
Abstract
Objective:
To prospectively assess early post-transurethral prostate surgery (TUPS) urinalysis changes and bacteriuria with its clinical relevance.
Methods:
Patients with benign prostate obstruction enrolled for TUPS were prospectively assessed. Patients were assessed at 2, 4, 8, 12, and 24 weeks postoperatively by the dysuria-visual-analogue-scale (DVAS), international prostate symptom scores (IPSS)-quality of life, uroflow, and postvoid residual. Routine urinalysis was performed before discharge and at all visits. Midstream urine culture (MSUC) was performed before discharge, and 4 and 12 weeks postoperatively.
Results:
At final analysis, 152 patients were evaluable. Significant pyuria was reported in 52%, 96.1%, 94.1%, 71.7%, 78.9%, and 52.5% in, before discharge, 2-, 4-, 8-, 12-, and 24-week urinalysis postoperative, respectively. The mean time to nonsignificant pyuria (95% confidence interval [CI]) was 19.1 (17.5–20.7), 20.1 (17.3–22.9), 15.8 (12.8–18.8), and 14 (10.3–17.8) weeks after prostate resection, vaporization, enucleation, and incision, respectively (p = 0.03). Regardless the TUPS technique, half of patients had significant pyuria at 24 weeks postoperative. MSUC was positive in 37/152 (24.3%), 3/152 (2%), 23/152 (15.1%), and 5/152 (3.3%) preoperatively, before discharge, and 4 and 12 weeks postoperative, respectively. Only positive preoperative urine leukocyte esterase independently predicted positive 4-week MSUC (odds ratio 3.8, 95% CI 1.3–11.1, p = 0.013). No significant correlation was found between IPSS or DVAS and positive MSUC, nor between IPSS and postoperative pyuria at different follow-up points (p > 0.05). However, the degree of postoperative dysuria was significantly correlated with postoperative pyuria count by urinalysis at 2 weeks (r = 0.69, p = 0.03), 8 weeks (r = 0.26, p = 0.001), and 12 weeks (r = 0.23, p = 0.004).
Conclusion:
There is a persistent but gradually declining pyuria and microhematuria following TUPS up to 6 months postoperative. An earlier resolution was noted following prostate incision and enucleation. While routine urine analysis screening in these months would be of no clear clinical value, a routine urine culture would be of a reasonable significance at 1 month postoperatively.
Introduction
Sterile pyuria is the persistent finding of white cells in the urine in the absence of bacteria, as determined by means of aerobic laboratory techniques, 1 whereas urinary growth of bacteria in an asymptomatic individual is defined as asymptomatic bacteriuria. 1 Notably, both clinical scenarios frequently do not require active medical intervention. Moreover, the European Association of Urology guidelines strongly recommended not to treat or even screen patients with asymptomatic bacteriuria. 1
Studies of the epidemiology of and risk factors for pyuria and bacteriuria post-transurethral prostate surgery (TUPS) are limited. 2 –5 Persistence of leukocytes and erythrocytes in postoperative urine analyses is claimed to be due to the inflammatory process and the remodeling of the prostatic surface. 1 Regardless the type of approach or energy of TUPS, microhematuria stops before pyuria reflecting the scaring process at the prostatic bed, where vascular and epithelial remodeling is taking place. 6 There is much controversy regarding transurethral urologic surgeries and the risk of developing subsequent urinary tract infection (UTI). 7 After effective TUPS, lower urinary tract symptoms (LUTS) may be still present in 5% to 35% of patients. 8 The most common cause of this persistent symptom is detrusor overactivity, 9 but this also could be attributed to UTI, 10 which affects postoperative voiding pattern.
Studies analyzing the post-TUPS urine microbiologic and chemical changes are relatively poor, retrospective, and showed many limitations. Factors affecting its persistence and time to normalization have not been established yet. Furthermore, follow-up strategy was heterogeneous and inconsistent. Eventually, the available literature has not reported clinical correlation of the postoperative urinalyses' findings to different urinary outcome measures. The current study aims at the prospective assessment of post-TUPS urinalysis changes and its clinical relevance. Furthermore, its relation to post-TUPS bacteriuria with its predictors is analyzed.
Patients and Methods
Study design
Study design, a prospective cohort study.
