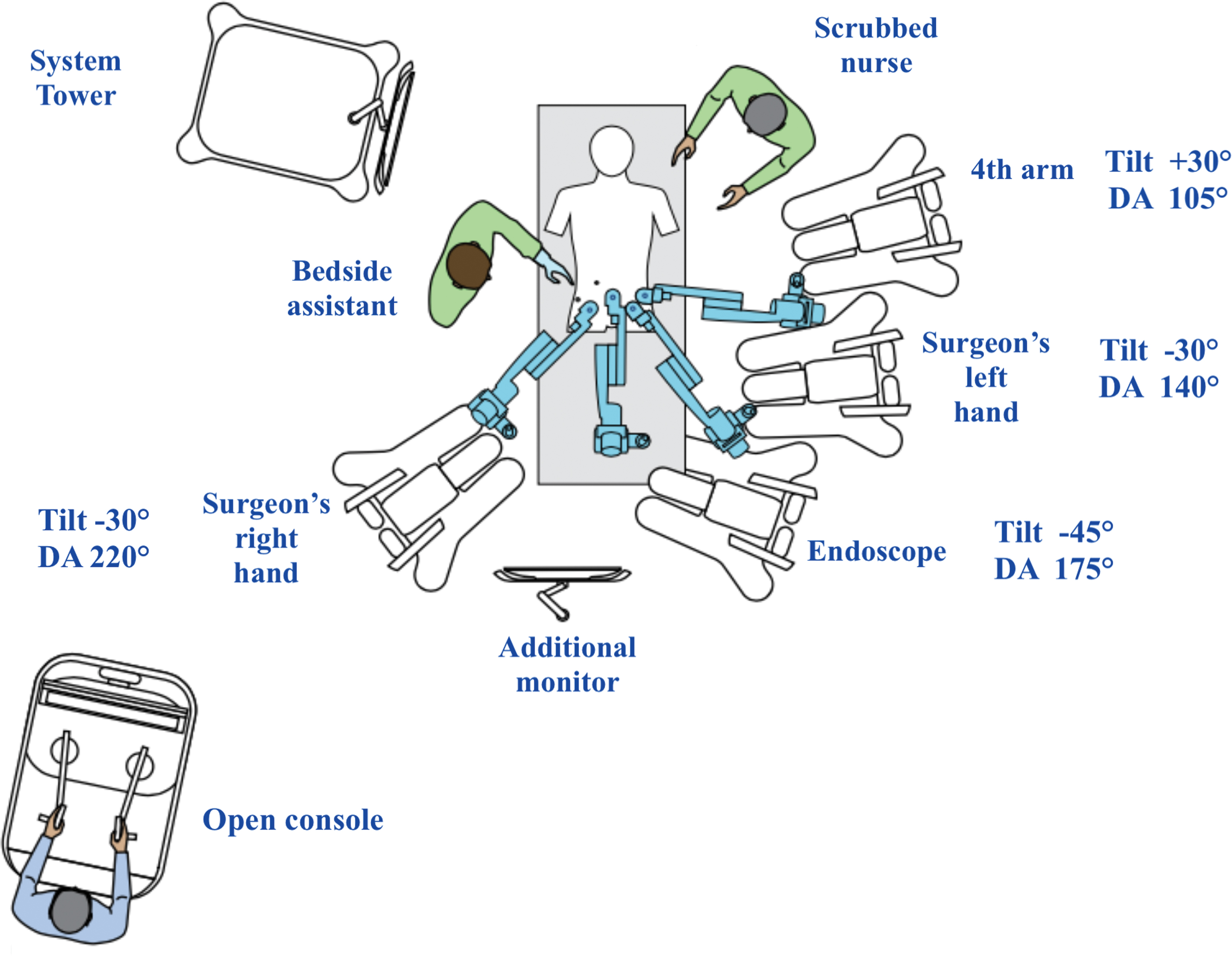
Operating room setting with the positioning, each tilt and DA (Docking Angle) of the four separate cart. DA, docking angle. Color images available online.
All procedures were performed with a 0° lens using three robotic instruments: monopolar curved scissors, Maryland bipolar forceps, or Cadiere forceps and needle driver. For both techniques, the procedures were concluded by removing the specimens from the camera port and closing the robotic ports.
Anterior approach
The first procedure shown in the Supplementary Video S1 is performed using an anterior transperitoneal approach. The medial umbilical ligament is medialized with the nondominant hand, and the peritoneum is then incised where the ligament and vas deferent cross. The paravesical space is carefully dissected until the endopelvic fascia is exposed. This procedure is repeated bilaterally, and finally, the urachus is coagulated and cut. The bladder is opened with a longitudinal cystostomy starting at the level of the prostate-vesical junction. Eventual concomitant bladder stones are removed in this phase through the cystostomy. For better exposure, the two edges of the bladder can be fixed to the abdominal wall using two extracorporeal straight needles. A traction stitch can be placed in the middle lobe to increase exposure. The bilateral ureteral orifices must be identified to avoid injury.