After Institutional Reviewer Board (IRB) approval (MS/17.12.91), patients presented for TUPS at a prostate unit between January 1, 2018, and December 30, 2018, and were assessed for inclusion criteria. Eligible patients were asked to participate in this study and were asked to sign an informed consent form.
Study population
Patients were included if they have treatment refractory benign prostatic hyperplasia (BPH)/LUTS with International Prostate Symptom Score (IPSS) >15 and peak urinary flow rate (Qmax) <15 mL/sec or patients with urine retention secondary to BPH who failed trial of voiding. Exclusion criteria include concomitant urinary tract pathology (except bladder stone) and active UTI.
Preoperative workup
Preoperatively, patients were routinely assessed by history and examination, including digital rectal examination, prostate-specific antigen, urinalysis and urine culture, international index of prostate symptom score (IPSS), quality of life (QOL), transrectal ultrasound measurement of prostatic volume and biopsy whenever indicated, measurement of postvoid residual assessment (PVR), and maximum urinary flow rate (Qmax). Preoperative flexible urethrocystoscopy was done when hematuria was the presenting symptom. Patients with positive urine culture were treated accordingly preoperatively. A single dose of intravenous prophylactic antibiotic (1 gm ceftriaxone) was given 1 hour before surgery, unless indicated by a previous urine culture result.
Intervention
Type of TUPS was decided based on surgeon preference, experience, patient and prostate assessment either prostate resection using monopolar or bipolar technique, prostate enucleation using laser or electrosurgical current, prostate vaporization laser or plasma and prostate incision Transurethral incision of the prostate. All patients were discharged from the hospital after an effective trial of voiding, oral ciprofloxacin 500 mg bis in die, twice a day for 10 days was given and stool softener unless otherwise indicated by urine culture. No empirical antibiotics were given afterward until proven by urine culture.
Postoperative workup
Patients were assessed at 2, 4, 8, 12, and 24 weeks postoperatively by the dysuria-visual-analogue-scale (DVAS) (a visual measurement instrument that tries to measure dysuria across a scale from 0 to 10), IPSS-QOL, uroflow, and PVR. Routine urine analysis (dipstick and microscopy) was performed before discharge and at all visits. Midstream urine culture (MSUC) was performed before discharge, and 4 and 12 weeks postoperatively.
Outcome measures
Postprostatectomy urine findings as depicted by routine urine analysis
Tracking of post-TUPS depictable urine blood cells, pyuria (WBCs >5/HPF), microhematuria [red blood cells (RBCs) >3/high power field (HPF)], 11 and other urinalysis changes over time. Time to event analysis will be carried out, looking for time to Non significant pyuria (NSP) nonsignificant pyuria (nonsignificant pyuria 5 or less WBCs/HPF) per urinalysis post-effective TUPS for benign prostate obstruction (BPO). Predictors of persistent significant pyuria till the last reported follow-up (24 weeks) were assessed. Correlation analysis for the depictable urinalysis findings and post-operative dysuria (DVAS 0–10) and/or LUTS postoperatively was performed.
Postprostatectomy microbiologic findings
Postprostatectomy microbiologic findings as identified by MSUC. A colony count of 105 CFU/mm was considered clinically significant. 12 Patients with positive MSUC were treated accordingly. Furthermore, predictors of significant bacteriuria at different time intervals postoperatively as identified by MSUC will be assessed.
Data analysis
Data were collected into the IBM SPSS20 program (social package for statistical sciences, IBM Corporation, Armonk, NY, USA). The mean (± standard deviation) or median (range) as indicated for all continuous measures and scores was recorded at baseline and at all subsequent visits. Results were compared between treatment groups using the chi-square test for categorical variables and the Student's t-test or Mann–Whitney test for quantitative variables. Binary logistic analysis with backward elimination using the likelihood ratio was used for multivariate analysis. Time to NSP will be tested using the Kaplan–Meier method with the log-rank test for assessment of potential predictors. Correlation analysis was performed using Spearman's test.
Results
Out of 195 patients, 187 patients met the inclusion criteria and were eligible for participation in the study, 152 patients were evaluable in the final analysis (Fig. 1). Baseline criteria of studied subjects and type of intervention are depicted in Table 1.
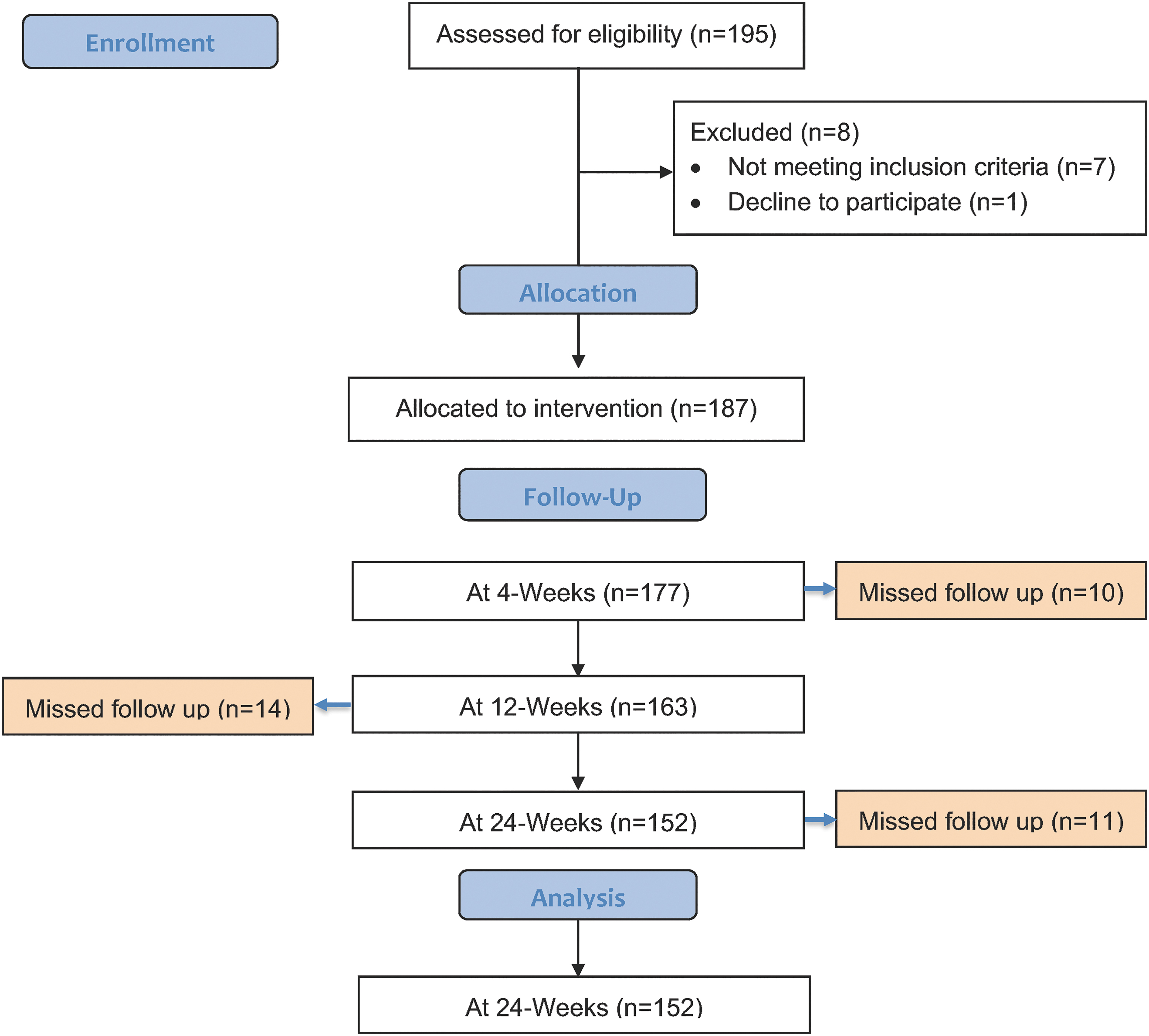
Flowchart for study subjects.
Baseline Characteristics
BMI = body mass index; IPSS = International Prostate Symptom Scores; PSA = prostate-specific antigen; PVR = postvoid residual; Qmax = peak urinary flow rate; QOL = quality of life; SD = standard deviation; TRUS = transrectal ultrasound.