The plane between the prostatic adenoma and the pseudocapsule is developed using sharp and blunt dissection, starting from the 6 O'clock position to the right lobe and then repeating the same procedure to the left lobe. Finally, the prostatic urethra is transected at the apex, and the adenoma is completely dissected. Then the prostatic fossa is carefully inspected for hemostasis, obtained with bipolar or monopolar electrocoagulation, and for any remaining adenoma nodules. A single-layer 3-0 V-loc running suture is utilized to re-trigonize the prostatic fossa, running from the urethra to the bladder neck.
At the end of the procedure, a three-way catheter with continuous irrigation is placed, and the cystotomy is closed using a double-layer 3-0 V-loc running sutures, the first layer incorporates the bladder mucosa, whereas the second layer incorporates all the detrusor muscle. To ensure the integrity of the cystorrhaphy, a watertight closure test is performed at the end with 180 mL of saline.
Posterior approach
The second procedure is performed with a posterior approach. The procedure begins with a posterior midline cystostomy of ∼3 cm. Bladder retraction is achieved using three stay stitches: two for the edges of the bladder and the last one for retraction of the catheter. Before beginning the enucleation phase, bilateral ureteral orifices must be identified to prevent injury.
The bladder neck is incised at the 6 O'clock position to expose the prostatic adenoma. The plane between the prostatic adenoma and the pseudocapsule is developed using both sharp and blunt dissection. The plane is developed circumferentially on both the right and left sides until the apex is reached. After complete dissection of the prostatic adenoma, the prostatic fossa is carefully inspected for hemostasis, and four to six single stitches are placed to prevent postoperative bleeding. A three-way catheter with 30 to 40 mL in the balloon and continuous irrigation is positioned in the prostatic fossa. Finally, the cystotomy incision is closed with a single layer of separate full thickness stitches, and a watertight closure test is performed to ensure the integrity of the cystorrhaphy.
Results
The demographic characteristics of our cohort are shown in Table 1. Overall, 17 (85%) procedures were performed with the anterior approach; median age and body mass index were 72 (IQR: 67–76) years and 29 (IQR: 25–31) Kg/m2, respectively. Median preoperative PSA level was 7.7 (IQR: 5.0–13.4) ng/mL.
Patients' Baseline Characteristics
ASA = American Society of Anesthesiology; IQR = interquartile range; PSA = prostate specific antigen; PVR = postvoid residual.
On the preoperative uroflowmetry, the median Qmax and postvoid residual (PVR) were 9.7 (IQR: 6.0–11.8) mL/s and 95 (IQR: 11–334) mL. A total of 11 (55%) patients had an episode of preoperative acute urinary retention, and 5 and 3 men had an indwelling urethral and suprapubic bladder catheter at the time of the surgery, respectively. Four patients had a concomitant bladder stone, and two men had a bladder diverticulum, which were removed in the same procedure. Three out of four patients (75%, n = 15) underwent previous unsuccessful pharmacologic treatments.
Perioperative data and postoperative outcomes are shown in Table 2. Median docking, operative, and console times were 7 (IQR: 5–9), 165 (IQR: 121–180), and 125 (IQR: 101–148) minutes, respectively. No intraoperative complication occurred, and there was no need for conversion to an open or laparoscopic procedure and/or additional ports placement. Median estimated blood loss was 400 (IQR: 313–875) mL. No drainage was placed, and the urethral catheter was removed on the first postoperative day in 80% of the patients. Median length of stay was 3 (IQR: 3–4) days. According to the Clavien–Dindo classification, only minor (grade I and grade II) postoperative complications were observed in three patients (15%).
Perioperative Data and Postoperative Outcomes
On final pathology report, the median prostate volume was 120 (IQR: 101–154) g and one patient was found with an International Society of Urological Pathology (ISUP) group 1 prostatic cancer, pT stage of T1a. The first postoperative follow-up was at 35 (IQR: 27–45) days and the median follow-up was 3 (IQR: 1–6) months. On the postoperative uroflowmetry, the median Qmax and PVR were 16 (IQR: 13–26) mL/s and 15 (IQR: 0–34) mL, respectively.
Discussion
In this article, we report the surgical outcomes of the first large series of RASP using the novel Hugo RAS system.
All the procedures were concluded without technical problems, including conflict among the robotic arms or major issues, in fact our port placement and operating room setting, already described for RASP and radical prostatectomy, allow optimal working space between the robotic arms. 13,14 Moreover, this setting provided more space both on the right and left side of the patient allowing the bedside assistant and scrubbed nurse to easily access all robotic instruments.