Figure 2 depicts serial perioperative and follow-up changes in microscopy and dipstick urinalysis. Significant pyuria was reported in 52%, 96.1%, 94.1%, 71.7%, 78.9%, and 52.5% in, before discharge, 2-, 4-, 8-, 12-, and 24-week urinalysis postoperative, respectively. The median WBCs/HPF at 24 weeks was 10 (0–100). Microscopic hematuria was reported in 96.7%, 92.1%, 90.8%, 73%, 62.5%, and 55.3% in, before discharge, 2-, 4-, 8-, 12-, and 24-week urinalysis postoperative, respectively. The median RBCs/HPF at 24 weeks was 5 (0–35). Significant pyuria (>5 HPF) at last depictable follow-up (24 weeks) was reported in 80 patients (52.6%) and none of the studied factors was a significant predictor (Table 2). However, mean time to NSP (95% confidence interval [CI]) was 19.1 (17.5–20.7), 20.1 (17.3–22.9), 15.8 (12.8–18.8), and 14 (10.3–17.8) weeks after prostate resection, vaporization, enucleation, and incision, respectively, p = 0.03 (Fig. 3).
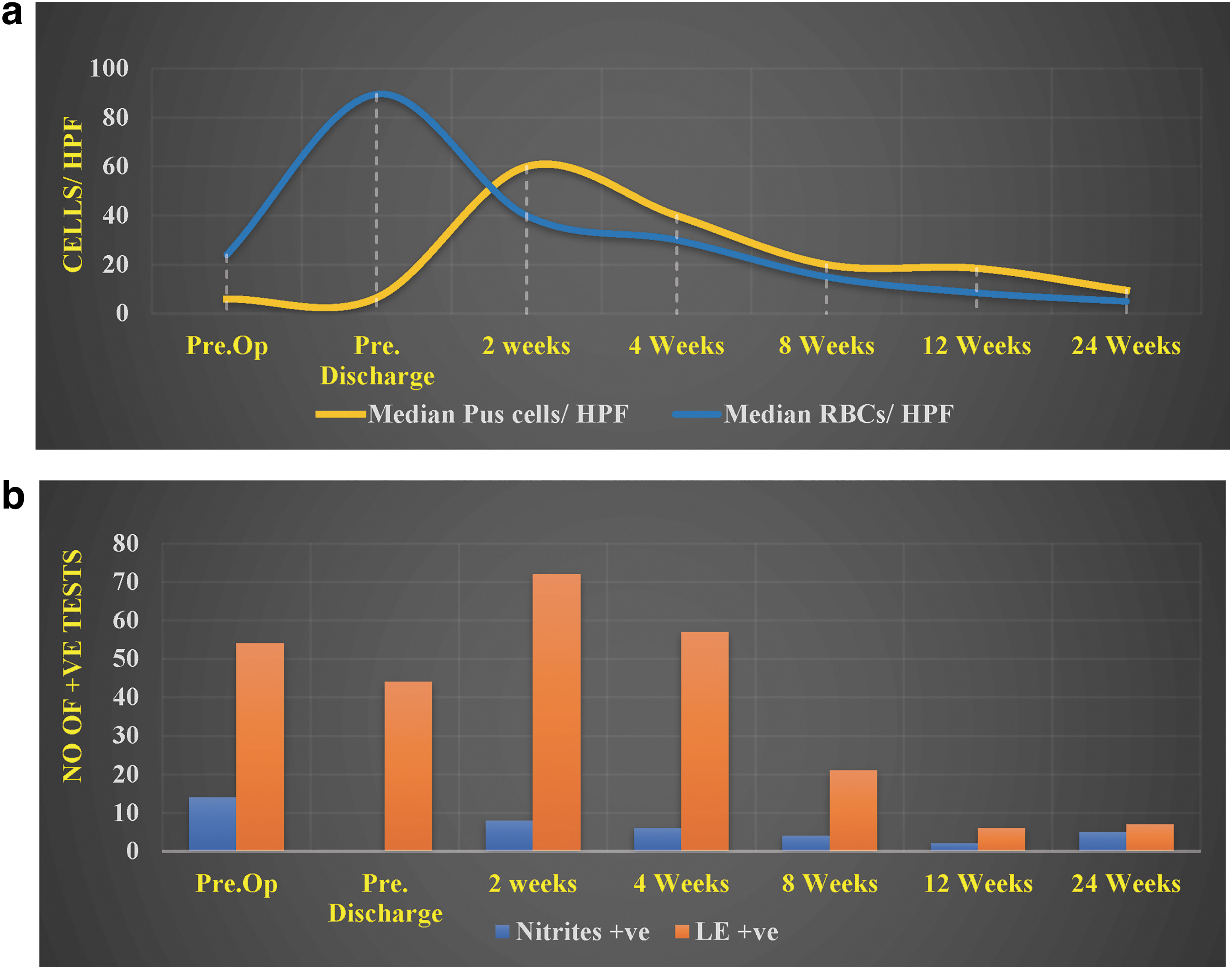
Perioperative urinalysis.
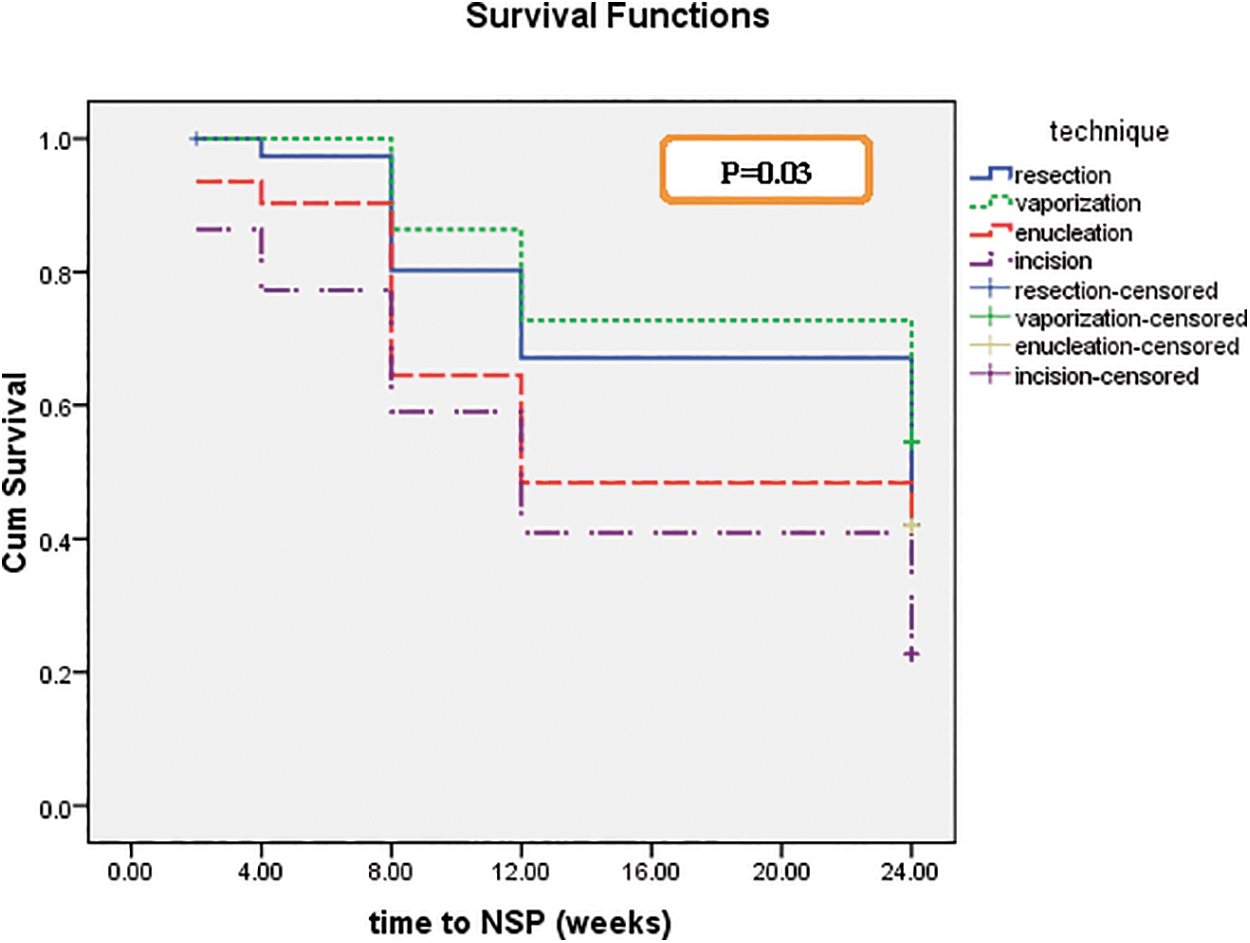
Time to nonsignificant pyuria [5 or less white blood cells (WBCs)/high power field (HPF)]. NSP, non siginficant pyruria; WBC, white blood cells.