One of the main differences between the HUGO RAS system and other robot surgical platforms is the presence of four separate arm carts that must be docked individually. For this reason, longer docking times may be a concern, but literature reports indicate that the docking time for the HUGO RAS system, after the initial cases, is ∼9 minutes, 15 –17 which is similar to the time reported by Broeders and others for the da Vinci system. 18
RASP is becoming a size-independent treatment for the management of BPO caused by a large prostate gland. 4 It is, also, a demanding procedure when done in a minimally invasive manner, as it includes challenging enucleation steps (adenoma dissection) and reconstructive steps (hemostasis of the adenoma fossa and the re-trigonization). However, it allows both short hospital stay and lower blood loss rate, with a low incidence of perioperative complications. 4 Concerning these fundamental aspects, we reported no intraoperative and no major postoperative complications. The reported estimated blood loss for OSP seems to be higher than for RASP 4,19,20 ; this situation is also reflected in the no need of intraoperative transfusion, which compared favorably with the rates seen for laser techniques for similar-sized glands. 21
Compared with data reported in the literature, we reported a shorter length of stay and catheterization time. In our series, in 80% of the patients, the catheter was removed on postoperative day 1, whereas different literature series reported a median time of 5 up to 10 days. 21 –23 This might be attributed both to surgical technique (such as the expertise of all the surgeons, meticulous hemostasis during enucleation, and re-trigonization of the prostatic fossa) and to the hospital postoperative management. The efficacy of RASP is also confirmed, in most researchers, with a significant improvement of the postoperative outcomes in comparison with preoperative values, such as Qmax and PVR, about 18.9 mL/s and 13.3 mL, respectively. 21 –23
Randomized controlled trials have been conducted to compare the effectiveness of RASP with other surgical techniques used to treat benign prostatic hyperplasia. These techniques include holmium laser enucleation prostate (HoLEP) and OSP. The results of these trials have shown that RASP produces similar outcomes to HoLEP and OSP in terms of Qmax, International Prostate Symptom Score, and reoperation rate. 4,22,24 However, it is important to consider certain characteristics associated with each surgical procedure. For example, both HoLEP and OSP carry a risk of bleeding, with an estimated transfusion rate of about 7% to 14%. 25 In addition, OSP may lead to transient postoperative urinary incontinence (up to 10%) and urethral stricture (up to 6%). 26 In contrast, HoLEP is associated with disadvantages such as prolonged urethral instrumentation, a steep learning curve, and longer operative times. 27
In this Supplementary Video S1, we also describe two different surgical techniques for RASP: anterior and posterior approaches. The anterior approach, similar to robot-assisted radical prostatectomy, involves technical phases such as bladder drop and development of the Retzius plane, so it can be preferred in most of the center. However, this approach permits a limited observation of the ureteral orifices and the trigone, and the steep angle of the instrument can make accurate hemostasis and re-trigonization of the prostatic fossa more difficult. 28
In addition, the development of the Retzius plane and bladder detachment can cause the formation of suprapubic adhesions with consequent postoperative complications. 29 In contrast, the posterior approach requires limited pelvic dissection and at the same time allows a broader view inside the prostatic fossa, easier re-trigonization, because of the urethra position with the instruments, and a better hemostasis on the anterior prostatic capsule. 30 Although as described by Mirvald and others in their comparative analysis there are no significant differences between the two RASP approaches in terms of complication rates and postoperative outcomes in the treatment of large prostatic adenomas. 28
The main limitations of this study are the short follow-up time and the limited number of cases, which prevented us from making a meaningful comparison of outcomes between the two different techniques. Further research with larger sample sizes may be necessary to fully evaluate the eventual difference in outcomes of these techniques. In addition, we believe that more studies are needed to compare the surgical outcomes and the cost analysis of RASP between the different new robotic platforms.
Conclusions
This series represents the first report of surgical outcomes of RASP executed with the novel HUGO RAS system. Awaiting further comparative evidence with long-term follow-up, these preliminary results are comparable with those described in the literature for RASP performed with other robotic systems, suggesting that HUGO RAS has multiple potential applications, and it ensures optimal outcomes also in nononcologic procedures.
Footnotes
Authors' Contributions
Methodology, investigation, data collection, formal analysis, and writing—original draft by A.P. Investigation, writing—review and editing, and data curation by M.P. Conceptualization investigation, writing—review and editing, data curation, and visualization by C.A.B. Investigation, validation, writing—review and editing, and visualization by F.P. Investigation, validation, and writing—review and editing by G.S. and M.T. Investigation and validation by M.P.L., E.B., N.F., S.R., and C.C.-R. Supervision and validation by A.I., R.D.G., and A.M. Conceptualization, supervision, and validation by F.G. Review and editing, data curation, visualization, and supervision by G.D.N. All authors read and approved the final version of the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Video S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.