Potential Predictors for Persistent Significant Pyuria
HPF, high power field; LE = leukocyte esterase; MSUC = midstream urine culture.
The time was significantly less following incision compared with resection (p = 0.013) and vaporization (p = 0.012) and was not significant considering enucleation (p = 0.6). No significant correlation was found between IPSS and postoperative pyuria count by urinalysis at different follow-up points (p > 0.05). However, the degree of postoperative dysuria (DVAS) was significantly correlated with postoperative pyuria count by urinalysis at 2 weeks (r = 0.69, p = 0.03), 8 weeks (r = 0.26, p = 0.001), and 12 weeks (r = 0.23, p = 0.004). No significant correlation was found between DVAS and postoperative pyuria count by urinalysis at 4 and 24 weeks.
MSUC was positive in 37/152 (24.3%), 3/152 (2%), 23/152 (15.1%), and 5/152 (3.3%) preoperatively, before discharge, and 4 and 12 weeks postoperative, respectively. On univariate analysis, positive preoperative urinalysis leukocyte esterase (LE), positive 4-week urinalysis LE, nitrite, and significant pyuria, and positive preoperative and before discharge MSUC were significant predictors for positive 4-week MSUC (Table 3). On multivariate analysis, only positive preoperative LE independently predicted positive 4-week MSUC (odds ratio 3.8, 95% CI 1.3–11.1, p = 0.013). On univariate analysis, positive preoperative LE, positive 12-week urinalysis LE, nitrite, and significant pyuria, preoperative indwelling catheter, and positive 4-week MSUC were significant predictors for positive 12-week MSUC (Table 3). On multivariate analysis, none of the reported variables significantly predicted positive 12-week MSUC. No significant correlation was found between IPSS or DVAS and positive MSUC at different follow-up points (p > 0.05).
Potential Predictors (Univariate Analysis) for Positive Midstream Urine Culture
Bold values signifies statistical significance.
Discussion
Urinalysis is a simple test that is frequently used in clinical practice. Nevertheless, urine culture remained the gold standard test for diagnosis of UTI. The European association of urology (EAU) and American association of urology (AUA) guidelines lack recommendations on the utility of both urinalysis and urine culture following transurethral procedures for BPO. 13,14 The natural history of urine analysis changes postprostatic intervention is poorly investigated in the urologic literature. Olvera-Posada et al. found that after TUPS pyuria persists longer than microhematuria regardless of the type of surgery, the weight of resected tissue predicted persistence of pyuria. 15 Herein, Figure 2a starting from postprocedure 2nd week's urinalysis showed microhematuria less reported than pyuria with parallel decline till the 24th week urinalysis.
The current study did not define predictors for persistent significant pyuria following TUPS, including positive urine cultures. Notably, the pending concern is time to NSP, when the patient and his treating doctor stop rattling for leukocyturia. In the current study, we found that mean time to NSP was 19.1, 20.1, 15.8, and 14 weeks following prostate resection, vaporization, enucleation, and incision, respectively, which was significantly in favor of prostate incision that represents the least invasive surgical intervention. Similarly, Yang et al. reported a significantly longer pyuria period after diode laser vaporization of the prostate in comparison with transurethral resection of the prostate (TURP) (16 vs 12 weeks, p = 0.0014). 16
These data strongly provide evidence that the degree and duration of postprocedure leukocyturia are not related to an active infection but rather to the degree of prostatic urethral inflammation and the resulting raw surface area with the subsequent progressive healing process. Thus, routine antibiotic prescription for this finding would be injurious in terms of increasing bacterial resistance without an apparent benefit. We would clearly vote against routine urine analysis screening in these patients in the first few postprocedure months.
Postoperative bacteriuria would be secondary to an ascending colonization along the urethral catheter, secondary to disconnection of closed urinary drainage system 5 or due to breaching of improperly treated intraprostatic infection. 17 El Basri et al., in a study of post-transurethral procedure bacteriuria, reported positive MSUC at 4 weeks in 7.6% of patients and only 1.9% had symptomatic UTI. 18 Huang et al. reported 18.2% positive MSUC during the first 4 weeks after bipolar TURP. In their study, there was no significant correlation between bacteriuria and pyuria and only longer operating time (>60 minutes), longer postoperative catheterization (>3 days), and disconnection of the closed urine drainage system independently predicted positive MSUC. 5 Colau et al. reported a post-TURP bacteriuria rate of 8%, 14% and 5% on catheter removal, 10th postoperative day, and 4 weeks postoperative, respectively. Longer operating time and disconnection of the closed urine drainage system independently predict post-TURP bacteriuria rate. 3
In the current study, periprocedural prophylaxis was carried out according to the recommendations of Berry and Barratt's meta-analysis that showed the greatest relative risk reduction for bacteriuria when using third-generation cephalosporins and quinolones. 19 Nevertheless, positive MSUC was depicted in 23/152 (15.1%) and 5/152 (3.3%) 4 and 12 weeks postoperative, respectively. Neither preoperative clinical features, type of procedure, nor postoperative pyuria predicted the postoperative MSUC. Positive preoperative urinalysis LE independently predicts positive MSUC. The relatively high reported yield of postoperative 4-week MSUC would impact routine practice. We would advise to include a routine urine culture rather than urine analysis at 1 month postoperatively particularly in patients with positive preoperative urinalysis LE.
These data suggest urine LE as one of the underestimated urinalysis findings if compared with pyuria count that hassles the patient and treating physician. Yang et al., in a matched finding, found no significant correlation could be depicted between clinical UTIs and pyuria. 16
Effective transurethral treatment of BPH aims subjectively at relief of voiding LUTS and objectively at normalization of uroflow and PVR. However, residual post-transurethral prostatectomy storage LUTS and/or dysuria would urge the patient and urologist for further assessment and care. This would have negative implications on patient's QOL and health care resources. In this investigation, postoperative dysuria was significantly correlated with postoperative pyuria count by urinalysis at most of the time intervals. This indicates that postoperative pyuria should not be interpreted as possible infection but should be perceived as a pronounced postoperative inflammatory reaction and might be treated by anti-inflammatory medications rather than empirical antibiotics.
Surprisingly, positive postoperative MSUC did not predict postoperative dysuria. Interestingly, residual postoperative LUTS as evaluated by IPSS was not predicted either by pyuria or by postoperative positive urine cultures. We do believe that these patients would improve by anticholinergics or B3 agonists to control the irritative bladder symptoms.
This study has certain limitations that include a small sample size and a limited follow-up to 24 weeks. We believe that if we prolonged the follow-up, a more solid conclusion about the time to NSP could be attained. However, to the best of our knowledge, it is the first prospective study to include four different techniques for transurethral treatment of BPO. Furthermore, we used a well-designed approach for the assessment of the procedure-related outcome both subjectively and objectively in relation to serial urine microbiologic as well as urinalysis changes.
Conclusions
There is a persistent but gradually declining pyuria and microhematuria following TUPS up to 6 months postoperative. An earlier resolution was reported following prostate incision and enucleation. While routine urine analysis screening in these months would be of no clear clinical value, a routine urine culture would be of a reasonable significance at 1 month postoperatively. Postoperative dysuria is probably best treated by anti-inflammatory medications, while residual postoperative LUTS is probably best treated by control of overactive bladder symptoms. These recommendations are to be further confirmed in future studies.
Footnotes
Authors' Contributions
A.M.E.: Article writing and data analysis. K.A.A.: Patient follow-up and data collection. A.E.A.: Data analysis and literature review. A.N.: Critical supervision. Y.O.: Critical supervision and article writing.
IRB Approval
Approval of the research protocol by an IRB (MS/17.12.91).
Informed Consent
Eligible patients were asked to sign an informed consent form.
Author Disclosure Statement
Nothing to disclose.
Funding Information
The study is funded by the hosting institution (Urology and Nephrology Center). Grant number MS/17.12.91.